
Abstract
PURPOSE:
The need for pediatric post-acute facility care (PAC) is growing due to technological advances that extend the lives of many children, especially those with complex medical needs. The objectives were to describe [1] the types and settings of PAC; [2] the clinical characteristics of the pediatric patients requiring PAC; and [3] perceptions of PAC care delivery by clinical staff.
METHODS:
An online survey was administered between 6/2018 to 12/2018 to administrative leaders in PAC facilities that have licensed beds for children and who were active members of the Pediatric Complex Care Association. Survey topics included types of health services provided; pediatric patient characteristics; clinical personnel characteristics; and perceptions of pediatric PAC health care delivery.
RESULTS:
Leaders from 26 (54%) PAC facilities in 16 U.S. states completed the survey. Fifty-four percent identified as skilled nursing facility/long-term care, 19% intermediate care facilities, 15% respite and medical group homes, and 12% post-acute rehabilitation facilities. Sixty-nine percent of facilities had a significant increase in the medical complexity of patients over the past 10 years. Most reported capability to care for children with tracheostomy/invasive ventilation (100%), gastrostomy tubes (96%), intrathecal baclofen pump (89%), non-invasive positive pressure ventilation (85%), and other medical technology. Most facilities (72%) turned away patients for admission due to bed unavailability occasionally or always. Most facilities (62%) reported that insurance reimbursement to cover the cost of providing PAC to children was not acceptable, and most reported that it was difficult to hire clinical staff (77%) and retain staff (58%).
CONCLUSION:
PAC in the U.S. is provided to an increasingly medically-complex population of children. There is a critical need to investigate financially-viable solutions for PAC facilities to meet the patient demands for their services and to sufficiently reimburse and retain staff for the challenging and important care that they provide.
Introduction
The medical complexity of children continues to increase as a result of improved health treatments and technological advances. There is a parallel increased need for augmented health and family support. This need is especially pertinent for children with chronic medical complexity who [1] require continuous physiologic monitoring and care that may preclude their ability to live at home, and [2] require heightened support following acute-care hospitalization to stabilize health as they recover. In these circumstances, post-acute facility care (PAC) can be a valuable link as a transition to home or other less restrictive environments. However, in the authors’ clinical experience, there is often insufficient understanding among pediatric clinicians of PAC, including its role and how it fits into the pediatric health system.
PAC encompasses a wide range of health and social services (e.g., rehabilitation, skilled nursing, respite, end-of-life care, etc.) with large variation in scope and timing (e.g., short-term vs. residential placement in a facility). PAC facilities provide long-term care, family teaching, rehabilitation, and direct medical care to optimize patients’ health and function during recovery and to enable a safe and cost-effective transition from acute-care hospitalization to home [1]. During the last decade, PAC use in adult patients increased significantly as Medicare policies emerged to shorten expensive, acute-care hospital stays in a value-based system [2]. PAC is now routinely embedded within the health care system for adults, with sufficient PAC access and capacity in many communities for adult patients throughout the U.S. In contrast with adults, much less is known about PAC facility use, access, and capacity for children. However, similar to adults, the need for pediatric PAC is growing due to technological advances that extend the lives of many children who would not have survived their conditions in the past.
Recent studies suggest that hospitalized children are rarely referred to PAC [3–7]. Factors influencing infrequent PAC use include limited access to and capacity of PAC facilities in many areas of the U.S. [8]. Long delays in acute-care hospital discharge can occur due to limited availability of PAC beds as well as insurance restrictions for PAC coverage and approval [7]. Lack of knowledge about the health services offered by PACs may limit acute-care hospital providers’ awareness of which pediatric patients may benefit from PAC. Additionally, pediatric PAC and transitional care may be provided in a variety of health care settings, including a freestanding facility dedicated to children, a unit within an adult PAC facility, or even a unit or floor within an acute-care hospital.
To advance knowledge about pediatric PAC, the current study was conducted to assess the landscape of U.S. PAC health services for children. The objectives of the study were to describe [1] the types and settings of PAC provided; [2] the clinical characteristics of the pediatric patients cared for at PAC facilities; [3] the characteristics of PAC clinical staff; and [4] staff perceptions of PAC care.
Methods
Study design, setting, and participants
An on-line survey between 6/2018 to 12/2018 was given to administrative and clinical leaders in 48 facilities that provide PAC to children in the United States. Leaders –including chief medical officer, chief nursing officer, and medical director as well as licensed administrators - were identified from a list of facilities that are active members of the Pediatric Complex Care Association (PCCA), a national association of pediatric PAC facilities. These individuals were targeted for participation because of the breadth of administrative and clinical experience required to sufficiently grasp and answer the PAC survey. Leaders were eligible to complete the survey if they worked in PAC facilities that [1] admit children (ages 0 through 18 years) and [2] have licensed beds for children (i.e., in rooms designated for children or in rooms that can accommodate children or adults during their stay). Participants provided informed consent prior to study participation. Email reminders for participation were sent every two weeks for two months. Online surveys were sent via an individualized Survey Monkey© link. This research was approved by the Institutional Review Board at Franciscan Children’s Hospital.
Survey content
PAC survey items included the following: 1) health services provided by the facility (e.g., outpatient, inpatient, home health care, etc.); 2) clinical and demographic characteristics of pediatric patients served by the facility (e.g., age, types of chronic conditions, and medical device use); 3) characteristics of clinical personnel working at the facility (e.g., advanced practice nurses, respiratory therapists); and 4) participant perceptions of pediatric PAC health care delivery, including quality of care, integration with acute care, discharge barriers, and cost of care. Perceptions were ascertained with Likert scales. Additionally, perceptions of relative value with advances in PAC advocacy, research, and other domains were assessed using a 100-point allocation scenario. Participants distributed the points across the domains, assigning the most points to the highest valued domain.
Statistical analysis
PAC facility survey items were scored and summarized using frequency statistics [e.g., percentages for categorical answers and mean (standard deviation) for ordinal answers]. Aggregate counts were calculated across facilities where appropriate (e.g., total number of PAC facility beds for children across all facilities).
Results
Characteristics of pediatric post-acute care facilities
Twenty-six (54%) PAC facilities, located in sixteen states from the U.S., completed the survey; eleven in the Northeast, eight in the Midwest, five in the South, and two in the West. Types of respondents included medical director [n = 7 (27%)], chief medical officer [n = 4 (15%)], chief nursing officer [n = 4 (15%)], and president/chief operating officer [n = 3 (12%)]. Fifty-four percent (n = 14) were identified by respondents as skilled nursing facility/long-term care, 19% (n = 5) intermediate care facilities, 15% (n = 14) respite and medical group homes, 12% (n = 3) post-acute rehabilitation, and 8% (n = 2) palliative care or hospice centers (Table 1). All facilities cared for children between the ages of 5-to-18 years; 59% (n = 15) cared for adults aged 19 and older. Fourteen (54%) had a patient catchment size of 11-to-100 miles, while the remainder (46%) had a catchment area of ≥100 miles. Eighty-five percent (n = 22) have been in operation with pediatric care for >25 years. Most (92%) were not-for–profit organizations. Median number [interquartile range (IQR)] of inpatient beds across facilities was 55 (IQR 38–52) (Table 2).
Characteristics of twenty-six U.S. pediatric post-acute care facilities
Characteristics of twenty-six U.S. pediatric post-acute care facilities
Beds and staffing of twenty-six U.S. pediatric post-acute care facilities
All facilities provided inpatient care. Across facilities, the most common other health services included occupational, physical, or speech therapy [77% (n = 20)], school/education [3% (n = 19)], and respite [69% (n = 18)]. Half (50%) of facilities offered outpatient care, including specialty care [46% (n = 12)], primary care [23% (n = 6)], dental care [15% (n = 4)], and home care [>15% (n = 4)]. Regarding specific clinical service lines, all facilities provided tracheostomy and long-term ventilation care. The majority also provided palliative care [77% (n = 20)], medical rehabilitation [73% (n = 19)], post-trauma [62% (n = 16)], and neonatal care [58% (n = 15)].
Demographic and clinical characteristics of children receiving post-acute care
All facilities cared for children aged 5-to-18 years; 73% (n = 19) provided care for neonates and infants age <1 year; 66% (n = 17) for young adults (19-to-25 years), and 23% (n = 6) for adults aged 26-to-50 years (Table 3). Sixty-nine percent of facilities (n = 18) reported that the clinical characteristics of their patients have significantly increased in medical complexity over the past 10 years. All facilities cared for patients with neuromuscular/neurodevelopmental and respiratory care health problems. A majority of facilities provided care for patients with musculoskeletal [92% (n = 24), digestive 92% (n = 24)], trauma [77% (n = 20)], and cardiac [73% (n = 19)] health problems (Table 3).
Characteristics of patients cared for by twenty-six U.S. pediatric post-acute care facilities
Characteristics of patients cared for by twenty-six U.S. pediatric post-acute care facilities
All facilities accepted care for children with tracheostomy and for those requiring mechanical ventilation, with an average ratio of one respiratory therapist per 19 pediatric patients. A majority of facilities reported capability to care for children with gastrostomy tubes [96% (n = 25)], intrathecal baclofen pump [89% (n = 23)], non-invasive positive pressure ventilation [85% (n = 22)], and other medical technology. Presence of mental health issues [65% (n = 17)] and use of diaphragmatic pacers [23% (n = 6)] were the most commonly cited reasons for denial of admission to a PAC (Table 3).
PAC admission
The majority [73% (n = 19)] of respondents reported experience turning away patients for admission due to bed unavailability at least occasionally (i.e., occasionally, frequently, or always); 27% (n = 7) reported this occurrence frequently or always. The majority [69% (n = 18)] found the variation in the process for insurance approval to PAC across different insurers (e.g., public vs. private) to be unacceptable. Thirty-five percent (n = 9) reported that the efficiency of the process to transfer children from referring institutions, including acute-care hospitals, is inadequate. Thirty-one percent (n = 8) of respondents felt that the health information, including clinical details, about the patient conveyed by acute-care hospital providers during transfer was insufficient.
PAC discharge
Most [69% (n = 18)] facilities experienced issues at least occasionally with the approval, ordering, and/or delivery of durable medical equipment to the children’s homes upon discharge; 23% (n = 6) reported this occurrence frequently. Nearly all 96% (n = 25)] experienced issues at least occasionally with family housing at discharge; 35% (n = 9) reported this occurrence frequently or always. All (100%) facilities experienced challenges at least occasionally with other social or family issues (e.g., financial or employment) at discharge; 62% (n = 16) reported this occurrence frequently or always (Fig. 1).
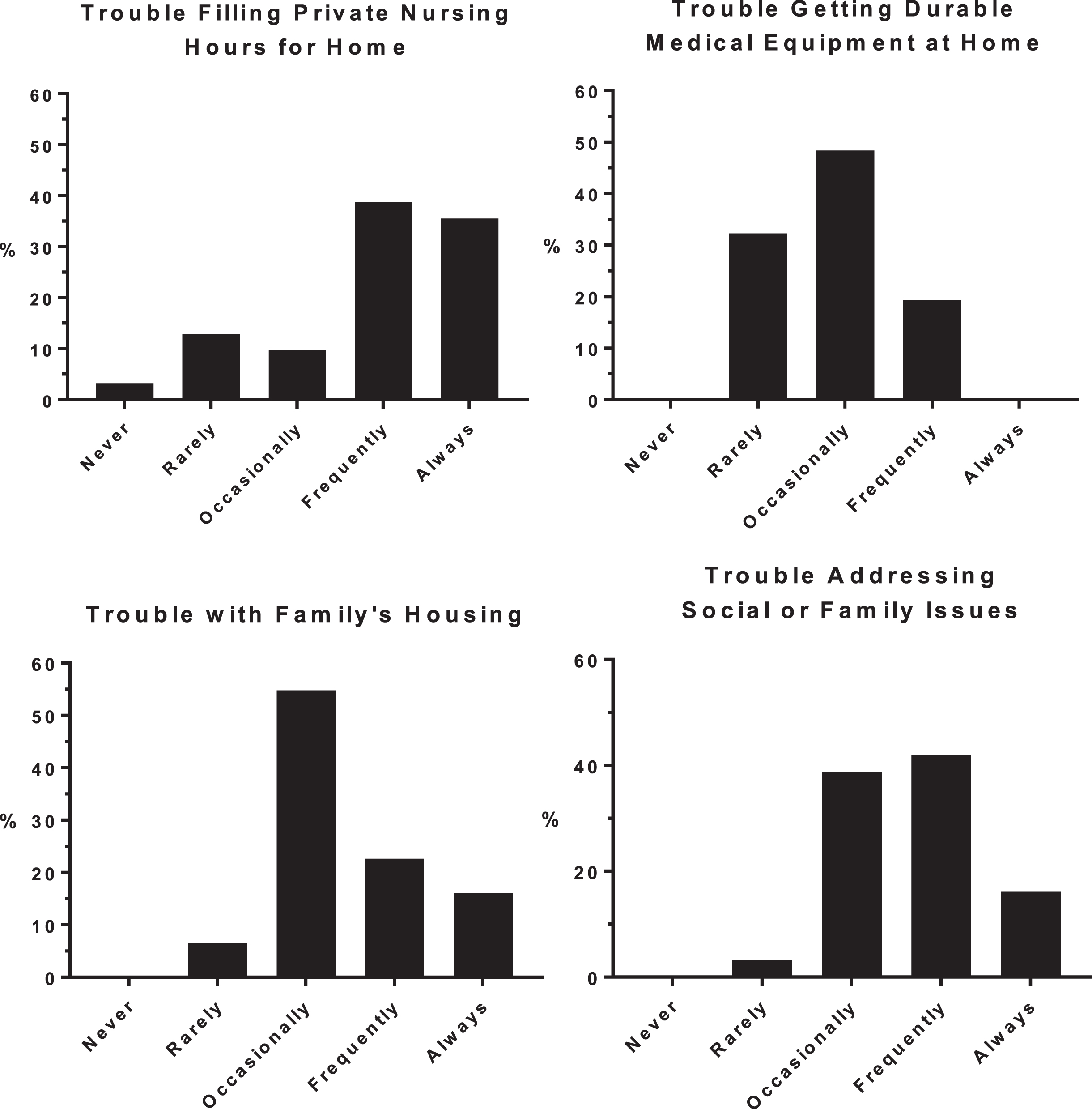
Participants were asked how frequently their facility experienced each type of issue.
The most common payer (75–100% of pediatric patients across facilities) was Medicaid. The majority [62% (n = 16)] of facilities reported that insurance reimbursement to cover the cost of providing PAC to children was not acceptable; 69% (n = 18) of facilities reported that the variation in reimbursement across insurance providers was also not acceptable. Most facilities reported that it was difficult to hire clinical staff [77% (n = 20)] and to retain hired staff [58% (n = 15)].
Measuring quality of care
All facilities measured patient and family satisfaction with care. Most facilities measured falls/fractures [92% (n = 24)], facility-acquired nosocomial infections [88% (n = 23)], medication adverse events [88% (n = 23)], pressure ulcers [88% (n = 23)], and functional outcomes of the patient [77% (n = 20)]. There was a greater frequency of indicators that facilities used than were required by regulations. Only 31% (n = 8) of facilities were required to use patient and family satisfaction of care. The largest required indicator to report was falls/fractures at 62% (n = 16).
Post-Acute Care Priorities. PAC facilities prioritized financial stability [mean 24.4 (SD 11.6) points] and ability to hire and retain clinical staff [mean 23.1 (SD 11.6) points] as the two most important activities to optimize their ability to provide PAC. Fewer points were allocated to the ability to train and educate staff [16.3 (SD 8.1) points>], community advocacy [15.0 (SD 9.5) points], and relationships with referring institutions [12.3 (SD 8.6) points]. The fewest points [9 (SD 7) points] were allocated to research on PAC care delivery and treatment for children (Fig. 2).
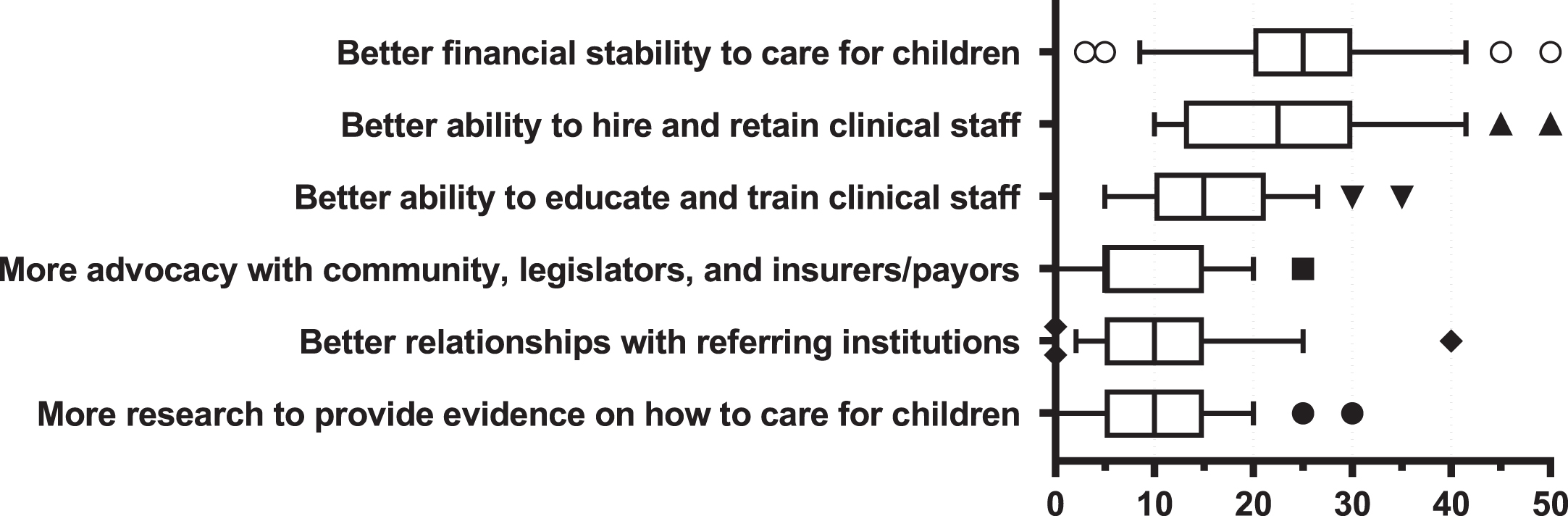
Perceptions of relative value with advances in post-acute care advocacy, research, and other domains were assessed using a 100-point allocation scenario. Participants were given 100 points total and asked to allocate points to each of the six domains shown on the y-axis. Participants distributed the points across the domains, assigning the most points to the highest valued domain. Box and whisker plots represent median (mid-box line), 25th and 75th percentiles (left and right box edges), 10 and 90th percentiles (whiskers), and 91st to 99th percentiles (outlier symbols).
All PAC facilities acknowledged treating children with neurodevelopmental disorders as well as those with chronic respiratory health issues, including the need for tracheostomy. Children with these attributes are known to have prolonged lengths of stay in acute-care children’s hospitals [9]. Efforts to target those for proactive consideration for PAC might be beneficial. Such consideration early in an expected prolonged admission might help improve acute-care to PAC transfer efficiency, communication, and overall quality. In addition, while the respondents all identify as pediatric facilities, a large percentage noted that they care for young adults. This is likely reflective of improved survival of children with complex medical problems and may be indicative of an emerging population of young adult patients that will require specialized post-acute and residential care in the near future. Whether those adult survivors of pediatric conditions are best served in a pediatric-centric facility or an adult facility for young adults has not been well studied.
While all facilities cared for children with tracheostomies and long-term ventilation care, there was a wide range of other care and health services provided across the continuum, suggesting no clear consensus about what core services are needed for PAC care beyond gastrostomy, tracheostomy, and ventilator care. Only 11% provided psychiatric care, which was the most significant factor to deny a child’s admission to the facility. This is consistent with the widely recognized mental health care crisis experienced in both pediatric and adult medicine. Depending on the medical needs of the child, they may not be able to receive care at these facilities, or may need to go far distances. This is further shown through the size of the catchment areas; nearly half of the facilities had a catchment size greater than 100 miles. This is a significant burden on multiple levels for families who want to remain involved in their child’s life and care, but whose nearest PAC facility is at a significant distance from their home.
The health care and social/familial challenges reported at discharge in the current study deserve more investigation. The high rates of problems with home, private-duty nursing, and medical equipment as well as family housing and other social issues are troublesome but not unfamiliar in the society. The effectiveness of PAC ultimately depends upon the quality of home, community, and social services available to maintain the health and well-being of children with medical complexity after PAC discharge. Exploration of improved integration of PAC with those services may be necessary to provide the best health care system for them. The experience of a child with medical complexity being readmitted within days or weeks following a carefully planned discharge speaks to the tenuous reality of care at home for many of these children.
More attention and action are needed to address the financial priorities raised by the survey respondents. In addition, more information on how facilities balance cost and reimbursement would be helpful [10–12]. Most respondents found payor reimbursement unacceptable for PAC health services. Insufficient reimbursement may be one of the factors that has contributed to the mismatch in the supply of pediatric PAC facilities vs. the demand for them [8]. This situation could become self-defeating for the health care system as a whole, because some readmissions to acute care may be reimbursed adequately at a higher per diem, whereas PAC availability at a significantly lower per diem may not be available. Use of PAC after acute-care hospitalization has been associated with decreased hospital readmission for children [9]. Opportunities for PAC revenue may exist with involvement in pediatric accountable care organizations that link PAC with acute hospital care for cost savings including readmission reduction (i.e., value-based care) [13–16]. Newly passed federal legislation on care management for children with medical complexity may also benefit PAC financial stability, especially if PAC is included in the implementation of the legislation’s health home concept [17]. As hiring and retaining clinical staff was a major problem identified by survey respondents, a better understanding of incentives and other financial factors to engage and retain high quality PAC staff is necessary.
This study has several limitations. Perceptions were elicited across a broad array of health service topics from one respondent at each facility. It is possible that there are variations in perceptions across staff within a facility. A broader assessment of all stakeholders, including families, payers, and referring providers, would offer a richer understanding of pediatric PAC. In addition, the geographic distribution of the responding organizations may not represent a true cross-section of the country. Due to the lack of information on the total number and types of PAC facilities in the U.S., the generalizability of the findings is not known. Further investigation of non-respondents may be helpful. Also, the sample size of the facilities did not have sufficient statistical power to meaningfully assess relationships between facility attributes and perceptions of care. The survey was not designed to elicit the reasons for the participants’ answers. For example, further study –perhaps qualitative –may be necessary to understand more about the reasons why respondents reported problems with insurance approval for PAC admission. Understanding those reasons will inform the development of solutions to address such problems, which is critical to getting children out of acute care hospitals and into the proper level of care based upon their medical status.
Despite those limitations, the findings from the current study will [1] raise awareness of the types of patients, health services, and challenges to care delivery experienced across PAC facilities in the U.S.; and [2] spark new areas of research investigation and action to advance knowledge on how to optimize PAC for children with chronic medical conditions. While this population is small in number, the amount of health care resources they consume is disproportionately large. Further work in this area is vitally important to be good stewards of the available resources and to support future program and resource development. Improved understanding of PAC will help to advance its integration into care across the continuum for children with medical complexity.
Footnotes
Acknowledgments
We acknowledge Christopher Haines, Michael Dribbon, and Sibyl Wilmont for their input and work on the design of this work, interpretation of findings, and drafting of the manuscript. We wish that there were more available slots to include them in the author list.
Conflict of interest
The authors have no conflict of interest or financial relationships to disclose.
Funding
None.