
Abstract
PURPOSE:
Down Syndrome (DS) is characterized by intellectual disability, hypotonia, and joint laxity. Physical disability can be an additional problem and manifests as reduced lower limb muscle strength and impaired balance. The objectives of this study were to characterize DS dynamic foot-ground contact area and to study its relationship with balance impairment among adolescents with DS.
METHODS:
Twenty-eight children and adolescents with DS and 28 non-DS adolescents/children were matched for age and sex. The Oxford Ankle Foot Questionnaire (parents’ version) was used to measure disability related to ankle/foot problems in all subjects. A pressure-sensitive mat was used to assess the contact area and arch index. Also, a Biodex balance system was used for measuring postural stability.
RESULTS:
There were significant differences between both groups in all domains of the Oxford Ankle Foot Questionnaire, overall contact area, and arch index (p < 0.05). Overall postural stability index was significantly decreased in subjects with DS (p < 0.05). There was a nonsignificant correlation between contact area and postural stability (p > 0.05).
CONCLUSION:
Adolescents with DS exhibited larger mid-foot and forefoot contact areas with respect to non-DS matched children. Impairment of balance in adolescents with DS is a multifactorial problem not related to changes in the foot contact area.
Introduction
Postural control/balance requires two different processes: the motor adjustment process which is involved in executing coordinated and properly scaled musculoskeletal responses, and the sensory organizational process in which multimodal sensory systems including the somatosensory, visual, and vestibular ones are involved and integrated within the central nervous system [1]. Postural control is necessary for activities of daily living, providing accurate and smooth interaction with the environment [2, 3].
Down syndrome (DS) is known for joint laxity, muscle hypotonia, and reduced strength which may result in impaired stability leading to activity limitations and participation restriction [4]. Bio-kinematic chain mobility could be impacted by any minor foot dysfunction which represents the foundation of the human body in standing, walking, and running. Structural alterations within a foot may also contribute to impaired balance in the stance phase of walking [5–7]. Some evidence shows a relationship between foot feature parameters such as length and width, morphological variables of the foot including foot deformities, and static or dynamic postural stability [8]. Pes planus and other structural deformities such as hallux valgus, clinodactyly, and syndactyly of the lesser toe are common among children with DS [3, 7].
Foot deformities can impact overall postural stability [9]. If not diagnosed and treated early, these deformities may persist and progress to more severe pathology [2]. They may also cause serious biomechanical and postural deviations that could negatively affect performance in daily living, play, and school activities [10, 11]. In children with DS, abnormalities in foot pressure and/or hypotonia can result in an alteration in the foot structure and can cause a collapse of the longitudinal arch with resulting foot dysfunction [12].
Individuals with DS can have some degree of delayed motor and postural responses, as well as cognitive and sensory impairments [13] which increase the risk of falls [14]. Postural instability and balance deficits among individuals with DS could be explained by deficits in the postural control regulation system. Reduced postural tone was found in individuals with DS [15] which negatively affects balance strategies and muscular co-contraction. It also results in deficits in kinesthetic feedback coming from hypermobile or lax joints.
The feet are crucial somatosensory structures used for postural control. They provide a direct contact between the body and the ground, and allow us to sense and interact with our environment. Sensory feedback provided by muscle and cutaneous afferents in the foot contributes to the ability to stand upright and to detect both the position and motion of the body in space [16]. Any decline in foot sole skin sensitivity found in those with DS is frequently associated with poorer postural control and an increased risk of falls [17].
Gait analysis for children with DS often reveals external foot rotation which may be used as a strategy for maintaining their balance [18]. Evidence suggests that children with DS are less stable during gait and community ambulation than those without. However, little is known about the relationship between postural stability, contact area between the body and the ground, and the foot arch index. This study aimed to characterize the DS dynamic foot-ground contact area and to study its relationship to balance impairment among children with DS.
Subjects and methods
Twenty-eight children with DS and 28 with typical development (non-DS) were recruited from elementary and middle schools in the city of Hail in Saudi Arabia. The participation of all students was voluntary. Written informed consent was obtained from each participant and their parents or guardians. Children and adolescents with DS ranged from 8–14 years old. Twenty-eight non-DS children/ adolescents with ages ranging from 9–14 years comprised the second group. Individuals in both groups were matched in weight, height, body mass index (BMI), and shoe size (Table 1) but not intelligence quotient (IQ). Adolescents were excluded from the study if there was a history of visual or labyrinthine/vestibular dysfunction, previous lower extremity orthopedic surgery, inability to walk independently, or the presence of a concomitant medical condition or injury that could affect their physical function (e.g. neurological or inflammatory disorders).
Subjects’ physical characteristics and between groups comparison. Data are presented as mean±SD
Subjects’ physical characteristics and between groups comparison. Data are presented as mean±SD
(*) significant difference.
Researchers interviewed the participants and their parents or guardians to explain the study protocol. During the interview, the parents’ or guardians’ agreement was confirmed by signing a consent form. They were also asked to complete the Oxford Ankle Foot Questionnaire (parents’ version) for measuring disability related to ankle/foot problems. All children participated in the following: full medical history including any other medical conditions associated with DS, complete clinical examination, and anthropometric measurements (weight and height) with the BMI calculated for each child. Among those with DS, the associated conditions included foot problems (67%), atlantoaxial laxity (9%), scoliosis (8%), arthritis (5%), and other problems (11%). The study was approved by the Ethical Committee of the College of Medical Sciences, University of Hail.
To assess balance and neuromuscular control, this study used the Biodex balance system (Biodex Medical Systems, Shirley, NY, USA) which consists of a movable balance platform that provides 20° of surface tilt in all directions. The platform is controlled by computer software (Biodex, Version 3.1, Biodex Medical Systems) that can be used as an objective balance assessment [19]. Postural stability is measured using three stability indices: the anterior/posterior, medial/lateral, and overall (OA) stability scores. The OA stability score is reported to best reflect the overall ability of the examinee to balance on the platform [20]. Bilateral stance was assessed at level eight over 20 seconds for all individuals [21]. Participants were asked to step on the platform, look straight ahead, and place their arms across their chests. The base of support width was controlled by the platform grids which were constant throughout the test session. Subjects were always tested with bare feet and eyes open. Children and adolescents in both groups were trained for 1 min to allow adaptation to the machine. Three practice trials and three test evaluations were performed to reduce the learning effect with a mean score calculated from the three tests.
A pressure platform (emed-q100, GmbH, Novel, Munich, Germany) was used to measure the arch index and the foot contact area. The procedure for measuring the contact area was demonstrated to each participant before starting. Participants were asked to walk across the platform at their usual walking speed (Fig. 1) while looking at a rounded colored sticker to keep the gaze away from the pressure platform during measurement. Five passes of each foot were needed to measure the plantar pressure. A trial was repeated if a foot was placed near or on the edge of the platform. The data obtained from an average of the five steps of each foot was used to represent the individual’s dynamic foot contact. Novel’s foot report (Novel, Munich, Germany) was used to provide a foot arch index, numerical measurement of the foot contact, and colored graphs simulating foot placement (Fig. 1). These reports were created immediately after the data collection.
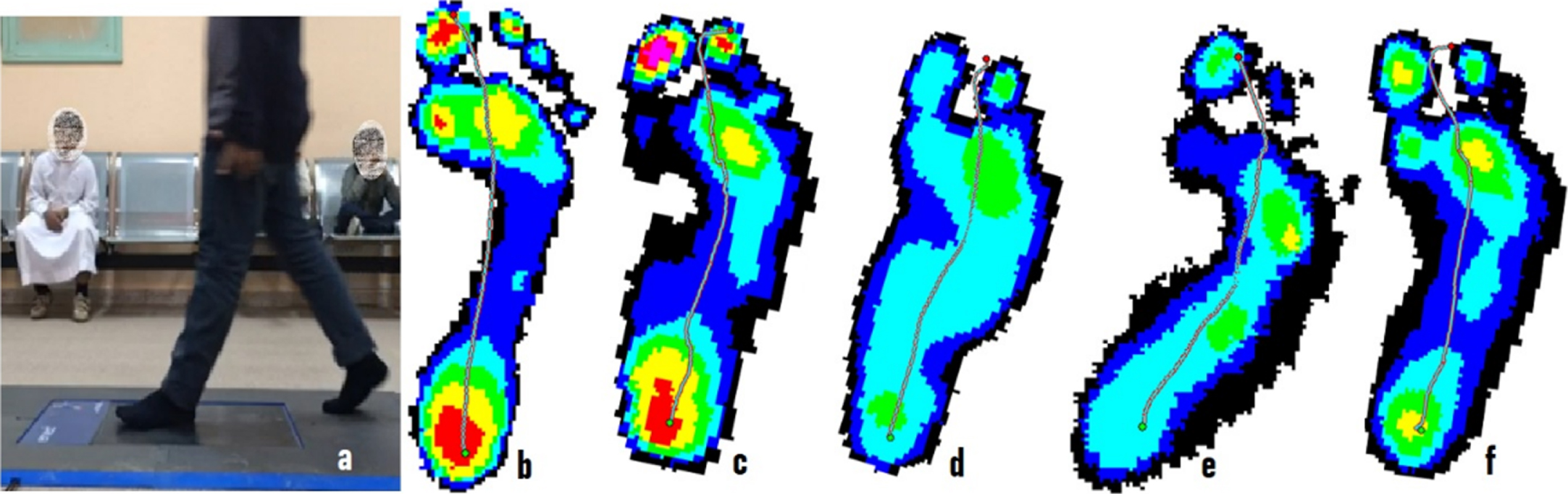
a: Measuring the foot contact area using emed pedography; b: Footprint for a non-DS adolescents; c,d,e, and f: Footprints for adolescents with DS.
After data collection, statistical analysis was performed for foot contact area, arch index, limits of stability measured by the Biodex system, and Oxford Ankle Foot Questionnaire for the two groups using the Statical Package for the Social Sciences SPSS version 20 (SPSS Inc., Chicago, IL, USA). All data were tested for normality by using the Kolmogorov–Smirnov test. The raw data was statistically treated to determine descriptive statistics (mean±SD). Paired t-tests were used to compare the demographic data of all participants. The children with DS were manually matched with those without DS by reviewing records and picking children that were approximately the same age, body weight, height, BMI, and shoe size.
Paired t-tests were used to compare the arch index, maximum force, contact area, postural stability, and the five domains (physical, school and play, emotional, footwear, and clothing) of the Oxford Ankle Foot Questionnaire. The probability value was set to p < 0.05. Pearson Correlation (p < 0.05) was used to study the relationship between the overall postural stability index and arch index, in addition to the contact area for the DS group only.
Results
The physical characteristics of the two groups are shown in Table 1. There were no significant differences in age, weight, height, BMI, or shoe size On the other hand, there were significant differences between IQ (p = 0.001).
Comparison of the data obtained from the parental version of the Oxford Ankle Foot Questionnaire revealed significant differences between the DS and non-DS children (Table 2, Fig. 2). Data recorded in the physical, school, and play domains showed significant differences (p = 0.001). These domains indicate children’s activity limitations and participation. The emotional domain measures how the psychological status could cause activity limitations and decrease the level of participation. Recorded data from this domain demonstrated significant differences between the studied groups at p = 0.001. The footwear and clothing domains are measures of body structure/function and showed a significant difference between the two studied groups (p = 0.001).
Between group comparison of the data obtained from the parental version of the Oxford Ankle Foot Questionnaire. Data are presented as mean±SD (%) for the four domains
Between group comparison of the data obtained from the parental version of the Oxford Ankle Foot Questionnaire. Data are presented as mean±SD (%) for the four domains
(*) significant difference.
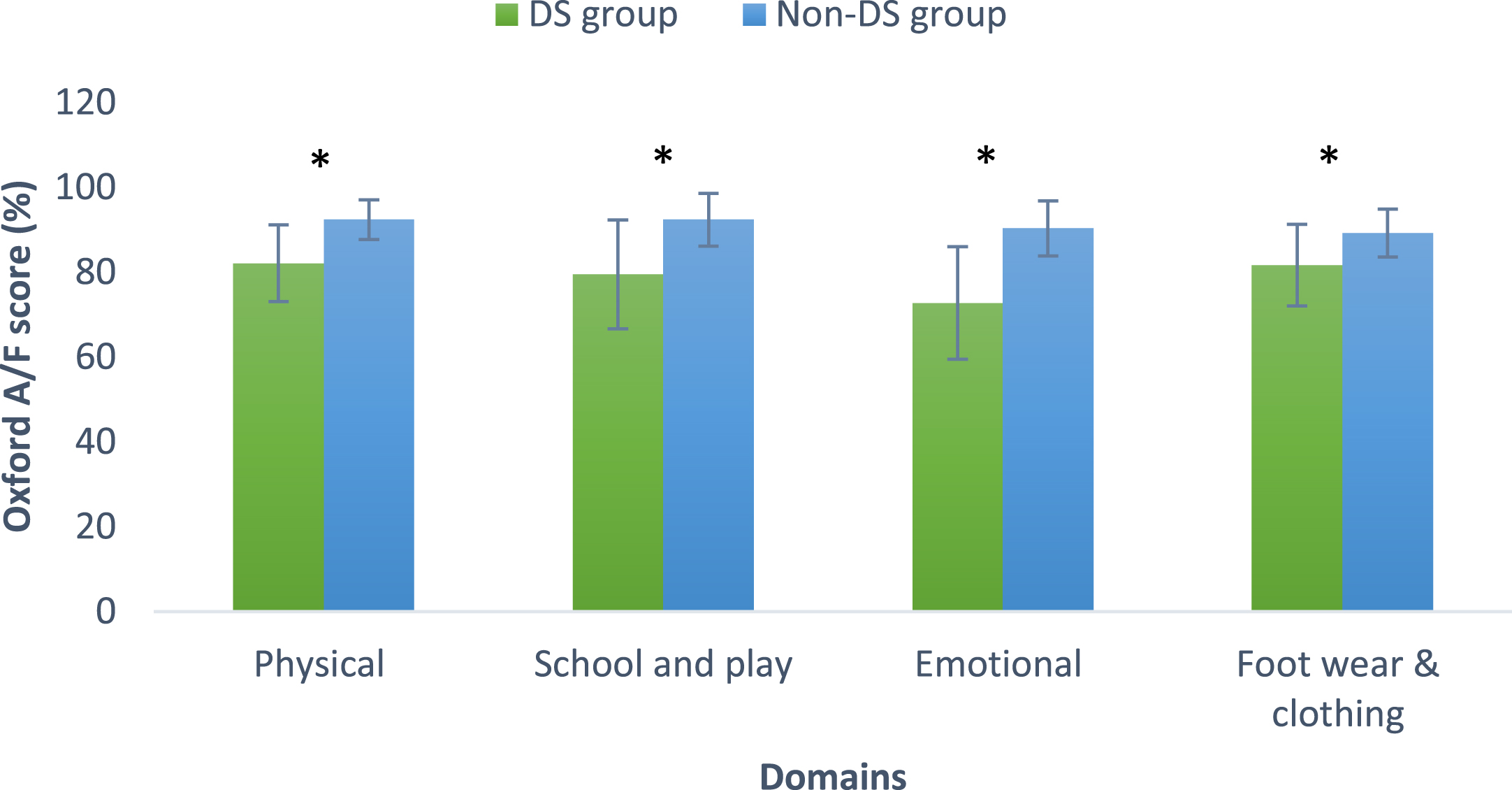
Between groups comparison of the data obtained from the parental version of the Oxford Ankle Foot Questionnaire. Significant differences (*) between children with/without DS were found in all domains (%).
Arch index and contact area of the foot were measured objectively by the emed system and were used as primary outcome measures to study the differences between the children with DS and their non-DS peers Fig. 3. There were significant differences in the arch index (t = 18.69, p = 0.001), overall contact area (t = 3.39, p = 0.002), midfoot contact area (t = 13.24, p = 0.001) and forefoot contact area (t = 8.84, p = 0.001). There was no significant difference between the contact areas of the hindfoot (Table 3). Postural stability testing is a measure of the ability to control the body’s center of gravity within the base of support. There was a significantly (t = 2.55, p = 0.017) reduced ability of children with DS to maintain their center of balance when compared to non-DS age-matched children (Table 3).
Between groups comparison of the contact area measured by the pedography. Data are presented as mean±SD in cm2. Overall postural stability index measured by the Biodex balance system is also presented as a mean±SD
(*) significant difference.
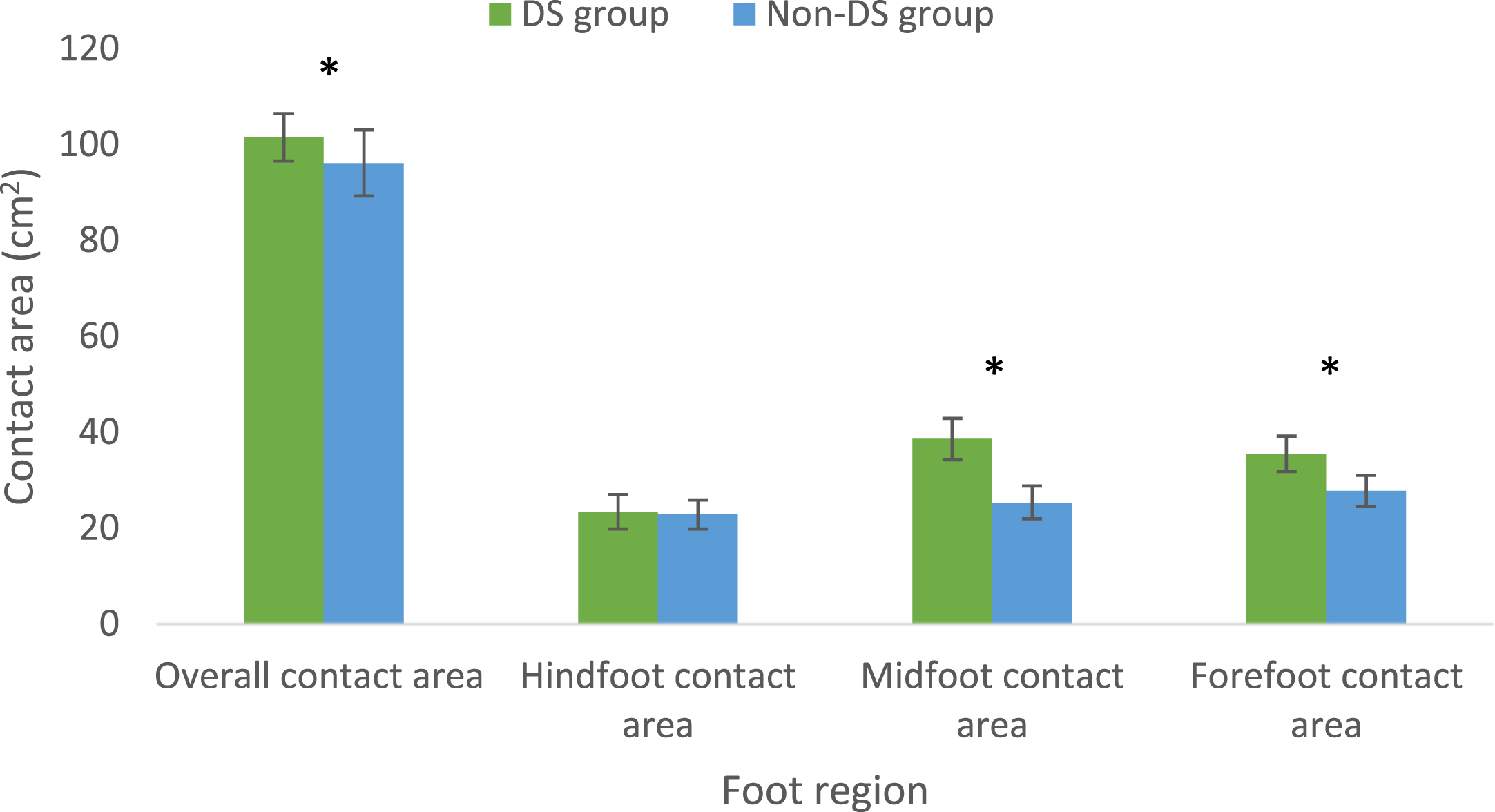
The data obtained from the pedography during walking comparing children with DS to those without. Significant differences (*) were observed between the overall, midfoot, and forefoot contact areas while there was no significant difference in the hindfoot. Data are presented as mean±SD in cm2 ..
Pearson Correlation was used to study the relationship between the impaired ability to control the center of gravity (reduced overall postural stability index), overall foot contact area, and arch index for the DS group only. The correlation between overall postural stability index and total contact area was found to be statistically nonsignificant (r(28) = –0.228, p = 0.338, 2–tailed). Additionally, the correlation between the overall postural stability index and the arch index was considered to be nonsignificant (r(28) = –0.251, p = 0.198, 2-tailed).
This study was conducted to characterize dynamic foot-ground contact area and to study its relationship to balance impairment among children and adolescents with DS. The current study was conducted on DS children and adolescents and matched non-DS children and adolescents with typical motor development. The results showed that those with DS exhibited significantly larger overall, midfoot, and forefoot contact areas as well as decreased arch index with respect to non-DS typically developed children. Increased values of contact area in different foot regions and decreased arch index are largely related to the high prevalence of pes planus in those with DS. This can be caused by generalized hypotonia and ligamentous laxity associated with the presence of a higher average contact area in the midfoot and forefoot. This is consistent with previous studies that confirmed a high prevalence rate of pes planus among children with DS, which was not related to obesity [22, 23]. The results are in close agreement with Pau et al. who tested 99 children with DS of mean age 9.7 (±1.7) using a pressure-sensitive mat to measure overall, rearfoot, midfoot, and forefoot contact area, arch index, and average contact pressure. The values obtained were then compared with those calculated from a sample of age- and gender-matched participants. The authors reported higher average contact pressure in the forefoot and midfoot for individuals with DS [24].
A nonsignificant difference was found in rear foot contact area between children with and without DS. This could be related to the overall changes in the weight distribution mechanism and alterations in the functionality of the foot proprioceptors directly involved in the control of balance. This is consistent with previous studies by Pau and colleagues who reported that changes in body weight distribution are not related to congenital deformities but rather are related to changes in the mechanoreceptors of the foot and ankle [25].
As expected, children and adolescents with DS showed evidence of a significantly decreased overall postural stability index when compared with the non-DS matched children and adolescents. This could be attributed to the fact that children and adolescents with DS have delays in the shift from visual to multimodal control of stance in addition to deficits in eye-hand coordination, laterality, visual-motor control, reaction time, strength, and balance [26].
The results are in close agreement with previous studies which concluded that children and adolescents with DS have worse static balance than their peers without DS and have more problems with altered somatosensory input [27]. Prior studies also compared the muscle strength of the hip abductors and knee extensors between children and adolescents with DS and those without. The authors also concluded that adolescents with DS did not demonstrate the physiological increase in muscle strength that typically occurs by 14 years of age [28, 29]. Moreover, postural deficits have been demonstrated among children and adolescents with DS. Postural reactions to the loss of balance were slow in young children and adolescents with DS, and inefficient for maintaining stability that could be related to defects within higher-level postural mechanisms [26]. Another study done by Conolly et al. compared the motor skills of children with and without DS and concluded that children with DS scored significantly lower in the balance subsection of Bruininks-Oseretsky Test of Motor Proficiency than the comparison group [30].
The results of this study showed a nonsignificant correlation between balance impairment and increased foot contact area. This is not consistent with the idea that increasing the contact area is associated with improved balance as the base of support is increased as well. This could be because of a change of the proprioceptor feedback, delayed postural response to balance loss, or decreased proximal muscle strength. This is consistent with Polastri and Barela who concluded that postural dysfunctions are commonly found in children with DS and associated with impaired proprioceptive feedback, impaired sensory-motor integration, and decreased reaction time for anticipatory postural adjustment [31].
The ability to control equilibrium and stability is an important requirement for functional activities. Failure in this control can seriously limit activity and community participation. Thus, it is essential to improve the static and dynamic balance of adolescents with DS. In general, their condition often results in inactivity which may contribute to even worse postural control. Therefore, individualized training programs could improve balance in these children. Considering the results of this study, these programs should focus on somatosensory input and performing coordinated musculoskeletal responses by improving muscular strength and coordination.
The limitations of the study included the use of the two steps technique which allowed the participants to walk across the platform at a self-selected speed. While individual variations in the selection of walking speed may have affected the results, this impact is likely minimal [32]. Moreover, it is hard to control the speed of walking among children and adolescents at this age, especially in those with low IQ. The sample size of the study was small. Future studies can be done with a larger sample size to enhance the applicability of the results. Including adolescents with vestibular/labyrinthine dysfunction and visual impairment may help to better understand the balance deficits among the DS population.
Conclusion
Adolescents and children with DS exhibited larger midfoot and forefoot contact areas with respect to non-DS matched adolescents. Impairment of balance in children and adolescents with DS is a multifactorial problem not related to changes in the foot contact area.
Footnotes
Acknowledgments
The authors declare that there no organizations that funded this research.
Conflict of interest
The authors declare that there is no conflict of interests regarding the publication of this article.