
Abstract
PURPOSE:
This study aimed to explore the family experience and associated challenges of transporting children with medical complexity (CMC) in personal vehicles.
METHODS:
Parents/guardians of CMC in Maryland were recruited to participate in an audiotaped, semi-structured interview. Conventional content analysis was applied to transcripts.
RESULTS:
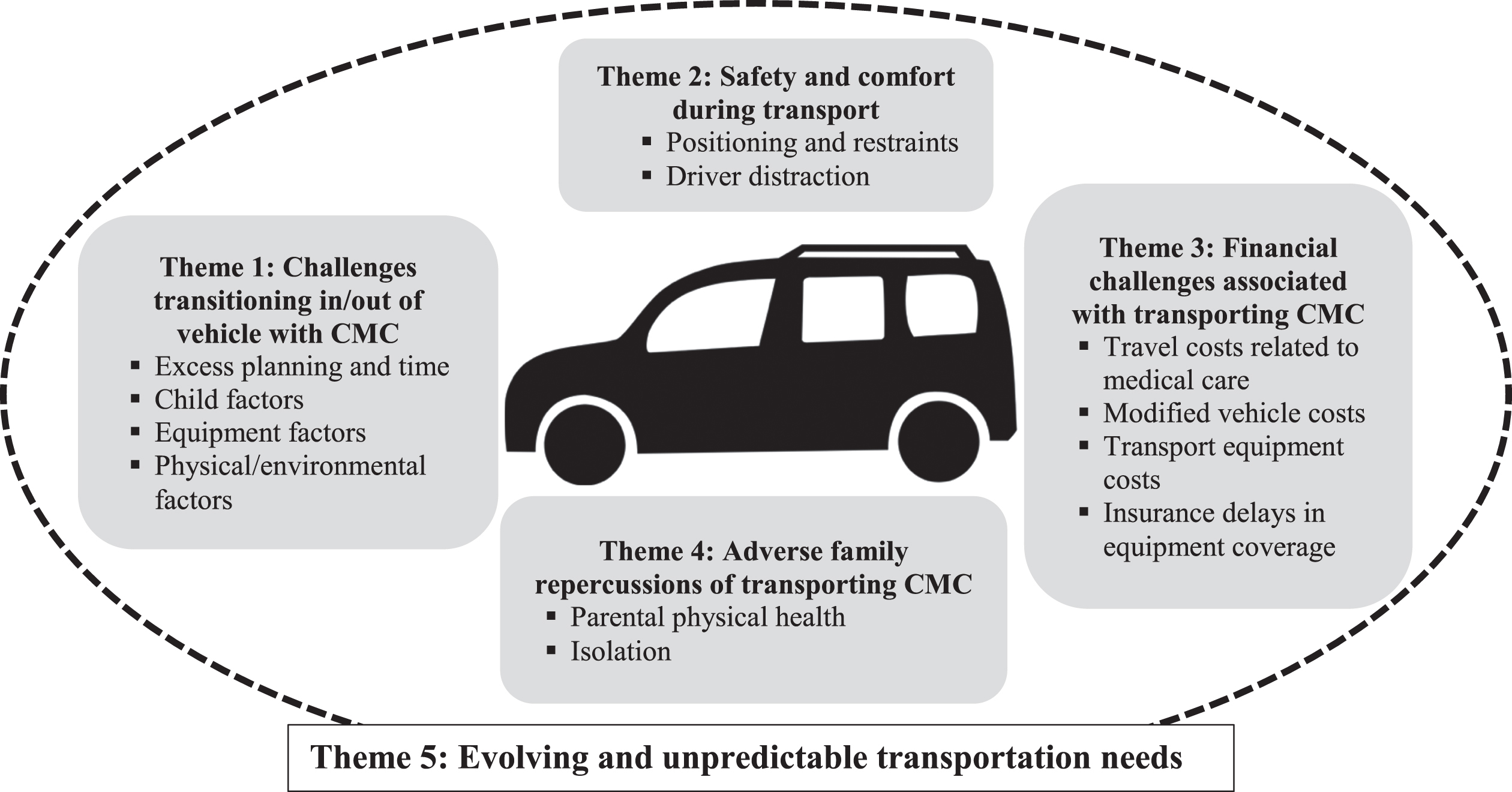
Data from 29 participants who indicated use of personal vehicles to transport their CMC were included in the analysis. Transportation challenges were common, and analysis revealed the following themes: 1) challenges transitioning in/out of the vehicle: excess planning time, child factors (e.g., weight), equipment factors (e.g., wheelchair), physical and environmental factors, 2) safety and comfort: CMC positioning/restraints, driver distraction, 3) financial challenges: travel costs related to medical care, accessible modification costs, transportation equipment costs, insurance delays in equipment coverage, 4) adverse family repercussions: parental physical health, isolation, and 5) evolving and unpredictable transportation needs.
CONCLUSION:
Families with CMC experience multifactorial challenges that impact all phases of travel in personal vehicles and negatively impact child and family safety, access to community and medical care, family finances, and overall well-being. Health care providers can support families by identifying transportation challenges that contribute to health inequities, tailoring solutions to the family’s unique needs, and advocating at a policy level to promote change.
Introduction
Driving around in the family vehicle is an integral part of daily living for families with children who must shuttle to and from school, sports, play dates, and medical care. The National Household Travel Survey reports 87% of “daily trips” are in personal vehicles, with each person averaging 4 trips per day, totaling 1.1 billion trips per day nationally [1]. As a result, the automobile industry is large and includes a specialized sector dedicated to family transport, giving parents widespread options for child safety and comfort in their vehicle. Unfortunately, transport needs are not uniformly met for all families, including those with children with medical complexity (CMC).
Like most families, parents of CMC are the primary providers of transportation for their children [2]. CMC, defined as children with severe, chronic health conditions, high medical care needs, and functional limitations, [3] often rely on medical devices and ambulatory equipment including bulky postural supports; all must be transported with the child to ensure safe and comfortable travel. Literature regarding the family experience of transporting CMC is limited and largely based on European data. UK families with children with cerebral palsy have described how good transportation, including access to personal transport and appropriate parking, is crucial for family community participation, child school attendance, and access to medical care [4]. Swedish families of children with physical disabilities have expressed concerns with attending to their children, inadequate positioning, incorrect restraint use, and confusion over how best to transport their children [2, 5] Both Swedish and American families with children with behavioral issues or a diagnosis of autism spectrum disorder have expressed concerns about children refusing to use or escaping from car restraints while in transport [6, 7].
As personal transportation is a major component of daily living and healthcare access for US families with CMC, this study aimed to explore the family experience and associated challenges of transporting CMC in personal vehicles. Specifically, challenges to transportation that might impact child and family safety, community and health care access, and family well-being were investigated. This information is meant to increase awareness of and advocacy regarding transportation challenges for families with CMC.
Methods
This qualitative study was part of a larger mixed-methods study on housing, household expenses, and transportation for families of CMC. Recruitment occurred in partnership with a state-based parent advocacy organization and a case management agency. Information about the study with a link to complete an initial survey was sent to respective listservs. Eligible participants lived in Maryland, were English-speaking, and were parents or guardians of children, youth and young adults <26 years old who met criteria for children with special health care needs using a validated screener [8]. Survey participants were recruited for an in-depth interview about their experience with housing, finances, and transportation. Surveys were completed by 137 participants, and 85 agreed to be contacted for an interview; 75/85 had a child(ren) with more complex medical needs (i.e., requiring adaptive equipment or medical technology, eligible for home nursing) and were prioritized for recruitment. Telephone interviews were conducted from August through November 2020; recruitment stopped when thematic saturation was reached (n = 31). Interviews were audiotaped and transcribed.
Interview questions were developed a priori, based on literature review [2, 4–7] and consultation with families and professionals knowledgeable about CMC. For purposes of this analysis focused on transportation, interview data from families in the larger study who indicated use of a personal vehicle for transportation (n = 29 out of 31) were included. Authors reviewed full transcripts to develop a limited data set of transportation-related content that parents provided in response to transportation-specific questions (Table 1) or at any point in the interview.
Transportation questions from interview guide
Transportation questions from interview guide
These transportation questions are a subset of questions from a more extensive mixed-methods study on housing, household expenses, and transportation for families of CMC. Full interview available upon request.
Conventional content analysis was applied to the limited data set [9]. Two authors individually reviewed the master document and independently developed a preliminary codebook. The codebook was refined through an iterative process with any discrepancies resolved through discussion with the study team. Final codes were applied to transcript data, and a subset of data was double coded for cross checking. Codes were grouped into code families and themes through discussion with study team.
The Johns Hopkins Institutional Review Board approved the study and informed consent was obtained.
All 31 participants interviewed in the larger study indicated transportation challenges; 29 reported use of personal vehicles and were included in this analysis. Participants were predominantly female (90%, n = 26), had 1–4 CMC in their family, and resided in geographically diverse locations within Maryland (suburban 62%, rural 23%, urban 15%). Within study families, there were a total of 37 CMC with variable medical conditions requiring complex care and frequent medical visits (Table 2). Nearly all of the children (92%) were dependent on adaptive equipment or medical technology, and over half required medical appointments at least monthly (Table 2). Almost all of the children (95%) had developmental delay/disability, and 16% had a mental health diagnosis (i.e., anxiety, depression, bipolar disorder, oppositional defiant disorder).
Characteristics of children with medical complexity
Characteristics of children with medical complexity
a. Percentages sum to greater than 100% as multiple responses per child were permitted. b. Adaptive equipment includes lifts, standers, shower chairs, and ramps. c. Respiratory support includes tracheostomy, ventilator, continuous positive airway pressure machine, bilevel positive airway pressure machine, and oxygen. d. Additional pulmonary equipment includes nebulizers, vibratory vests, and cough assists.
Qualitative analysis revealed five transportation themes and associated subthemes (Fig. 1). The first theme was the challenge of transitioning in/out of the vehicle, including excessive planning and time, the child’s physical and behavioral needs, challenges loading and unloading mobility and medical equipment, and physical and environmental factors that affect entry and exit from the family vehicle. The second theme was safety and comfort during transport, including positioning and restraints of CMC and driver distractibility. The third theme was financial challenges, including travel costs related to medical care, accessible modifications costs, transportation equipment costs, and insurance delays in equipment coverage. The fourth theme was adverse family repercussions from transporting CMC, which includes parental physical health and family isolation. The fifth theme was evolving and unpredictable transportation needs. Illustrative quotations were edited for anonymity and clarity.
CMC family transportation themes and subthemes.
Excess planning and time
Anticipating behavior and medical needs as well as planning and preparing for transport with medical equipment and supplies occurred even before the caregiver placed their child in the vehicle. Families with CMC often took longer to prepare, even for quick trips in the car, which resulted in decreased flexibility and spontaneity in daily activities.
“You just have to plan in advance because everything’s slower. It’s not like we can say, in five minutes, we’re going to leave.”
Parent A (child with autism, pain syndrome, gastrointestinal dysfunction)
Child factors
Once families were prepared for transport, challenges continued with getting into the car. These difficulties reflected the child’s specific underlying physical and behavioral needs. Participants described difficulties lifting and positioning a non-ambulatory child in the car due to their size, weight, and physiological condition.
“Well, it’s difficult because I have to carry him and put him in. He’s pretty long and I have a sedan. We have bought a decent size vehicle. It’s not like I’ve got a mini car. But he’s 46 inches long and he’s got hypertonia in his legs . . . When you’re trying to get him in the vehicle, he’s this rigid board and you can’t manually bend him . . . It’s difficult.”
Parent B (child with cerebral palsy, feeding tube, respiratory support)
Aggressive behavior and safety concerns when transitioning in/out of car were described by some families, as transportation sometimes triggered self-injurious and/or harmful behaviors.
“We have a transition protocol for him . . . he does get aggressive if he doesn’t want to go somewhere. Being on the third floor [of an apartment] it makes it more complicated. . . If he doesn’t want to go, we have a battle on our hands.”
Parent C (child with autism, epilepsy, intellectual disability)
Equipment factors
Participants reported that transporting medical and mobility equipment was demanding, as was coordinating equipment transfer while managing their child’s needs. The size and weight of equipment added to travel complexity; it was difficult to lift, time-consuming to load, and reduced space inside the vehicle.
“Fitting two wheelchairs in my van was a lot of work. And the lifting, you lift [my son], and then you put him there, then you go pick up [my daughter], you lift her in and out. Then, you have to take the wheelchairs. My daughter’s wheelchair is electric. It’s very heavy. It weighs like 70 pounds.”
Parent D (children with neuromuscular disorders, developmental delay, wheelchair)
Physical and environmental factors
Once at the destination, additional difficulty existed in getting the child out of the car due to parking or physical barriers, especially for those who needed wheelchair accessible transportation, ramps, or lifts. Parking lots and sidewalks modified for accessibility did not always meet the child’s needs, resulting in added transfer time, inability to exit the car, and frustration.
“They had handicap spots, but they weren’t wide enough . . . There ended up being only two spots in the parking lot where we could actually get her out of our van, because we had a side-loading van.”
Parent E (child with neuromuscular disorder, ventilator, feeding tube, wheelchair)
Theme 2: Safety and comfort during transport
CMC positioning/restraints
Participants were often confused about proper positioning while in transit. They noted an association between their child’s discomfort and inadequate/absent postural supports or adaptive transit equipment (e.g., adaptive car seat, accessible vans).
“Ever since [name] became paralyzed, he used to love going on rides. He doesn’t like it now because he can’t feel his feet. He doesn’t feel grounded. He does not like long drives at all. It makes him feel super uncomfortable.”
Parent F (child with ventriculoperitoneal shunt, paraplegia, wheelchair)
Participants were also confused about how to safely restrain their child during transport given their child’s specific needs. This confusion surrounded baseline transport needs and short-term modifications (e.g., following procedures).
“Until now, he’s been in a car seat, but he just had surgery, so we can’t really transport him without laying him down in the back of a car.”
Parent G (child with cerebral palsy, seizures, wheelchair)
Driver distraction
Participants discussed the need to balance driving with simultaneously managing their child’s behavioral and medical needs.
“ . . . [it] is always tough in the car. He wants to open the windows, tries to open the doors, tries to remove the seat belt, tries to hit others in the car with feet, pushing the front seat, hitting the front seat.”
Parent H (child with autism, intellectual disability)
“ . . . there are literally times when I’m driving down the highway with 911 dialed, in case I need to call.”
Parent I (child with genetic syndrome, feeding tube, respiratory support, wheelchair)
Theme 3: Financial challenges associated with transporting CMC
Travel costs related to medical care
Accessing the medical system frequently could result in significant out-of-pocket transportation expenses for families; associative costs (e.g., gas, parking) were not covered by insurance.
“We have the extra doctor’s appointments that we have to go to. That’s extra gas and travel expenses. . . We could not save any money at all. We had a lot of travel expenses that we were dealing with.”
Parent J (children with cranio-facial disorder, intellectual disability)
Accessible modification costs
Transporting CMC, especially non-ambulatory children, could require purchasing a larger vehicle, an accessible/customized vehicle, or modifying an existing vehicle. Such expenses were typically not covered by insurance, with significant out-of-pocket burden. Difficulties finding accessible automobiles and extended wait times for customizations were also reported.
“There weren’t many places in the area that did the handicapped modifications that we needed. . . We were able to find a company that could do the modifications, but it was [far away]. That process took some time and a lot of money.”
Parent K (children with autism, leukodystrophy, feeding tube, wheelchair)
Transport equipment costs
Insurance infrequently covered adaptive equipment for transport of CMC; participants described paying out-of-pocket, using a waiver program, if available, or foregoing equipment altogether.
“I need to look into getting an adaptive car seat for her as she’s almost growing out of her current one. Most of these things are unfortunately not covered by insurance. . . They’re very expensive. We tried submitting [at] one point the [adaptive] stroller for insurance. We had so many issues and never got anywhere with it. We didn’t even move forward with it.”
Parent L (child with epilepsy, autism, intellectual disability)
Insurance delays in equipment coverage
On the rare occasion insurance or waiver programs covered an item, it often took a long time to receive it. Participants expressed frustration with inefficiencies and delays in approving items needed for travel.
“[The waiver caseworker] didn’t submit anything. She was like, ‘Oh, that’s why you sent me quotes.’ Then, she was like, ‘Well, you don’t need the Hoyer lift if we’re trying to get a van.’ I’m like, ‘It’s taking you months to try to get this van. I need the Hoyer lift. I can’t go anywhere or do anything.”’
Parent M (child with neuromuscular disorder, respiratory support, wheelchair)
Theme 4: Adverse family repercussions of transporting CMC
Parental physical health
Challenges transporting CMC could have a physical toll on caregivers.
“I have back issues from all of the lifting of equipment in and out, and dismantling that wheelchair, which is not light at all. Every time we go somewhere I have to dismantle the wheelchair and lift that up in the car as well as lift him up in and out the car.”
Parent N (child with cerebral palsy, feeding tube, respiratory support, wheelchair)
Isolation
Challenges with transportation impacted the families’ ability to access health care, basic needs, and the community.
“Oh travel! Travel is a big issue. We stopped traveling just because of him. . . Certainly we wish that he could sit more than half an hour in the car seat without removing the seat belt so that we could travel long distances.”
Parent H (child with autism, intellectual disability)
“His wheelchair is like 700 pounds. There are things that we can’t do or [places] we can’t go because of that.”
Parent F (child with ventriculoperitoneal shunt, paraplegia, wheelchair)
Theme 5: Evolving and unpredictable transportation needs
The families experienced evolving, unpredictable transportation needs as the child grew: medical equipment/supports enlarged in bulk, medical problems evolved, and new equipment was added. This made it difficult for families to prepare for future transportation needs.
“We’re going to have to think about getting a van or something wheelchair accessible, especially if he’s going to get a power chair. I almost kick myself now. We thought about it at the time, buying a sedan versus buying a larger vehicle. We were like, ‘No, he’s been doing so great. Like if he’s walking now, what are the chances?’ Then something happens. I guess it’s difficult because there’s no way to predict and it’s like you don’t want to assume they need more than they do. . . ”
Parent B (child with cerebral palsy, feeding tube, respiratory support)
Discussion
Families with CMC experience a diversity of challenges, including access to care, [10–12] financial hardship, [12–15] physical and psychosocial stressors, [13, 17] and marital strain and family pressure [18, 19]. In addition to requiring daily medications and therapies, [20, 21] CMC often have frequent medical appointments, [3, 20] regular laboratory testing and procedures, [3, 10] rehabilitation visits, [3, 10] and repeated hospitalizations [3, 22] The time and effort required for coordination and management of this care can have considerable impact on families’ lives, [14, 23], including loss of parental wages [3, 15] and limitations on community engagement and socialization [13, 19]. Many of these challenges have transportation at their core, as it is vital to accessing health services and the broader community.
This paper explored challenges associated with personal vehicle transport of CMC from the perspective of US families. These challenges were multifactorial and occurred within all phases of travel from planning to destination. They affected travel to medical care, running basic errands, and interacting with the community. Some difficulties the families faced were the direct result of the child’s physical and behavioral characteristics: the child’s weight, size, immobility, physiological condition, and behavior. Other challenges were associative, such as the size and volume of medical equipment and supplies needed for safe transport, parking and environmental barriers, adequacy of families’ vehicles, and substantial out-of-pocket transportation costs. The data indicated that transporting CMC affected the broader social, financial, and physical well-being of the entire family.
Talk about transportation
These families with CMC experienced multiple challenges meeting child and family needs, including basic transportation. US families with CMC expressed a need for support transporting their children. The study participants described difficulty transferring CMC in/out of the car due to excess planning time, child factors, equipment factors, and physical/environmental factors. They also noted concerns for safety and comfort while driving. This is consistent with research of Swedish families who reported anxiety over a child’s positioning and difficulty paying attention while transporting their children with disabilities [5]. Since CMC have a high frequency of medical and rehabilitation appointments due to complex care needs, [3] there are many opportunities where providers can help caregivers think through and plan for such transportation challenges.
Guidelines exist to help medical and rehabilitation providers discuss transportation with families. The American Academy of Pediatrics (AAP) recommends that pediatricians have a basic understanding of child passenger safety and communicate and review child safety recommendations with families at each visit [24]. Both the AAP and National Highway Traffic Safety Administration have published guidelines for safe transport of CMC [25–28] as well as car seat recommendations based on common medical conditions found within this population (e.g., muscle tone, gastrointestinal issues, behavior) [25, 28–31]. However, a recent study that explored the prevalence of physician screening for social determinants of health found that only 35% of clinics and hospitals surveyed reported asking their patients about transportation needs [32]. It is unknown how many ask families with CMC about their transportation challenges.
Providers should ask families with CMC targeted transportation-related questions to identify and address the unique challenges they face (Table 3). Exploring these challenges may uncover contributing physiological and/or psychological issues and identify whether further referrals are warranted (e.g., orthopedics, psychologist, additional rehabilitation specialists). Also, broadening the focus to include the family unit could potentially identify safety concerns and challenges noted by study participants that are more associative to the child (e.g., adequacy of family vehicle, parental injuries, financial burden, and parental feelings of isolation). Considerations of potential modifications, referrals, treatments, and recommendation for caregiver supports may be possible through thoughtful questioning, especially at key times when needs may be evolving: growth spurts, puberty, new diagnoses, worsening of existing conditions, new equipment, and changes within family structure (i.e., new sibling).
Transportation questions for families with CMC
Transportation questions for families with CMC
Participants expressed uncertainty about various aspects of their transportation needs, including what postural supports were appropriate, when to transition to accessible equipment, how to properly use equipment in the vehicle, and when and where to purchase an accessible vehicle. This was further complicated by the unpredictable transportation needs that emerged as the child grew, medical needs changed, and family needs changed. In order to identify and address these issues, families and physicians relied on referrals to rehabilitation specialists (e.g., occupational therapist [OT], physical therapist [PT], child passenger safety technician) and equipment vendors with expertise in this field.
However, not all rehabilitation specialists have adequate training to evaluate the needs of CMC. A survey of over 1,000 rehabilitation therapists including OTs and PTs within the US found that the majority had little or no knowledge (53%), formal training (79%), or experience (54%) regarding the safe transport of children with special healthcare needs [33]. As such, when referring CMC for transportation assessments, physicians need to confirm that the rehabilitation provider has experience evaluating and addressing the needs of this population.
Additionally, providers must be careful that rehabilitation therapists or vendors do not make independent decisions about medical equipment that are not in accordance with federal or state regulatory requirements for physician-initiated prescriptions for durable medical equipment [34]. A survey of pediatricians from Mississippi and Ohio found that one-third of respondents from Mississippi and one-quarter of respondents from Ohio would allow rehabilitation therapists to be the sole decision maker of wheelchair orders and that nearly 10% would allow a vendor to make the final decision alone [34]. As families noted challenges with reimbursement of transportation-related equipment, physicians must balance relying on rehabilitation therapists and vendors to provide guidance on transportation equipment while also taking the lead to prescribe appropriate equipment/supports that will be reimbursable and appropriate for the child and family.
There is a need to develop universal guidelines that detail an organized, multi-disciplinary approach to evaluating a child’s specific transportation equipment needs and placing the relevant equipment orders. Such guidelines should also specify intervals for reassessment over time to accommodate for growth and evolving needs.
Financial resources
The financial burden associated with transporting CMC is significant, in part due to insurance denials or delays in coverage for transportation equipment/supports. Even with multiple coverage resources (i.e., private and public insurance, waivers), many of the participants were still paying out of pocket for items, including adaptive car seats. This was surprising because Medicaid covers the costs of adaptive car seats in all 50 states, although determination of eligibility varies by state [35]. More research is needed to understand why durable medical equipment for personal transport is so poorly covered by insurance.
A multi-disciplinary approach to securing transportation supports (e.g., car seats, wheelchair locks, lifts, accessible vehicles) may be necessary to reduce transportation costs. Health care providers can support families financially by working with insurance companies, rehabilitation specialists, and vendors to understand what referrals and prescription patterns are necessary for maximum reimbursement (e.g., letter of medical necessity, scripts, referral for evaluation by a PT instead of an OT). Additional help through case management and social workers may help identify potential secondary financial resources (e.g., eligible loan programs). Financial planners and low-cost financial advising services, through legal aid or pro bono projects, can help parents navigate insurance and additional financial concerns. Advocating for increased access to grants to offset the cost of transportation equipment may also be beneficial. Research on vehicle and accessibility grants in Sweden noted that families of children with disabilities who received either vehicle or vehicle adaptation grants reported increased frequency of travel, increased spontaneous travel, a positive effect on freedom, and a positive effect on the child’s daily life [36].
Consider modifications to traditional appointment scheduling
Health care providers should consider the unique transportation challenges of CMC families when scheduling medical appointments. Participants noted significant time related to travel preparation, challenges transitioning in/out the car, and parking/environmental barriers regardless of destination, geographic location, and/or vehicle accessibility. Additionally, they described how parking, gas, and toll fees accrued with every appointment.
Limiting the number of trips needed for in-person medical appointments could help reduce some of these transportation burdens. One approach is grouping co-located specialist and therapy appointments in the same day. Case managers and/or social workers may be necessary to facilitate this level of coordination. Another approach is increasing the use of telemedicine appointments to offset transportation challenges. The expansion of telemedicine in response to the COVID-19 pandemic has shown that this is a feasible option for CMC families. Telemedicine visits result in reduction of healthcare and travel costs for families with CMC, reduction in unplanned hospitalizations, and improved family satisfaction with healthcare [37]. A third approach is partnering with area school systems to provide clinical and rehabilitation services onsite at the child’s school, which could further reduce the transportation burden of CMC families.
Advocacy and political action
Health care providers should partner with professional organizations (e.g., AAP, American Academy of Physical Medicine and Rehabilitation, American Physical Therapy Association), parent advocacy groups (e.g., Parents Helping Parents, Family Voices), and nonprofit organizations (e.g., United Cerebral Palsy, The Arc) to advocate for improvements in personal transportation for families with CMC. In order to address the specific challenges expressed by the participants, some particular areas of advocacy are improved Medicaid reimbursement and financial grants (state and federal) for accessible vehicles and adaptive equipment commonly used for personal transportation (e.g., lifts, postural supports), improved accessible parking design, family transportation waivers to offset driving costs (e.g., gas, parking), improved evaluation standards for the identification of family transportation needs (e.g., development of family-centric transportation clinics), and continued or enhanced reimbursement for telemedicine services. Additionally, lobbying for government subsidies to offset the research and development costs of lighter-weight mobility equipment should also be considered to prevent caregiver injury and transportation challenges associated with lifting and dismantling heavy equipment.
Strengths and limitations
CMC represent a medically diverse population with varied medical, physical, and psychological needs [3]. A strength of this study was that the families included reflected this population’s diversity and needs. However, this study also had limitations. The authors studied families from a single state, which may limit generalizability. Also, the analysis of family transport was limited to personal vehicles because it was the preferred mode of transportation of families with children with special healthcare needs reported in the literature [2]. Additionally, ride-share and inadequacies of non-emergency medical transport have been previously discussed [38, 39].
Conclusion
Riding in the family car is a routine and integral part of US culture. However, many families with CMC experience hardship due to transportation challenges that are multifactorial and affect all phases of travel, including transitioning in/out of the vehicle and safety and comfort during travel. These challenges negatively impact child and family safety, well-being, finances, and access to community and medical services. Health care providers can support families with CMC by identifying transportation challenges, tailoring solutions to the family’s unique needs, and advocating at a larger policy level to promote change.
Footnotes
Acknowledgments
Thank you to Breanna Watson for her assistance with the interviews. This work was supported by the Thomas Wilson Foundation.
Conflict of interest
The authors have no conflicts of interest to report.
Ethical considerations
IRB Approval number: IRB00228817, January 7, 2020 –January 6, 2021. Informed consent was obtained for all participants.