
Abstract
PURPOSE:
The aim of this study was to evaluate the feasibility and effectiveness of the Parent Empowerment Program (PEP) to help caretakers deliver a home program to promote developmental activities and gross motor function in their children with Down syndrome.
METHODS:
Parents attended a 14-month program with training sessions 1–4 times a month. Outcomes were measured using a change in the Gross Motor Function Measure (GMFM-88) at baseline and assessment one.
RESULTS:
Forty-eight families participated in the PEP. Children’s mean age was 16.2
CONCLUSION:
This study describes a clinically applied research that focuses on program design, development and evaluation. Findings indicate that the PEP is effective in improving gross motor function in children with Down’s syndrome in Pakistan. Parents were satisfied with the program outcomes and were able to cope with the requirements at home. The PEP had favorable outcomes and may be an effective method to support PT services in resource poor countries.
Introduction
Down syndrome (DS) is one of the most common birth defects in the United States with an estimated birth prevalence of 14 per 10,000 live births [1]. The global prevalence of DS is not well known due to lack of birth defect registries globally [1]. Presson et al. have estimated that the population prevalence of DS is 8.27 per 10,000 population [1]. In recent years, quality of life for people living with DS has improved due to successful clinical interventions and community programs to promote societal inclusion and acceptance of these individuals [2]. In the developed world, the estimated life expectancy of persons with DS has increased from 12 years to 60 years [3]. However, in developing countries like Pakistan, little is known regarding the prevalence of this disorder and suitable interventions in the family or community context [4].
DS is associated with a high prevalence of co-morbid conditions and decreased mortality across body structure and function systems (e.g., cardiac, gastrointestinal, immunological, respiratory, sensory, and musculoskeletal) [3]. Pneumonia is known to be the most common cause of mortality in patients with DS across the lifespan [3]. Congenital heart defects are the most common cause of morbidity and mortality in childhood (13%) and adulthood (23%), whereas coronary artery disease (10%) and cardiac, renal, and respiratory complications (9%) are reported in adult patients with DS [3].
Developmental delays are also common in children with DS [5, 6]. Compared with age-matched controls, children with DS spend 0–18 months working on the ability to sit and move on the floor. By 18 months–3 years, children with DS work on learning to stand independently and walk. By 3–6 years, they are working on the ability to run, jump, climb-up and down stairs. The predicted motor outcomes of 121 (Canadian) children, ages 0–6 years, with DS have been discussed in detail by Palisano et al. [7]. According to this study, 91–98% of children with DS stand between 2.5–3 years of age. Walking is achieved by 92–99% of children with DS by 3–4 years of age, and running, climbing steps and jumping are achieved by 67–84% of children by 6 years respectively [7]. This was used as a historical guideline in motor milestone development in children with DS at Karachi Down Syndrome Program (KDSP). Despite being used for a population that differs by ethnicity, culture, and child rearing practices substantially, there is no such data that exists for children from Pakistan or other parts of the developing world to the best of the authors’ knowledge. Pereira et al. used Alberta Infant Motor Scale (AIMS) to evaluate infants with DS (
Unlike the United States, which mandates early intervention under the Individuals with Disability Education Act (IDEA) [12], in Pakistan, there is no such system in place. There is a lack of physical therapists (PTs) trained to provide early intervention services to families with children with DS. Furthermore, there is no medical insurance program to pay for these services. Those who receive therapy sessions do so in hospital or outpatient settings. There is very limited home-based therapy which has been shown to be effective because the child is in the natural environment [13]. Parent child interactions in the home environment are known to have a positive effect on short and long term developmental outcomes [14]. Therefore, we sought to empower parents to provide home-based therapy to improve motor and psychosocial development as a method to provide a ‘physical therapy-like program’ in the absence of trained pediatric therapists.
Methods
This was a preliminary feasibility study to examine effectiveness of the Parent Empowerment Program (PEP), which was conducted during February 2016–April 2017 at KDSP in Pakistan. Launched in 2014, KDSP is a not for profit organization (a Non-Government Organization [NGO]), whose vision is to enhance the quality of life of children with DS and make them valued members of the family as well as the community [15]. The aim of this feasibility study was to (1) describe a clinically applied research design that focuses on program design, (2) develop and evaluate the feasibility of a pilot Parent Empowerment Program to deliver a home intervention in order to promote developmental activities and gross motor function in children with DS. This kind of program is consistent with current models of early intervention in which the daily involvement of the parent and family in fostering the child’s early development is the most important factor in facilitating the child’s improvement [16]. We also evaluated the association of comorbid conditions with Gross Motor Function Measure (GMFM-88) scores that may affect development of gross motor function during the program.
The eligibility criteria for the study were children with DS between the ages of 0–5 years. The GMFM-88 was used to measure the child’s gross motor outcomes because it is a standardized gross motor test for children 0–5 years which has been validated to assess gross motor function in children with DS [17]. It is comprised of 5 dimensions that represent different categories of gross motor development (A: Lying and Rolling; B: Sitting; C: Crawling and Kneeling; D: Standing; E: Walking Running and Jumping). The advantages of this tool are that parents can provide item responses when children are not cooperating in item performance. They can also add testers’ observations of more difficult motor items, which allow them to ‘pass’ the child on precursor or lower skill items in that dimension. Also, for children older than 3 years of age who have achieved higher level motor function, only dimensions D (Standing) and E (Walking Running and Jumping) are used [18].
Parents of children with DS were identified and recruited from KDSP. A sample of convenience was used in this study. We did not need an IRB for this study. KDSP is an NGO (Non-Government Organization), and no formal IRB is in place. Additionally, since a caretaker or parent at home was performing therapy, an IRB was not deemed mandatory. A signed parental consent was obtained despite lack of an IRB because we wanted parental permission to use some of the videos of their children in teaching sessions as resources for other parents. Enrollment was done on a first come first serve basis. Parents were educated verbally and by using videos during therapy assessment of their child. They also attended a baseline parent session in which PEP was explained, and they signed consent forms when they agreed to participate. Our goal was to enroll 50 parent-child pairs. We achieved 96% of our enrollment goal and stopped enrollment at 48 families due to our project timeline. Parents then attended ongoing physical therapy sessions in which they were trained and instructed in home activities to promote developmental skills and gross motor function in their children with DS. In addition, they attended a training/coaching program 1–4 times a month. A trained pediatric therapist lectured and showed videos of treatment sessions being done on other children enrolled in the study (with consent of parents). Actual demonstrations of typical developmental activities, including positioning for lung development, neck holding activities in sitting and prone positions, rolling activities, anti-gravity flexion (i.e., pull to sit and sitting balance), standing balance activities (i.e., standing against wall reaching in all directions), overhead ball throwing activities in sitting and standing, assisted trampoline jumping, stair climbing, climbing up and down a ramp or uneven ground and obstacle course (i.e., stepping over a book or toy) were stressed. The importance of transitional movements was impressed upon the parents in coaching sessions and during therapy because transitional movements are precursors to earlier walking abilities [19]. Mothers were also educated on when to use supra-malleolar orthosis (SMOs) to aid standing balance and walking [20, 21, 22] and the importance of child-initiated movements and task-specificity in therapy (i.e., sit to stand and reach for a toy placed on a shelf) [23]. Practice sessions of the above named developmental activities comprised of small groups of 3–4 parents were encouraged during training. Each group had a pediatric therapist who acted as a facilitator.
In a typical therapy session with the concerned child, the mother was given the opportunity to work with her child, whilst the treating PT observed and assessed the pair to encourage confidence on the part of the mother. The therapy session also included brief hands-on therapy of the child by the treating therapist, whilst the mother videotaped the entire session for replication at home. This was repeated 1–4 times a month per parent-child pair according to the needs of the child and the availability of the parent. Because some parents lived far from the therapy center, they decided to commute once or twice a month.
Parents agreed to attend training sessions 1–4 times a month, depending on their availability and their child’s needs. During these training sessions parents’ queries and skills were addressed by the treating therapist, in order to support and promote their interaction with their children. This increased the parents’ confidence and simultaneously promoted the child’s motor and psychosocial development in the long run (See Fig. 2).
A project PT was trained in PEP outcome measures (administering GMFM-88 at baseline and assessment 1). During the 14-month long program, the same PT collected data at baseline and at two assessment sessions, which were 4–6 months apart. Two months were used for recruiting and 8–12 months were designated for the completion of PEP. Descriptive and process data were obtained from PEP attendance records and from parents via interview. Details regarding co-morbidities, including cardiac anomalies, vision and hearing defects, and previous hospitalization were obtained via parent interview.
In order to measure compliance with PEP, parents kept diaries/logs which were checked by the treating therapist regularly once a week, twice monthly or once monthly depending upon the frequency of treatment received by the child and how often the parent sought guidance from therapist. Parents living far from the center sent videos via WhatsApp or email once a week to ensure they stayed on track. They were highly motivated and thankful that correct guidance/instructions on PT management were being given for their children, in a country where (1) children with DS are hidden at home due to shame or denial on the part of the parents and nonacceptance or noninclusion on the part of the Pakistani society and (2) where physical therapy is considered a luxury and basic medical help is a blessing not an expectation. A parent was considered to be adhering to the PEP if he/she performed 20–30 minutes of prescribed activities with their child every day.
The justification of this pilot feasibility program/ model was the fact that the treating therapists had the opportunity to see the child 1–4 times a month and determine therapy intervention as the child progressed or showed improvement. This progression of therapy intervention by the treating therapist was important because the mothers, although highly motivated in this cohort, did not have the skill set to assess the progress and change treatment goals/objectives and treatment recommendations over time as their child improved. At re-evaluation sessions, videos taken by the caretaker/ parents and diaries/logs of frequency and intensity of sessions performed at home were assessed by the treating therapist.
Developmental activities were measured using the GMFM-88 scoring system. This is a universally accepted scoring system for children with disabilities [7]. The GMFM-88 has been translated into multiple languages and is an international gold standard to measure gross motor capacity in children with DS or CP [24]. PEP outcome measure was the change in GMFM score between baseline and assessment one.
Data analysis was conducted using SPSS 20. To determine program effectiveness, a paired
Results
Forty-eight families who had children with DS were enrolled in this study. Mean age of the participants was 16.2
Baseline characteristics of study participants
Baseline characteristics of study participants
Cardiac anomalies in the study participants
Change in GMFM score at baseline and assessment one.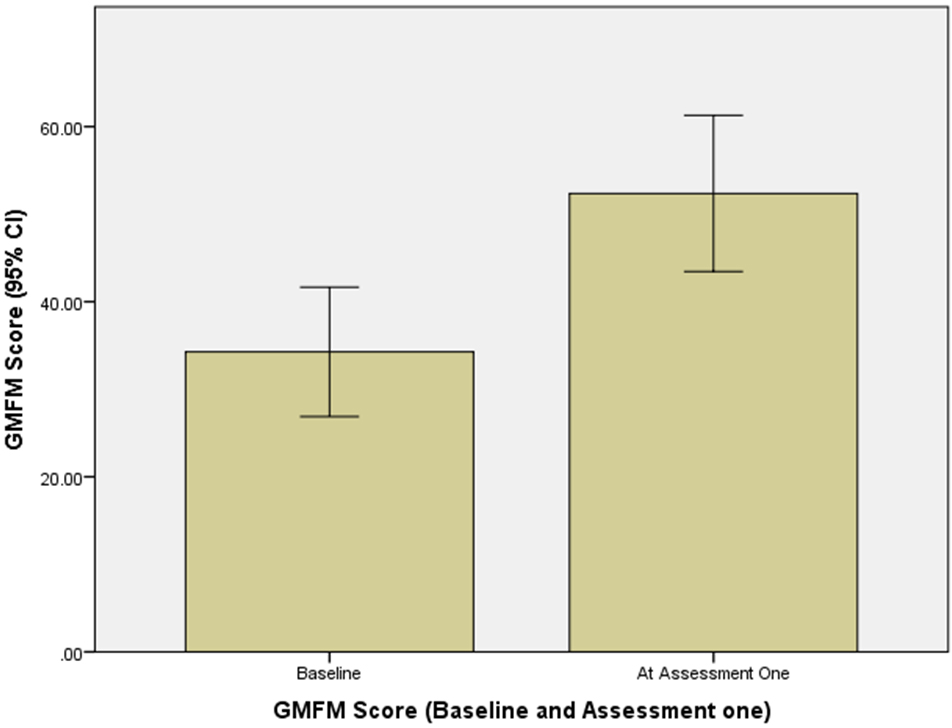
Example of sitting balance and walking activities that parents learned during the PEP sessions.
Parent adherence to the PEP at home and in ongoing training sessions was 69%. At assessment 1, there were 32 participants (67% retention) while at assessment 2 (4–6 month interval), only 11 participants returned (23% retention). Parents who did not attend assessment 2 reported that their children had achieved walking goals and that they no longer required PEP. Due to the high attrition rate at assessment 2, the GMFM-88 scores were only compared between baseline and assessment 1 (which occurred at the 4–6 month interval from baseline). There was significant improvement in GMFM-88 scores between baseline and at assessment one, t (30)
Previous hospitalization significantly affected GMFM scores both at baseline and assessment one. Children with no previous hospitalization, t (6)
This study showed that the PEP model was effective in improving gross motor function in children with DS in a resource poor country like Pakistan. The IDEA reports that for infants and toddlers, natural settings such as the home environment is most conducive to learning activities and therefore promotes early home based interventions [12]. Sayers et al. reported that parent-implemented, home-based pediatric intervention program for children under 5 years of age with DS empowered parents to provide developmental and motor skill building activities and was perceived to be worthwhile by families [25]. Findings from early motor interventions also suggested significant changes in the motor development and quality of movement of children with DS over the course of therapy [26].
Similar findings were reported at the first baseline assessment in our study. Parents in our cohort were highly motivated partially because they met with other parents who achieved success with their children, which was defined as ability to walk with or without support within 6 months of the PEP. This reinforcement from other parents and their success stories further motivated newer parents in the PEP. Anecdotally, according to parent interviews, this sharing and support among parents was an important characteristic of PEP success. However, there was a high attrition rate at the second assessment (8–12 months into therapy) mainly because children reached their goal of independent walking. Hence, parents were not willing to pursue further therapy. In the future, it may be important to expand the goals of PEP beyond walking abilities to provide support to parents on other developmental challenges (i.e., fundamental movement skills like running, jumping, throwing and catching, fine motor skills, social skills, and school and community skills) that will occur as their child ages, has more experiences and encounters the natural environment outside of the home.
Cardiac structural and functional defects are commonly reported in children with DS [27]. It is also appreciated that there is a high prevalence of functional limitation and activities of daily living after cardiac surgery in children [28]. Our cohort had very few children who required cardiac surgery mainly because the majority of the defects were relatively minor, such as Patent Ductus Arteriosus (PDA), and did not require surgical intervention. This might be one reason why we did not see any effect of the cardiac defects on motor development in our cohort. Repeated hospitalizations were significantly associated with lower GMFM-88 scores. Most of the children in our study had repeated respiratory tract infections, which necessitated intravenous antibiotics and respiratory therapy. This seemed to have a negative impact on their motor scores. The finding that repeated respiratory tract infections had a negative impact on the motor scores of children in our cohort is supported in the literature [29]. This suggests that perhaps it would be important to have hospital based PT services or developmental activities and mobility services for children with DS so that they do not regress during inpatient stays.
The PEP developed for this study is a good example of a system that may be applicable to other developing countries, which have few trained pediatric physical therapists. Furthermore, it is important to consider the socio-economic and cultural aspects in the development of parent education programs for children with disabilities [30]. Such a program may be the solution for helping children with DS in resource-strained settings such as Pakistan.
This study has several strengths and limitations. It helped establish a socio-economically viable option to improve parents’ confidence in working with their child with DS. In resource poor countries, this is a realistic mode of delivering quality therapy to children who, due to financial and logistic issues, including absence of trained/qualified pediatric PTs, would otherwise not receive any interventions. Empowering mothers and caretakers also benefits the child. A home environment and working with a familiar and trusted caretaker optimizes the child’s responses to therapeutic activities. The mothers’/caretakers’ high motivation was an important factor that cannot be underestimated, and it is very probable that this contributed to the success of the program. Parental involvement was the main objective of the PEP. However, the small sample size (
Conclusion
In conclusion, PEP is an effective model to promote gross motor functioning in children with DS in resource poor settings. Future work is required in a larger community-based outreach program to empower parents, deliver developmental and gross motor activities, consider broader program goals, and conduct in-depth stakeholder interviews to determine new directions for the PEP. Logically, the next step would be to develop a “train the trainer” program and recruit mothers of children with DS who have gone through the PEP to be community support for other new parents. This would be an economically viable training system, which would engage the parents of children with DS, promote community participation and improve the functional outcomes for children with DS.
Footnotes
Conflict of interest
The authors have no conflict of interest to report.