
Abstract
BACKGROUND:
Coffin-Siris syndrome is a rare genetic disease with heterozygous variants in the ARID1A, ARID1B, ARID2, DPF2, SMARCA4, SMARCB1, SMARCE1 or SOX11 genes. It may manifest with somatic anomalies, deafness, urogenital malformations, recurrent infections, mental retardation, speech deficit, agenesis of the corpus callosum, convulsions, hypotonia, developmental delay, and scoliosis.
CASE REPORT:
A 14-year-old boy with Coffin-Siris syndrome due to variants in the ARID1A gene was referred to the clinic. His rehabilitation over a 9-year period was described. The problem of assessment and the approach to rehabilitation was discussed, enabling a progressive remodelling of the cognitive-behavioural disorders that most hindered the possibility of his acquiring new skills and achieving social and family integration.
CLINICAL REHABILITATION:
A protracted, customised, multiprofessional rehabilitation approach, centred on realistic functional objectives, implemented with the direct involvement of the family and school, was the only way to achieve the maximum independence and social and family integration permitted by his residual disability.
Introduction
Coffin-Siris syndrome is a very rare genetic disease. About 200 confirmed cases in the whole world have been described [1]. The exact prevalence and incidence are not known, although it is thought that diagnosis may be underestimated. All reported cases have been sporadic. In some patients it has been possible to detect pathogenic heterozygous variants in the ARID1A, ARID1B, ARID2, DPF2, SMARCA4, SMARCB1, SMARCE1 or SOX11 genes. Variants in these genes have autosomal dominant inheritance, although most cases seem due to de novo mutations. The syndrome remains without molecular confirmation in about 10% of cases. Although clinical variability is high, diagnosis is based on genetic testing, which is of fundamental importance, and on one major and at least one minor clinical sign. Major signs include fifth digit anomaly, deafness, joint laxity, urogenital and renal malformations, recurrent infections and mental retardation [2] which may be associated with speech deficit, hirsutism, coarse facial features, and low-set malformed ears. In some cases there may be clinodactyly of the fifth digit or hypoplasia of the distal phalange of the second, third and fourth toe. Minor signs include: Dandy-Walker malformation, cortical gyral simplification, agenesis of the corpus callosum [3], convulsions, [4] and hypotonia. Developmental delay and scoliosis manifest in the neonatal period or during infancy [5].
Case report
Clinical assessment
The boy, an only child of parents of Caucasian race, was referred in 2011 at age 14 years. He showed facial and ear malformations (Fig. 1 and 2) and scoliosis (Fig. 3), severe behavioural disorders including aggressiveness, wandering, compulsive stereotyped motor activity and accentuated attention deficit. He handled objects for a few seconds, rapidly losing interest. He had no apparent visual defects. Severe impairment of verbal production with unstructured language was evident. He had some communication signs for primary needs, sphincter continence, and was largely dependent on others for activities of daily living. Family history showed no evidence of consanguinity. The mother had an obstetric history that included three miscarriages. The baby was born at term (38 weeks) after a normal pregnancy with birthweight 2950 g, Apgar 8 at 1 minute after birth and right microtia. Perinatal ultrasonography showed agenesis of the corpus callosum. Episodes of convulsions during fever occurred at 3 and 6 years of age but the child was not subsequently treated with antiepileptic drugs. Bilateral orchiopexy was performed at age 4 years. The child suffered recurrent respiratory infections with two episodes of pneumonia. He was treated with hormone replacement at 17 years for suspected Hashimoto thyroiditis. Annual ECG, echocardiogram and EEG were within normal limits. Spinal x-ray showed severe dorso-lumbar scoliosis (40° Cobb). Cranial NMR showed dysgenesis of the corpus callosum (Fig. 4).

Facial malformations (published with parental consent).

Ear malformation (published with parental consent).
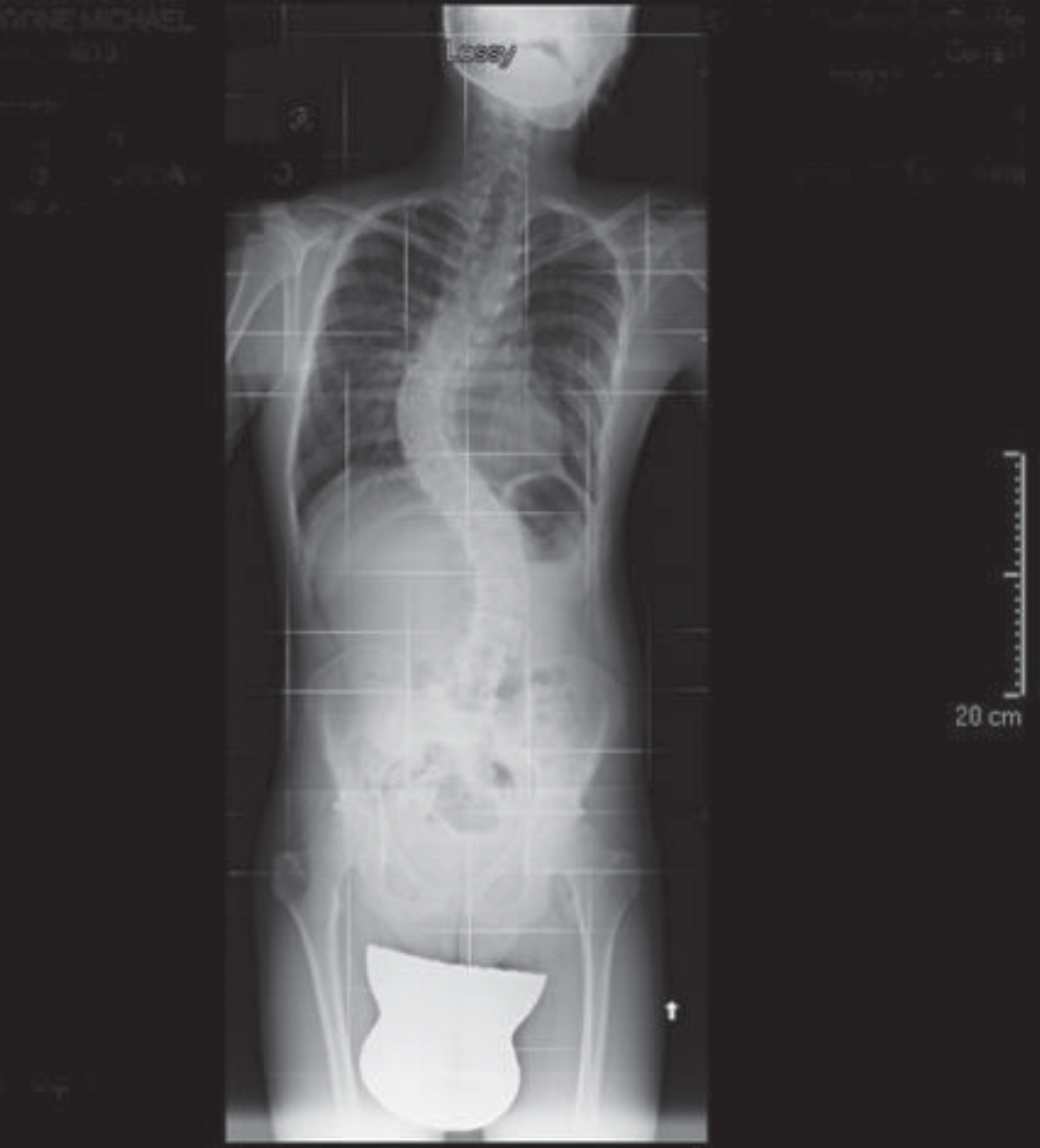
Scoliosis (published with parental consent).

Brain NMR - dysgenesis of corpus callosum (published with parental consent).
In 2018, a variant in the ARID1A gene was detected by Next Generation Sequencing (NGS) and confirmed to be a de novo mutation by Sanger sequencing. The patient was diagnosed with Coffin-Siris syndrome. Analysis of genetic variants in the proband and parents was conducted by PCR and direct sequencing in the region (GRCh37/hg19) chr 1:27,094,373-27,094,640. The patient showed a heterozygous variant in ARID1A (GRCh37) chr1:27094442C > A NM_006015.5:c.3150 > A, p.(Asp1050Glu) that was absent in his parents.
The gene ARID1A encodes a protein involved in gene activation/repression by chromatin remodelling (AT-rich interactive domain-containing protein 1 A). Defects in this gene have been linked to Coffin-Siris syndrome with autosomal dominant transmission. According to ACMG guidelines [6], the variant p.(Asp 1050Glu) is classified as probably pathogenic (class 4).
In 2011, when the patient was consigned to the care of a multiprofessional rehabilitation team (neurologist, physiatrist, neuropsychologist, occupational therapist, psychomotor therapist and educator), he was difficult to engage along with being hyperactive and sometimes aggressive. Despite considerable difficulty in daily management, the parents did not authorise administration of psychiatric drugs. Since it was impossible to work at the table, multidisciplinary neuromotor and psychomotor rehabilitation were addressed in the gym where the initial objectives were to keep the patient in the room, in the proposed setting and to generalise some simple strategies of functional movement. The actions were broken down into components and the outcome measured using the Goal Attainment Scale (GAS) [7] (Table 1) at 3, 6, 9 and 12 months (T1, T2, T3, T4).
Goal Attainment Scale (GAS)
Goal Attainment Scale (GAS)
Scoring: +2 = much more than expected; +1 = somewhat more than expected; 0 = Patient achieves expected level; –1 somewhat less than expected; –2 = much less than expected. Timing: T1: first trimester; T2: second trimester; T3: third trimester; T4: fourth trimester.
To increase attention span and independence in a sheltered environment, a setting was used in which the patient had to recognise the photos of the operators and associate them with the various activities, memorising the path to the various therapy rooms. Direct observation of communicative skills showed an expressive component limited to simple vocal sounds, whereas the verbal and contextual understanding proved to be functional to the requests. Regarding behaviour, the rehabilitation program was aimed at reducing problematic behaviour, stereotyped movements, impulsivity and distractibility with frequent recourse to transitional object. The parents were enlisted from the start in weekly support and training sessions, to overcome daily problems, provide facilitation, and generalise simple strategies decided with the team [8–10]. Initially, parental stress was assessed with the QRS-GFD questionnaire [11, 12] and at discharge. No significant difference with respect to the mean was found in any of the scales (Parent and family problems, Pessimism, Child characteristics), although qualitative analysis of the results showed an increase in attention and in social-family integration perceived by the parents.
In 2013, a first simplified formal neuropsychological assessment using the Leiter-R scale became possible [13] (2). Assessment of adaptive behaviour was made with the Vineland scale (Table 3) which was repeated every 3 years to monitor the patient’s progress [14, 15]. The Goal Attainment Scale (GAS) for activities of daily living was repeated once a year from 2013 to 2019 (Table 5).
Vineland scale 2013, 2016, and 2019
Goal Attainment Scale (GAS) Objective: DRESSING years 2013–2019
Scoring: +2 = much more than expected (autonomy); +1 = somewhat more than expected (cognitive reinforcement); 0 = patient achieves expected level (minimal physical and cognitive help); –1 = somewhat less than expected (important physical and cognitive help); –2 = much less than expected (totally dependent). Timing: T1: first trimester; T2: second trimester; T3: third trimester; T4: fourth trimester.
The goal was to improve and increase overall communication, learning, and socially appropriate behaviour, proposing behavioural intervention in a structured environment and personalised settings. The fundamental principles on which the behavioural rehabilitation programme was based are those of the theory of learning and operant conditioning [16]. Behaviour is influenced by setting, to elicit consequences designed to model it according to an established aim and to generalise a positive strategy for the future. It is done by prompting, proposing a clue or facilitation to achieve behaviour that would not otherwise have happened because it had not yet been learned. Fading techniques were used to gradually eliminate the clues and achieve an autonomous behavioural response. Shaping to systematically reinforce behaviours closer and closer to the target was used. Finally, chaining was used which involves breaking down more complex actions to memorise brief sequences, until the actions are carried out in the right sequence.
Chaining, fading, and shaping favour a gradual change in behaviour and increasingly reinforce the stimulus-response links that make up the behavioural chain. The first phase of this rehabilitation was one-to-one. Also, it took considerable time before the boy could be included in group therapy. The approach was adapted for a patient with severe communication disabilities, who first was seen in adolescence. The TEACCH method [17] is one which is flexible and better accepted by parents and teachers, as well as being coherent with the holistic approach of the working group. The patient was also included in individual occupational therapy to increase independence in daily life activities, differentiating the activity into progressively more complex motor sequences such as the activities of dressing and undressing (Table 5), and proposing concrete and practical settings that are more motivating.
Regarding the communicative component, the patient already had a tablet which he occasionally used with frustration and with the help of an operator who supported his arm in choosing the button and in formulating a message which was then interpreted by his parents. To make use of the tablet possible and functional [18], daily practice at home, supervised by the parents, in using the touch screen to see personal photos and videos and to move between grids was necessary. In this way it was possible to use pre-set games with increasing independence and to select one of two activities from a list. Currently, the tablet has become an instrument to express communicative content, music, photos and videos that make it possible to share private events and personal emotions.
These aims were also achieved thanks to use of the Feuerstein “Basic Instruments” method [19, 20], especially the component concerned with the capacity to express and understand the emotions of others.
The patient was gradually included in group activities (cooking, gardening and music workshops), seeking greater collaboration with other users resulting in greater social integration. Over the years of the personalised rehabilitation programme, there were periodic meetings with the teachers to draft the Personalised Education Plan and to sustain the support teacher in promoting integration with companions. Only later was it possible to propose some structured programmes with the supervision and training of the parents, and then introduction to adaptive sports which increased the occasions for socialisation.
However, clinical observation showed improved communicative intention and efficacy in transmitting a message. The adolescent proved to be more amenable to interaction and showed good motivation and collaboration. Episodic memory was fair. He remembered the path between the different rooms and the place of certain objects in the rooms and he observed social rules (e.g., to knock on the door and wait before entering). Obsessive traits were confirmed so that the patient had to exercise strong control. Self-stimulating behaviours persisted.
In 2019, at the end of the direct work with the patient, a cognitive assessment with non-verbal tests, calibrated for age, was repeated with the Leiter-R test [13], and a broader assessment with Raven’s Coloured Progressive Matrices (CPM47) [21]. The Non Verbal Intelligence Test (TINV) [22, 23] was possible for the first time. The Vineland scales [14, 15] were administered for the third time to assess adaptive behaviour, and functional activity was assessed for the last time by the GAS.
Table 1 shows GAS scores for minimal objectives in a rehabilitation setting in the first year of treatment (2011).
Table 2 shows the results obtained in 2013 in a first simplified formal neuropsychological assessment using the Leiter-R scale [13]: Full-scale IQ on the VR battery showed moderate developmental delay and attention and memory deficits (AM scale).
Cognitive assessment 2013 Leiter-R Scale
Cognitive assessment 2013 Leiter-R Scale
Legend: IQ: intelligence quotient.
Also in 2013, a first administration of the Vineland Adaptive Behaviour Scales was possible [14, 15]. Scores were lower than the norm of the composite scale (C, DA, S) and in all domains investigated (Communication, Daily Living and Socialisation) (Table 3).
In 2019, at the end of the direct work with the patient, cognitive assessment with the Leiter scale [13] was repeated, although it was necessary to approximate correction for age, since the youth had exceeded the age limit of the normative data by 2 years. This time, analysis of performance showed that learning delay had worsened in terms of “spatial visualization” and “memory screener” which deteriorated from mild to moderate delay. It also proved possible to administer the test with sufficient sustained attention for about 45 minutes, despite the patient’s being easily distracted by external stimuli. Clear-thinking ability and logical-deductive reasoning, assessed by CPM47 [21], proved to be impaired. Overall intelligence measured by the non-verbal intelligence test TINV [22, 23] was below normal without differences between geometric IQ (QINV-FG) and pictorial IQ results (QINV-IO).
The Vineland scores were lower than the norm of the composite scale (C, DA, S) and in all domains investigated (Communication, Daily Living and Socialisation) (Table 3).
The GAS was administered once a year to monitor skills in activities of daily life. Table 5 shows for example how the activities of dressing and undressing evolved in the course of the rehabilitation period.
The approach to rehabilitation for Coffin-Siris syndrome necessarily extended over many years because the patient was referred late with deteriorating behavioural problems, the parents did not authorise use of psychiatric drugs, and because they often could not attend the intensive therapy since they worked a great distance from the centre. Otherwise it would have been possible to implement an early intensive rehabilitation programme specific for all the developmental milestones from early infancy and adolescence to adulthood [24]. Full psychometric assessment was not possible, especially in the initial phase, due to the degree of cognitive-behavioural and communicative impairment as well as attention deficit. However, the disability profile was significant. Despite the persistence of pathological results in the formal assessment (Table 4), today, the patient shows significant functional improvement regarding activities of daily living, simple housekeeping, self-determination, and social integration in simplified contexts including sport, with good emotional participation. All this combined with good support of the family by the team [25] over a long period, the good resilience [26] and self-efficacy beliefs of the parents [27] and improved self-control of the patient, has enabled serene family life and gratifying new life experiences.
Cognitive assessment 2019
Cognitive assessment 2019
Legend: IQ: intelligence quotient; RS: raw score; CS: corrected score; ES: equivalent score; SS: standard score.
It is important not to give in when faced with cognitive disability typical of genetic pathology which may increase on reaching adulthood, a delicate phase for persons with severe disabilities from early infancy. In these patients, it is necessary to support development and training, favour any possible social-occupational integration, continue to monitor psychophysical well-being, and promote the greatest possible autonomy and independence [28]. A holistic multidisciplinary rehabilitation approach [29] was used, which was ecological, customised, patient-centred, and protracted in time, as required by such a severe chronic pathology. Long follow-up and close collaboration between rehabilitation staff, family, school, and society were necessary. These objectives were achieved thanks to the determination of the parents, along with the staff, who were able to see beyond their son’s disabilities and to succeed in promoting a programme of psychocognitive growth and social-family integration.
This care report is offered, not simply as a description of a rare case of ARID1A syndrome, but as a possible model for the rehabilitative care of severe complex disabilities arising in the developmental period, where multiprofessional technical skills need to be combined with empathic capacity of acceptance of the patient and his family, as well as ability to construct innovative personalised settings to optimise the residual potential of the person.
Conflict of interest
The authors have no conflict of interest to report.