
Abstract
PURPOSE:
To determine characteristics associated with self-management independence and quality of life (QOL) among adolescents and young adults with spina bifida (AYASB) engaged in a spina bifida (SB) health care transition clinic.
METHODS:
During SB transition visits, Eighty-eight AYASB ages 14-20 completed the Adolescent/Young Adult Self-management and Independence Scale II Self-Report/SB (AMIS II-SR/SB), scores ranging from 1–7 with 7 indicating full independence in activities, and the QUAlity of Life Assessment in Spina bifida for Teens (QUALAS-T), which has two subscales, family/independence (QFI) and bowel/bladder (QBB), with scores ranging from 0-100 with 100 indicating maximal QOL score. Demographic and clinical variables were collected from the electronic medical record.
RESULTS:
The baseline AMIS II-SR/SB score was 3.3 (SD 1.0). Baseline scores for QUALAS-T QFI and QBB subscales were 73.8 (SD 19.9) and 63.8 (SD 25.8). Older age was associated with a higher baseline AMIS II-SR/SB score (p = 0.017). Over time, AMIS II-SR/SB total significantly improved (p < 0.001), but QFI and QBB did not. AYASB not on chronic intermittent catheterization (CIC) and those using urethral CIC significantly improved in AMIS II-SR/SB total scores (p = 0.001), but those using abdominal channel CIC did not.
CONCLUSION:
Baseline bladder management method was associated with self-management improvement for AYASB engaged in a SB-specific transition clinic.
Introduction
Spina bifida (SB) is the most common neural tube defect with an estimated global incidence of 0.7–42.8 per 10,000 births per year [1]. Given SB’s lifelong impact on an array of organ systems, multiple daily self-management tasks such as bladder catheterization, bowel regimens, and skin checks, are required. Self-management is the set of behaviors that individuals with chronic health conditions engage in to optimize their health and well-being such as medication/regimen adherence, symptom monitoring, complication prevention/management, and care navigation [2]. Self-management support is considered an essential component of health care transition from pediatric to adult care for adolescents and young adults (AYA) with complex conditions such as SB [3, 4]. For the purposes of this study, transition is defined as “the process of moving from a child/family-centered model of health care to an adult/patient-centered model of health care. The transition process involves planning, transfer, and integration into adult-centered health care” [5].
AYA with SB (AYASB) may experience more difficulty in acquiring self-management skills compared to other AYA because of SB-related executive function deficits such as higher order planning, mental flexibility, focused attention, ability to shift attention, working memory, and problem solving skills [6–9]. Thus, self-management support for AYASB not only involves the implementation of necessary skills and behaviors for condition management, but also the developmentally appropriate hand-off of self-management responsibility from the parent/caregiver to the individual [10].
Striking the balance between maximizing self-management independence and meeting the extensive care needs of AYASB is a complex challenge. Indeed, higher independence correlates with increased family relationship satisfaction and decreased urinary tract infections, hospitalizations, and depression/anxiety highlighting the priority of self-management intervention for this population [11–14]. However, due to the range of condition severity, neurocognitive ability, and physical ability in this population, only one-third of adults with SB gain full independence while one-third still need supervision or occasional help and the last third routinely need assistance for care tasks [15]. Understanding the demographic and clinical factors associated with self-management independence has important implications for transition preparation such as planning for daily care needs, independent living supports, funding for such services, and higher education/employment opportunities. Additionally, understanding how self-management independence relates to health related quality of life (QOL) can help align interventions with patient priorities [3]. However, to date there is limited knowledge about factors associated with self-management, independence and potential for improvement as well as QOL for AYASB during transition.
This study sought to determine [1] demographic and clinical characteristics associated with baseline self-management independence and SB-related QOL and [2] demographic and clinical characteristics associated with self-management, independence and QOL changes over time for AYASB engaged with a tertiary pediatric hospital SB transition clinic program. It was hypothesized that younger age, increased physical impairments (i.e., having a higher SB lesion level and non-ambulatory status), increased needs for learning support, and more involved bowel or bladder regimens requiring the use of enemas or catheterization may be associated with lower self-management independence scores at baseline and less improvement over time. Additionally, it was anticipated that minority race/ethnicity status, being from a primarily non-English speaking household, and not having private insurance may be associated with lower baseline and subsequent self-management scores as these individuals may have additional barriers to attaining independence. Regarding QOL, studies suggest that adolescents with SB may perceive their QOL to be higher than adults with SB [16]. Comparatively, adults with SB experience increased barriers in relationships, employment, and independent self-care as well as a potential decline in health status and more pain [16, 17]. Thus, it was hypothesized that as AYASB in the program may have relatively stable health and have not yet encountered many of these emerging adult challenges. Thus, QOL scores may be relatively high and not have significant change over time.
Methods
Clinic setting
The Texas Children’s Hospital SB Transition Clinic is a comprehensive SB-specific transition clinic program based on the Six Core Elements of Health Care Transition ™ and the Chronic Care Model [18–20]. In the Texas Children’s SB program, AYASB ages 14 and above continue to follow up in the SB multidisciplinary clinic annually and the transition clinic every 3–6 months until transfer to adult care between ages 19–21. During a transition visit, an internal medicine-pediatric physician, nurse, and social worker provide SB-specific comprehensive transition planning based on the Spina Bifida Association’s Transition Guidelines [20–22]. The transition care provided includes chronic condition management, adolescent health counseling, funding/education/employment planning, care coordination, and goal-setting self-management support specifically for AYASB.
Transition self-management support
To support self-management in the transition program, the clinic team developed a self-administered questionnaire to categorize patients’ bladder, bowel, and skin self-management ability into a hierarchy of levels. In the assessment, level 1 describes independence in basic tasks such as bladder catheterization, bowel evacuation regimens, and skin self-examination. Level 2 describes independence in adherence to tasks without a caregiver prompting. Level 3 describes independence in preventing and managing complications such as urinary tract infections, constipation or bowel accidents, and skin ulcers. Level 4 describes healthcare navigation independence in activities such as ordering medications or supplies and making appointments. Questionnaires were completed during the visit by patients and their parents. Then, a clinic provider is assigned a level for each domain based upon the questionnaire responses. Afterward, the clinic nurse, patient, and the patient’s parent developed a goal and action plan for one or two self-management domain(s) based on the level assigned, patient preferences, and chronic condition priorities. As an example, a goal for bladder level 2 would be to catheterize on time without the caregiver prompting. The action step would be to write down a schedule and use a phone or watch reminder. Goals were followed up at clinic visits every 3–6 months. The clinic nurse was available for assistance by phone between visits as needed.
Participants
After receiving approval from the Baylor College of Medicine Institutional Review Board, AYASB established with the transition clinic were recruited for participation in the study. As the study cohort was a convenience sample of the patients who were able to complete surveys during their transition visit, there was no prior power analysis conducted. Inclusion criteria were: 1) AYASB ages 14–21 with myelomeningocele, myelocystocele, lipomeningocele, or sacral agenesis/congenital tethered cord, and 2) with the ability to read and answer questionnaires independently. AYASB not established with the transition clinic, those with inability to answer questionnaires independently, those with acute medical concerns (i.e., fever, wound, malaise, etc.), and those who were not able to give assent (age less than 18 years) or consent (age 18 years or older) were excluded. Consent for participation was given by the parent or guardian accompanying the adolescent if younger than 18 and by the young adult if older than 18. Consent was re-established annually.
Measures and procedures
During their transition visits, participants completed baseline Adolescent/Young Adult Self-management and Independence Scale II (AMIS II-SR/SB) and the QUAlity of Life Assessment in Spina bifida for Teens (QUALAS-T) questionnaires using SurveyMonkey® on iPad tablets [23, 24]. The AMIS II-SR/SB is a 36-item self-reported questionnaire examining self-management independence developed as a parallel to the AMIS II-interview version by an interdisciplinary team of researchers, Sawin, Brei, Holmbeck, Pasulka in 2013 [25]. The AMIS II-SR/SB includes 8 SB condition-specific self-care questions and 28 general self-management activities. Responses are on a Likert scale ranging from 1 (never/rarely less than 25%on my own) to 7 (Always, over 90%all on my own). The question responses were averaged to give the total AMIS II-SR/SB score. While subscales were developed for the interview version of the AMIS II, they have not been validated for the AMIS II-SR/SB, thus only the total AMIS-SR/SB was used. The QUALAS-T is a 10-item QOL assessment for AYASB ages 13–17 describing satisfaction in family/independence (QFI) and bowel/bladder continence (QBB) domains. The subscale scores range from 0–100. Patients continued to follow-up for transition visits ideally every three to six months for planning and goal setting. The AMIS and QUALAS-T were repeated during these standard clinic visits every 6–12 months.
Demographic and clinical data were collected using the electronic medical record.
Demographic variables included patient gender, age, race/ethnicity, primary household
language (English or Spanish), and primary insurance (private or public including Medicaid
or Children’s Health Insurance Plan). SB-related condition variables were based on the
Center for Disease Control and Prevention’s National Spina Bifida Registry measures [26]
including: 1)
Data analysis
Patient demographics and clinical characteristics were summarized using means with standard deviations, medians with minimum and maximum values, or frequencies with percentages. Independent linear regression was used to test the association between patient characteristics and baseline QUALAS and AMIS II-SR/SB scores. Factors found to be significant at the p < 0.05 level were considered for inclusion in a multiple linear regression. Backwards elimination followed by forward re-entering of variables was used to find more parsimonious regression models. Due to low frequencies, race/ethnicity categories for ‘African American/Latino’ and ‘mixed’ were combined while the bowel category ‘colostomy’ was not included in the regression analysis.
Random coefficient regressions with an unstructured variance-covariance structure (unless otherwise noted) were used to test whether QUALAS and AMIS II-SR/SB scores changed over time. This mixed effect model allowed for analysis of each patient’s baseline AMIS II-SR/SB and QUALAS scores and rate of change. To determine whether the change in scores was dependent on patient baseline characteristics, the interaction between time and each characteristic was tested with a separate random coefficient model. Interaction terms significant at the p < 0.05 level were considered for multiple regression. The average change in QUALAS or AMIS II scores over time was estimated with 95%CI for each factor level of those found to be significant. Model contrasts were performed and p-values for pairwise comparisons between factor levels were adjusted for multiple hypothesis testing using Sidak’s method [28].
Results
A total of 88 AYASB participated in the study, which represented 61%of patients, ages 14–20, established with the Texas Children’s SB program. Across demographic and clinical variables, there were no statistically significant differences between patients who participated in the study and those who did not, with one exception. Study participants were less likely to have a history of learning support need than non-participants (p = 0.001) with more non-participants categorized as having a known learning disability or having an IEP. While the majority of the participants completed their baseline surveys at their first transition visit, on average, they were established for 7.05 months before completing baseline surveys. Baseline characteristics are described in Table 1. The average baseline score for the AMIS II-SB/SR was 3.3 (SD 1.0) indicating that on average, AYASB reported needing assistance with self-management activities 50-75%of the time. Average baseline scores for the QFI and QBB subscales were 73.8 (SD 19.9) and 63.8 (SD 25.8), respectively (Table 2).
Summary Statistics
Summary Statistics
Baseline QUALAS and AMIS II score
Only age at the time of the baseline survey was significantly associated with the AMIS II-SB/SR score (p = 0.017), with the average being 0.17 points higher (95%CI: 0.03, 0.30) per older age (Fig. 1). There were no baseline characteristics associated with baseline QFI or QBB.
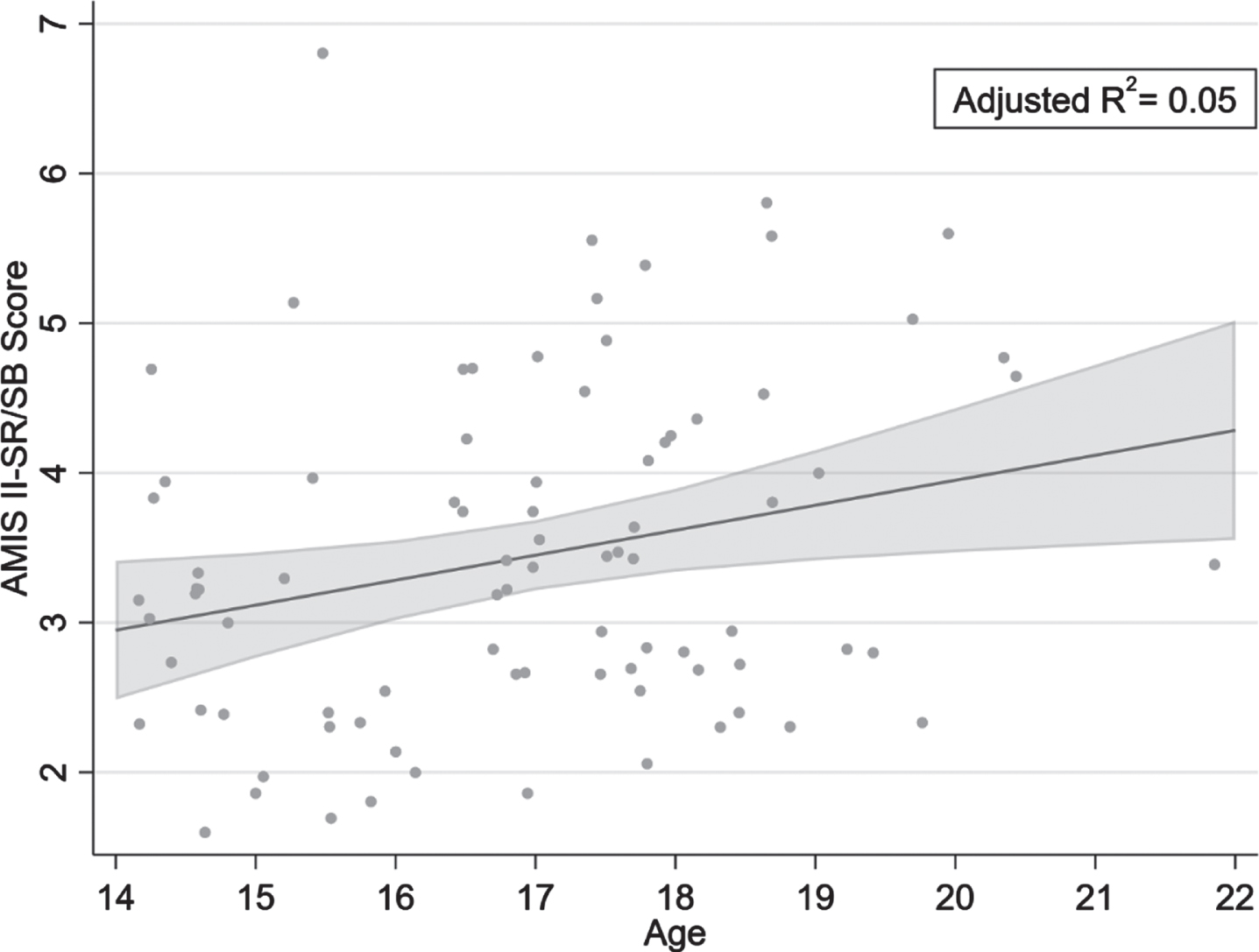
Average Baseline AMIS II-SB/SR Score per Age (with 95%CI).
Using the random coefficient model, the average AMIS II-SR/SB score increased 0.05 points per month (95%CI: 0.03, 0.07, p < 0.001). AMIS II-SR/SB over time was associated with primary language (p = 0.014) and baseline bladder regimen (p = 0.001) using single regression models. When both of these interactions were included in a random coefficient regression, AMIS II-SR/SB over time no longer depended on primary language but did significantly depend on the patient’s baseline bladder regimen (p = 0.001). The average AMIS II-SR/SB score increased by 0.10 points (95%CI: 0.05, 0.16) per month among patients without CIC management, by 0.07 points (95%CI: 0.04, 0.09) per month among patients managed with urethral CIC, and did not significantly change over time for those managed with channel CIC at baseline (p = 0.355) (Fig. 2). Pairwise comparisons showed that compared to patients using channel CIC. Those managed with urethral CIC (p = 0.009) and those without CIC management (p = 0.009) had more improvement in AMIS II-SR/SB scores over time (Table 4). However, there was not a significant difference in the change in AMIS II-SR/SB score between those without CIC management and those with urethral CIC (p = 0.579).
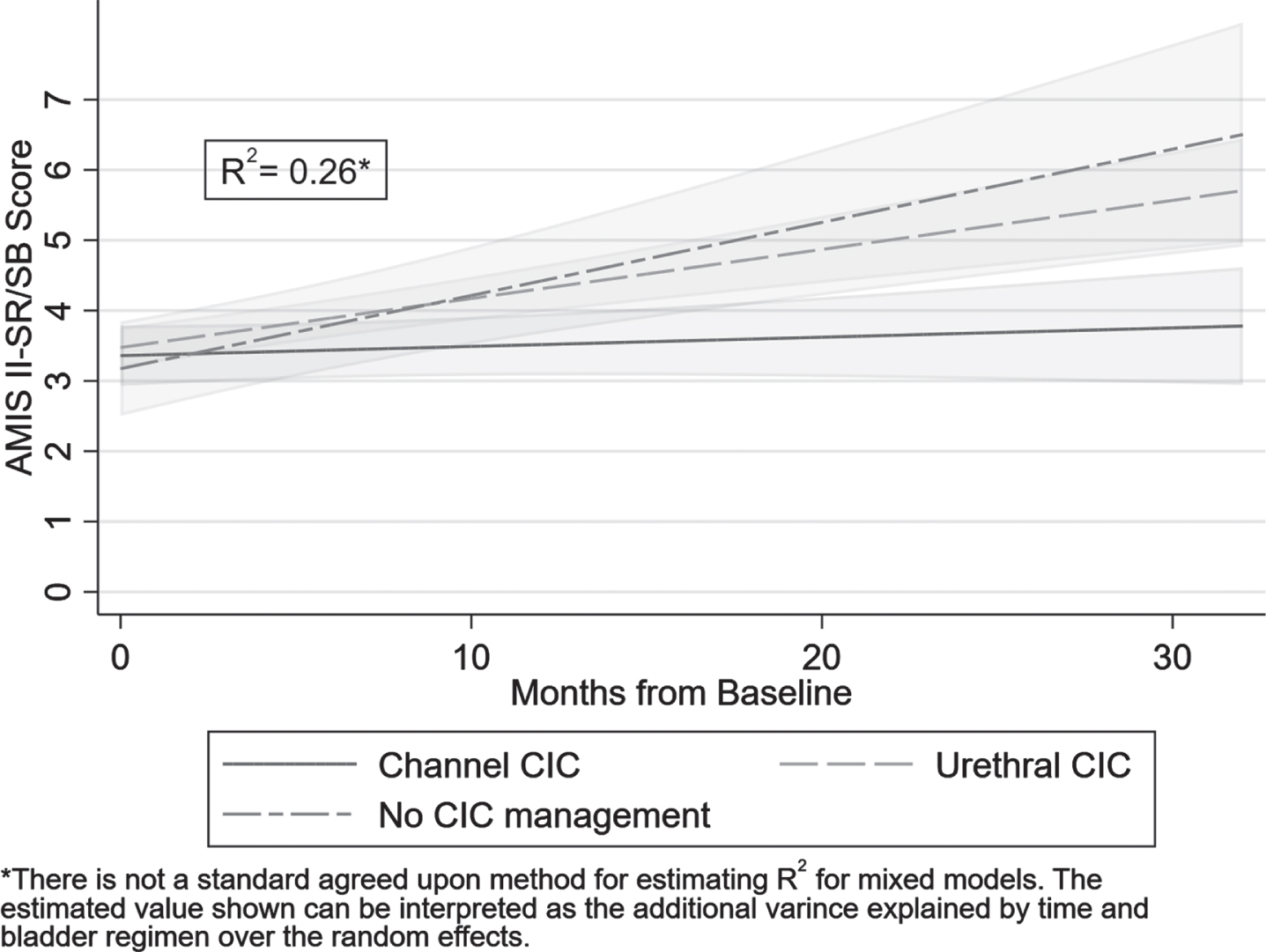
Average AMIS II-SR/SB over time per bladder regimen (with 95%CI).
Comparison of change in AMIS II-SR/SB per month for bladder regimen type
*adjusted for multiple comparisons using Sidak’s method.
P-values for independent linear regressions of variables associated with baseline AMIS II-SR/SB
There were no characteristics found to be associated with baseline QFI or QBB. QFI did not significantly change over time (p = 0.747). The bowel regimen time interaction was significant (p = 0.043) in the model for QFI, but after adjusting for multiple comparisons, there were not any significant differences in QFI over time between any of the bowel categories. Although not significant at the p < 0.05 level, QBB appeared to increase by 0.39 points per month (95%CI: –0.01, 0.78, p = 0.055,). Additionally, QBB over time did not depend on any baseline patient characteristics tested.
Discussion
This retrospective cohort study offers a longitudinal analysis of change in self-management independence for a subset of AYASB engaged in a SB-specific transition clinic. It was found that age was the only variable associated with the baseline AMIS II-SR/SB score. Over time, the AMIS II-SR/SB score significantly improved, and the baseline bladder management type was associated with score improvement. An average AMIS II-SR/SB improvement of 0.05 per month could potentially indicate that AYASB can be expected to improve by 1 AMIS scale point in approximately 20 months. The baseline average AMIS II-SR/SB score was 3.3 (SD 1), and based on the scale descriptions, this indicates the ability to independently perform self-management tasks 50–74%of the time. An increase of 1 AMIS scale point could indicate that AYASB in the program may be able to independently perform self-management tasks more frequently at 75–90%of the time by 2 years. However, there may be a ceiling to this affect due to physical or cognitive limitations or other health/social set-backs. Recognizing limitations in the sample size, none of the variables were significantly associated with QUALAS-T scores at baseline or overtime, and the QUALAS-T score did not significantly change.
Associations with AYASB Self-management independence
In this study, the baseline AMIS II-SR/SB score of 3.3 (SD 1.0) indicated that on average, AYASB with a mean age of 16.1 years were independent 50–74%of the time for activities of daily living and self-care. By comparison, a cohort of 50 AYASB with mean age of 21 years studied by Bellin et al. had an average AMIS II score of 4.5 (SD 1.0) indicating that this older group was independent 75–90%of the time [29]. While age was positively associated with independence at baseline, both the current study and the Bellin study indicate that many AYASB will need on-going care support throughout adolescence and early adulthood. The impairments in executive function skills such as planning, organizing, and problem solving that commonly impact AYASB are likely to impede the acquisition of such self-management activities [30–32]. As such, Davis et al. found that adaptive skill development was 2–5 years delayed in adolescents with SB compared to typically developing adolescents [30]. Understanding the on-going self-management support needs of AYASB, executive function impairments, and likely delay in the development of adaptive skills is important for setting expectations with families during transition planning. AYASB may need more structured supports and practice to accomplish self-management tasks that require several steps such as bladder catheterization or bowel regimens [33]. However, in this study, baseline age was not associated with AMIS-II SR/SB score improvement suggesting that all ages of AYASB can improve their skills and emphasizing the importance of self-management support for all ages during these critical years of development.
The SB lesion level is often used as a marker of condition severity and a significant predictor of functional independence due to its association with physical and cognitive impairments [11, 34–36]. However, an association between baseline self-management score and lesion level was not found. Davis et al. described a similar pattern wherein cognitive impairment, rather than lesion level, was associated with the age of acquisition of independent living skills [30]. While cognitive impairment may have a bigger impact on adaptive skill development than physical impairment, it should be noted that many AYASB may experience a decline in their motor ability during adolescence [37]. Thus, self-management programs for AYASB should evaluate how mobility impairments may impact self-management independence and consider equipment or regimen options that may help overcome these physical limitations.
Previous studies using data collected from the National Spina Bifida Patient Registry have found that private insurance was associated with bowel continence, CIC independence, and ambulation [38]. Additionally, Atchley et al. found that having Medicaid insurance predicted a lower likelihood of self-CIC [39]. In this study, insurance was not associated with AMIS II-SR/SB baseline score or score improvement. In a camp-based self-management intervention by Holbein et al., parents of participants from lower socioeconomic backgrounds also reported greater progress towards health-related goals following the intervention [40]. They theorized that AYASB with limited home and community resources to foster independence may particularly benefit from goal-setting self-management interventions. Similarly, in the transition program, a dedicated nurse educator/coordinator and social worker meet with AYASB and their families at each visit to provide education, motivation, psychosocial support, and care coordination to facilitate self-management achievement.
While the type of bladder regimen was not associated with baseline self-management scores, score improvement did depend on the patient’s baseline bladder regimen. Specifically, AYASB not on CIC management and those managed with urethral CIC improved in self-management scores, but those managed with channel CIC did not have significant score improvement. We theorize two possible explanations for the lack of improvement for those managed with channel CIC. First, there could be a ceiling effect in improved bladder self-management after their initial post-operative period. While, Strine et al. demonstrated that 68%of children with SB who underwent bladder reconstruction with placement of a catheterizable channel required less or no assistance one month post-operatively, there may be less potential for improvement independence over time [41]. Secondly, the group managed with channel CIC often have more mobility impairment which may impede improvements in self-management [42]. In contrast, finding the greatest improvement in those without CIC management may reflect less limitations in self-management advancement as they have less complicated care routines and may have less mobility impairment. The improvement seen in those managed with urethral CIC may demonstrate that they have more skill growth potential than the channel CIC group that can be fostered by self-management support. Castillo et al. similarly found that independence in SB-specific self-management tasks such as skin checks and non-SB tasks such as dressing and bathing independence correlated with bladder catheterization independence [43]. Thus, associating SB-specific care independence goals with the attainment of other skills for independence (e.g., home responsibilities, peer relationships, or preparing for employment and independent living) may be helpful when counseling AYASB and their families.
Associations with SB-related QOL
No variables were associated with baseline or change in QOL, which could be due to several factors. First, sample size was small, and baseline QOL scores were relatively high for both subscales. Previous studies have demonstrated health-related QOL scores in AYASB tend to be relatively high despite their having chronic conditions and functional impairments [16, 44]. Lennon et al. describe this phenomenon as a “resilience-disruption” view of family functioning, wherein the diagnosis of SB initially represents disruption to normal family functioning, but over time families of individuals with SB exhibit significant resilience [45]. Other studies also show that psychosocial factors such as family resilience, social support, hope for the future, and a positive attitude toward SB may contribute more to QOL perception than condition severity or impairments for children and adolescents with SB [44, 46]. However, several studies have demonstrated that adolescents with SB have higher QOL scores compared to young adults with SB [16, 47]. Emerging adult activities like transitioning from high school to employment or higher education, encountering housing and transportation barriers, navigating adult relationships, and worsening mental or physical health may precipitate QOL concerns that the younger population has not yet faced [14, 48]. Thus, further investigation is needed to understand the long-term QOL outcomes associated with independence as these AYASB emerge into adulthood.
Limitations
There are several limitations to this study. First, AMIS II-SB/SR and QUALAS-T surveys were completed by patients during their SB transition clinic appointments. Thus, surveys were not completed at consistent intervals or for a consistent duration as follow-up varied amongst the group. However, the random coefficient regression analysis used is designed for this situation where measurement intervals and duration are varied [49]. The small convenience sample may have limited significant findings due to models being underpowered. Additionally, there are numerous important variables that could impact self-management and independent living skills which were not evaluated due to the limited scope of this study including family functioning, adherence, and health literacy. Future studies should test these additional variables with a larger sample size. As surveys were entered via self-response, patient reporting accuracy can be questioned. Indeed, Psihogios et al. found that often adolescents with SB report higher levels of responsibility than their parents report [50]. Also, our self-management education and goal-setting intervention was part of our SB transition clinical care approach and lacked a formal research protocol. As such, the impact of patient goals on the AMIS-II SR/SB scores was not evaluated in this study. Given the lack of a formal research protocol and comparison group, we were not able to draw specific conclusions regarding the impact of this self-management support on self-management independence or QOL. Thus, further development of this goal-setting protocol and comparison studies are needed.
Finally, psychosocial factors contributing to self-management independence were not directly investigated. Several AYASB engaged in the program were asked about facilitators and barriers to initiating their goals during post-visit phone interviews. Commonly, AYASB reported external motivators in implementing their goals, such as coaching particularly, from their mother, phone alarms, visual prompts, as well as internal motivators such as desire to improve one’s health and prevent adverse outcomes such as hospitalizations. AYASB reported that the absence of coaching, prompting, school support and lack of internal motivation were barriers to implementing goals. These facilitators and barriers are helpful to consider when investigating difficulties with adherence and counseling on goals.
Conclusions
Self-management requires that individuals engage in routine health-related behaviors amidst their everyday lives. Thus, self-management development should be viewed as a dynamic process requiring frequent and on-going support from clinicians and families [2]. Understanding factors that may aid or delay independence for AYASB aids clinicians in tailoring interventions to the individual’s needs. This study suggests that age and bladder regimen type are significant indicators of self-management independence for AYASB. The institutional approach –to mitigate adverse social determinants –may have played a role prior to enrollment. Thus, race, ethnicity, and household language were not associated with scores at baseline or over time. This finding emphasizes that discussing family support needs and potential psychosocial barriers to self-management development is necessary to implementing patient centered goal-setting plans and fostering independence development. While QOL scores did not significantly change and significant associations with QOL scores were not found, there was a trend towards improvement for the QBB. Thus, the relationship between bowel and bladder care independence and QOL should be further evaluated with a larger sample size. Additional multicenter studies are needed to compare self-management interventions amongst AYASB who are ethnically diverse, have socioeconomic barriers, and have a wide range of physical and cognitive abilities.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflict of interest to report.