
Abstract
PURPOSE:
To compare scoring systems and their ability to capture short and long-term recovery of paediatric patients with acute encephalitis. To identify clinical predictors of short-term outcomes by correlating functional outcome measures at 1 month post diagnosis of acute encephalitis.
METHODS:
Patients with encephalitis diagnosed between July 2011 and 2016 based on Granerod’s criteria were studied in this retrospective cohort study. Functional outcome scores on WeeFIM, LOS, GOS-E, mRS and ICF at initial presentation and 1, 3, 6 and 12 months later were compared.
RESULTS:
WeeFIM and LOS scores both showed maximum change in the first 3 months, reflecting highest recovery in this period. With WeeFIM, the greatest change occurred within the first month following diagnosis. On univariate analysis, seizure frequency in the first month, presence of movement disorder, presence of autonomic dysfunction and lower baseline functional score was associated with poorer WeeFIM scores at 1 month. The latter three variables remained statistically significant on multivariate analysis.
CONCLUSION:
WeeFIM is a potentially preferred functional outcome assessment tool as it demonstrated greatest recovery within the first month due to a trend of high responsiveness and relatively low ceiling effect. Presence of autonomic dysfunction and movement disorders at diagnosis correlated with poorer outcome at 1 month post diagnosis.
What this paper adds: Comparison between the various scoring systems has not been performed in paediatric patients post encephalitis. WeeFIM is a useful functional outcome score in paediatric patients post encephalitis that shows the most change in recovery within the first month post event. Functional score at 1 month may help to predict short-term recovery up to 3 months post event. Presence of autonomic dysfunction and movement disorders predict poorer outcome.
Introduction
Acute encephalitis in the paediatric population is an uncommon but serious acute neurological emergency in children, with a global incidence of up to 12 per 100,000 people [1]. An audit at our centre reported 173 children treated for encephalitis and meningitis over a 4 year period (2008–2012), equivalent to an incidence of 21.3 per 100,000 person-years [2]. The reported percentages with minimal deficits or complete recovery range from 46%to 81%, with severe impairment from 2%to 28%, and with death from 4%to 25%[3–8]. One reason for the variability of outcome measures among the different studies would be the wide range of outcome measures used. Some studies used established outcome scoring systems such as modified Rankin Scale (mRS), Liverpool Outcome Score (LOS), and Glasgow outcome scale [1, 9–11]. Others used intelligence quotient or personality questionnaires, while some studies made use of clinical abnormalities such as persistent symptoms or abnormal neurological examination [12–14]. In addition, the time points for measurement of outcome differ between studies, and selection of these time points are largely arbitrary or timed at discharge from hospital or at follow-up without a defined time interval.
In adult studies, the Functional Independence Measure (FIM) scoring system was reportedly more reliable especially in adult patients post stroke and post traumatic brain injury [15–17]. The International Classification of Functioning, Disability and Health (ICF) has been reported to be similar to the FIM in the assessment of the activities of daily living and mobility of adults in the rehabilitation setting [18].
Functional independence measure for children (WeeFIM) had been used in previous studies that looked at improvement in functional outcomes post encephalitis. These studies reported that the improvement in functional scores across all domains were significant, with a mean duration of rehabilitation between 39 to 48 days [19, 20].
In terms of eventual outcome post encephalitis, most studies reported that few patients continue to improve in functional abilities post discharge and that most reach their permanent state by 12 months post discharge [1, 14]. It has been reported that factors such as baseline functional status and presence of movement disorder could affect functional outcome [1, 9]. Others have also reported factors such as admitting Glasgow Coma Scale (GCS), MRI and EEG changes, presence of cerebro-spinal fluid (CSF) pleocytosis, length of intensive care unit stay and time to initiation of immunomodulatory treatment to be significant in predicting functional outcome [1, 13]. In the paediatric population, younger age at onset, presence of seizures and number of treatments required for encephalitis were predictors of poorer functional outcomes [19].
There is currently no gold standard for measurement of functional outcome in children with acute encephalitis. An accurate measurement of functional outcome would enable researchers to identify clinical predictors of outcome to better prognosticate and guide intensity of therapy during early management. The aim of this study was to identify the scoring system with the greatest responsiveness for capturing short and long-term recovery of paediatric patients with acute encephalitis, with functional outcomes measured at 1, 3, 6 and 12 months. Responsiveness of the scoring system is the ability to detect change over time [21]. The secondary aim was to identify clinical predictors of short-term outcome by correlating functional outcome measures at 1 month post diagnosis of acute encephalitis.
Methods
Children aged 1–20 years who presented with acute encephalitis were recruited at a single institution providing acute care services (KK Women’s and Children’s Hospital, Singapore) from July 2011 to June 2017 (retrospective July 2011–November 2016, prospective January–June 2017). Ethical approval was obtained from the hospital’s institution review board. The inclusion criteria for encephalitis were based on Granerod’s criteria: encephalopathy lasting more than 24 hours with no alternative cause identified, with at least 2 of: documented fever > 38 degrees Celsius within 72 hours before or after presentation; seizures not attributable to pre-existing epilepsy; new onset focal neurologic findings; cerebrospinal fluid white cell count > 5/mm3; acute abnormality in brain parenchyma on neuroimaging and/or electroencephalography (EEG) abnormality that is consistent with encephalitis [22]. Patients with all forms of encephalitis (infectious or autoimmune causes) were included, whereas those with chronic encephalopathy of metabolic or epileptic causes were excluded.
Clinical variables of the patients such as age, gender, and presence of developmental delay were then collected. Presence of movement disorder, number of seizures in the first month, presence of status epilepticus, abnormal neurological examination, low Glasgow Coma Scale (GCS) < 8, presence of neurocutaneous stigmata, presence of autonomic dysfunction also were noted. Investigation findings of MRI and EEG changes, presence of CSF pleocytosis, total length of stay in intensive care unit, and time to various treatment modalities were also noted.
Next, five commonly used functional outcome measures in patients with neurological impairment or disability were selected, including i) Functional Independence Measure for Children (WeeFIM), ii) Glasgow Outcome Scoring –Extended (GOS-E), iii) modified Rankin scale (mRS), iv) abbreviated International Classification of Function for Children and Youth (ICF-CY) and v) the Liverpool Outcome Score (LOS). WeeFIM and ICF were designed for use in persons with disability in the rehabilitation setting [23, 24]. Components of WeeFIM included level of assistance required with transfers, activities of daily living, bladder and bowel control, need for mobility aids, ability to communicate and cognition [15]. ICF-CY categories included grade of difficulty in transferring oneself, maintaining a sitting position, amount of sleep, maintenance of sleep, agreeableness, tone of all muscles of body, involuntary contractions of muscles and presence of generalised pain [24, 25]. Modified Rankin scale was also designed for chronic disability, but most widely used for stroke. Its scoring is based on the level of disability with regards to activities of daily living [26]. GOS was designed for traumatic brain injury patients, with GOS-E being the paediatric version. Its categories include the level of disability with regards to degree of consciousness, independence at home or outside home, social activities, family and friendships and return to normal life [27]. The Liverpool Outcome Score (LOS) was developed as a simple tool to assess severity of disability in Asian children post Japanese encephalitis. It was determined to have high sensitivity and specificity in identifying children who were likely to be dependent based on a score of 2 to 5 for each category. Its categories included communication, feeding, independence, behavioural issues, school participation, presence of seizures, assistance with dressing, bladder and bowel control, along with motor control [10]. This score was also used to measure the level of dependence of children with other causes of encephalitis [9].
Functional outcomes were scored using 5 different scoring systems –WeeFIM, LOS, GOS-E, mRS and ICF –at initial presentation and 1, 3, 6 and 12 months later. As each of the 5 scoring systems makes use of different scales, the scores of WeeFIM, mRS, LOS and ICF were scaled to the 7 point scale of GOS-E to facilitate comparison. The scaled scores were calculated by scaling the scores to the range of 0 to 7, where the scaled score is the product of (raw score/maximum value for each scoring system) *7. Score changes are those between the score at two consecutive time points. Score changes per unit score from 0 months to 1, 3, 6, and 12 months were used as a measure of responsiveness. Ceiling effect was obtained by calculating the percentage of patients who had fully recovered (i.e., scaled score of 1) at each of the time points. The ceiling effect would be low when the majority of patients reached the highest possible score with little score change over time.
Age-adjusted WeeFIM scores using the Developmental Functional Quotients (DFQ) were then obtained. For GOS-E and mRS, scores were based on comparison with abilities of other similarly aged healthy children. For LOS, full score for the domain was given if the child would not have been expected to attain the developmental milestone based upon age, as per the instructions for LOS scoring. Patients were followed up until August 2017. Data from therapists’ entries and nursing charts were used to generate scores for each functional outcome measure, aided by scoring guides.
Statistical analysis
Non-parametric Kruskal-Wallis test was used for scaled scores and score changes. Scaled scores, score changes and extent of ceiling effect were compared against the scoring system with largest score changes - WeeFIM –using the Wilcoxon rank sum test for scaled scores and score changes and Fisher exact test for ceiling effect. Spearman rank correlation coefficients were obtained for pairwise comparison of raw scores to determine construct validity.
As the WeeFIM demonstrated greatest score change in the first month, the association between demographic and clinical variables at baseline and the WeeFIM score at 1 month using linear regression analysis were assessed. The clinical predictors that were statistically significant from univariate analysis were then used to perform multivariate linear regression. Statistical analysis was performed using SPSS v26.0 (SPSS Inc, Chicago, Illinois, USA).
Results
We recruited 29 participants in total at KK Women’s and Children’s Hospital, Singapore, 24 retrospectively and 5 prospectively from January to June 2017. Of the 29, 23 could be scored on all 5 scoring systems. Six were excluded from further analysis due to incomplete scores or being less than 3 years old.
Table 1 shows the baseline clinical characteristics of the study population. The mean age at presentation was 8.9 years (Range 3.1–15.0 years), with 10 males. At presentation, there was abnormal neurological examination in 62%and behavioural changes in 88%. Mean duration of onset of behavioural change was 4 days. Forty four percent of patients also developed movement disorders. Majority of the patients had seizures during the illness and only 33%did not have them. Mean length of ICU stay was 15 days, with the main indication for ICU being presence of refractory seizures requiring multiple anti-convulsants and airway support.
Baseline characteristics (Total N = 23)
Baseline characteristics (Total N = 23)
Only 16 (55%) patients had follow-up to 12 months. The rest were either lost to follow-up or had not reached the required time point for collection of data by the end of this study.
WeeFIM and LOS were similar to each other in showing greatest recovery in the first 3 months with much less recovery subsequently. GOS-E and mRS were similar in demonstrating improvement in functional scores in a stepwise pattern. ICF was least responsive in demonstrating changes in functional scores compared to the other 4 scoring systems (Fig. 1).
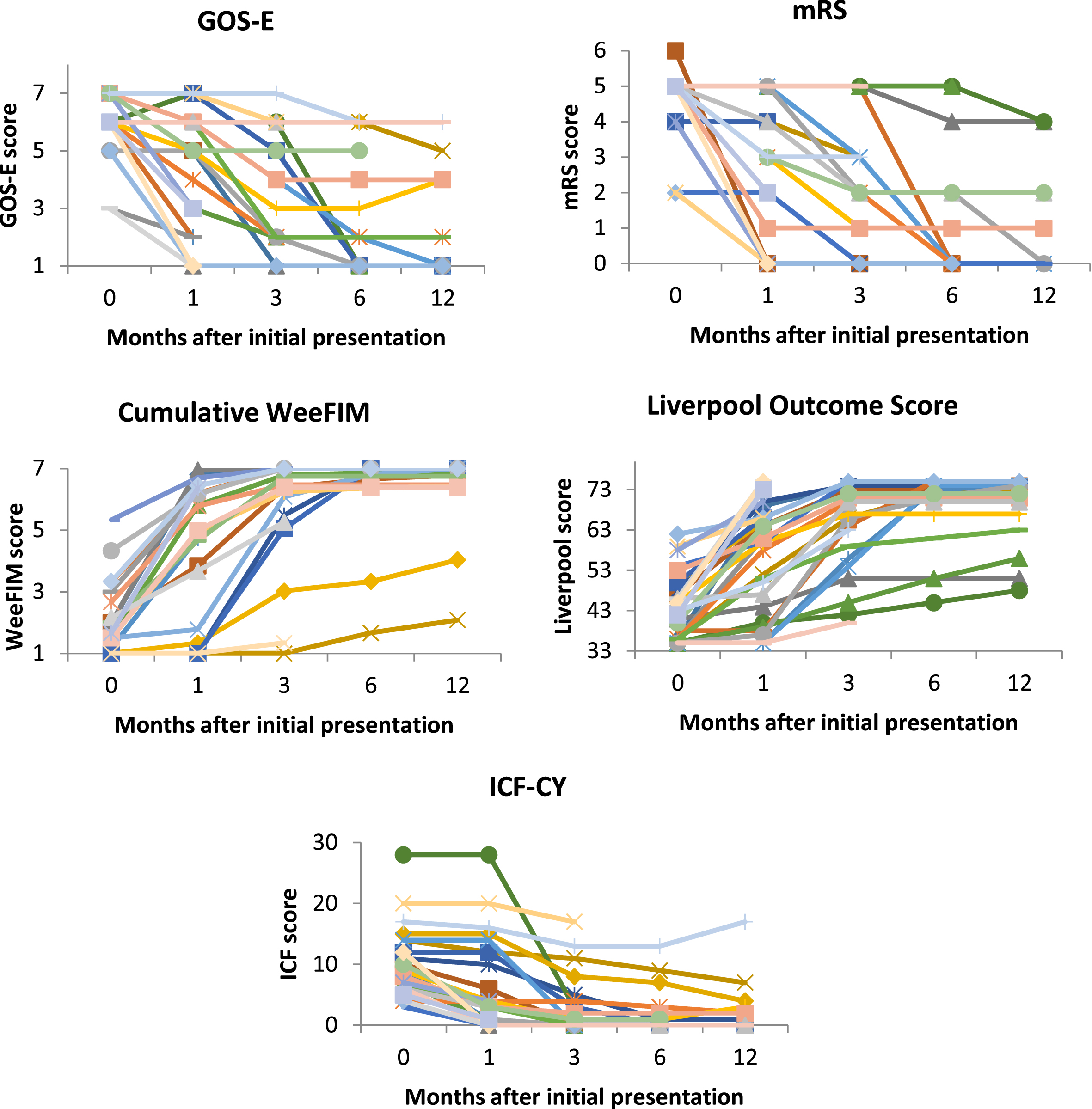
Changes in functional scores (raw scores) for each patient over time. Each line represents one patient over time at 0 months, 1, 3, 6 and 12 months after presentation; GOS-E (Glasgow Outcome Score –Extended) score range 1–8; mRS (Modified Rankin Scale) score range 0–6; Cumulative WeeFIM (Functional Independence Measure for Children) score range 1–7; Liverpool Outcome Score range 33–75; ICF-CY (International Classification of Function for Children and Youth) score range 0–30.
There is a high degree of correlation between the raw scores of all 5 scoring systems that is statistically significant (Table 2), despite the differences in scaled scores and score changes. The moderate and high correlations suggest substantially overlapped measurements of these 5 scoring systems.
Pairwise correlation coefficients between scoring systems
Pairwise correlation coefficients between scoring systems
Numbers in parentheses are the p values.
In this study, responsiveness is based on the ability to demonstrate the greatest score change at all time points. The mean change of scaled scores were compared for the 23 patients aged 3 years and above who could be scored on all 5 systems, WeeFIM had the highest responsiveness. LOS and ICF had the lowest responsiveness compared to WeeFIM at all-time points (p < 0.05). mRS had significantly lower responsiveness than WeeFIM at 3 month follow-up (Table 3).
Scaled scores at 0, 1, 3, 6 and 12 months, mean changes in scores from baseline of 0 months to 1, 3, 6, and 12 months and numbers of patients with score of 1 (i.e., fully recovered [R]) at 0, 1, 3, 6 and 12 months for each of the 5 scoring systems
Scaled scores at 0, 1, 3, 6 and 12 months, mean changes in scores from baseline of 0 months to 1, 3, 6, and 12 months and numbers of patients with score of 1 (i.e., fully recovered [R]) at 0, 1, 3, 6 and 12 months for each of the 5 scoring systems
p-values shown were derived from the test on mean change in scaled scores, computed using Kruskal-Wallace test; Fisher exact test for number of patients with full recovery. *indicates p < 0.050 for pairwise comparison of interval score changes between WeeFIM and other 4 scoring systems.
Looking at the subgroup of 16 patients with 12 months follow-up, the change in score from 0 to 1 month was smaller, suggesting that initial recovery may have been slower. The largest score change was demonstrated with WeeFIM in the first 3 months followed by smaller score change from 3 to 6 months. GOS-E and mRS had smaller but consistent score change at each time point from 0 to 6 months. As a result of this latency effect, there was greatest discrepancy between WeeFIM and GOS-E/mRS at 3 months, which was statistically significant (Table 3). GOS-E had a statistically significant lower responsiveness than WeeFIM at 3 months follow-up. Beyond 3 months, the scores of GOS-E/mRS caught up with that of WeeFIM (Fig. 2). LOS and ICF have the lowest score changes throughout the time course.
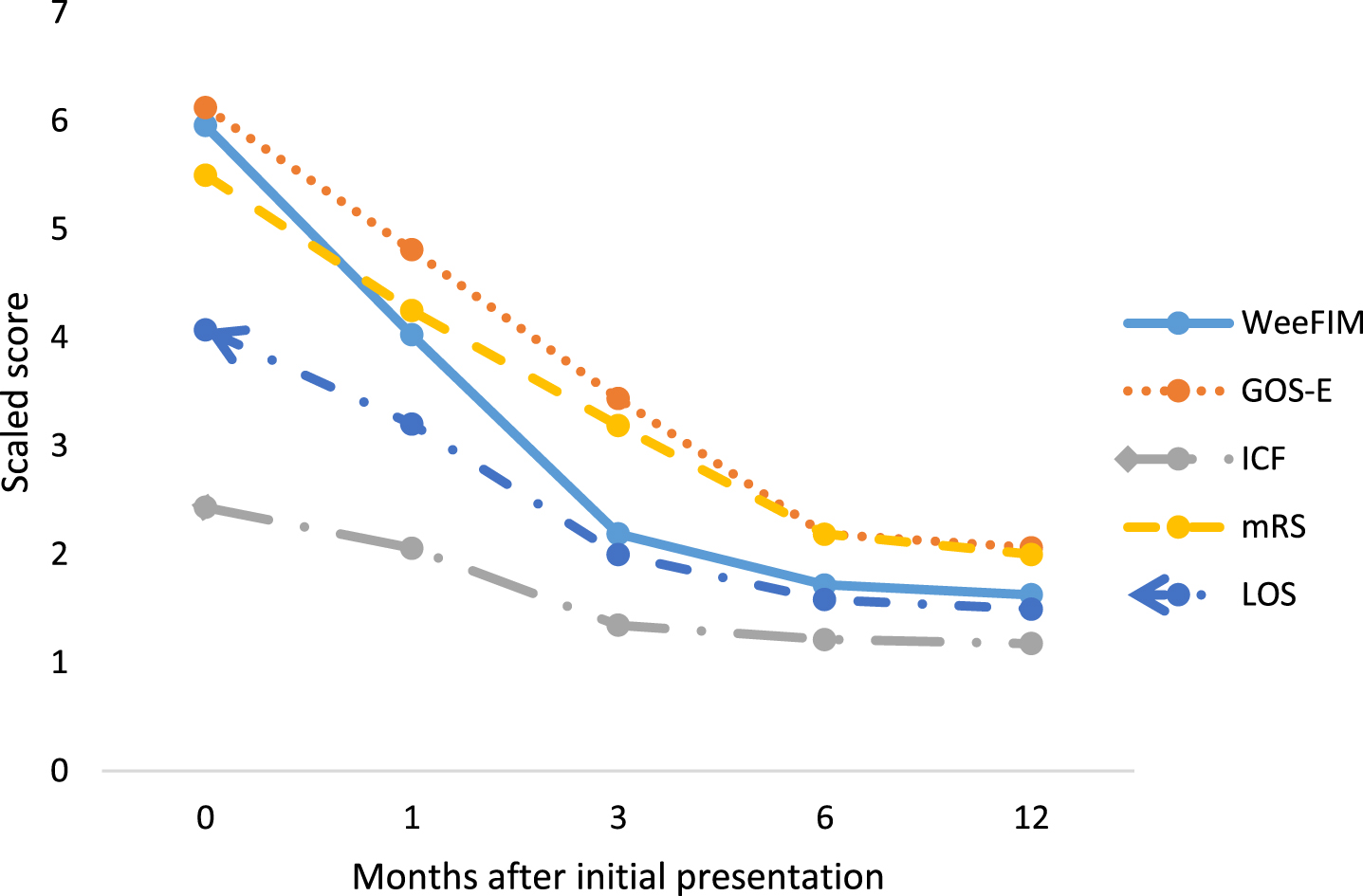
Mean scaled scores comparing 5 scoring systems at each follow up. Data available only for patients (N = 16) who completed 12 months follow up. Scaled score = (raw score/maximum value for each scoring system)*7.
In terms of ceiling effect, WeeFIM had lower ceiling effect than GOS-E and mRS at 1 month, but the difference was not statistically significant. At all the other time points, the extent of ceiling effect of WeeFIM, GOS-E and mRS were similar. At 3 months and beyond, LOS had the lowest ceiling effect and ICF had the highest (Table 3).
Since there was a trend of highest responsiveness and relatively low ceiling effect for WeeFIM (not statistically significant), it was used to identify overall trends in clinical improvement with time. From WeeFIM, the greatest recovery occurs between 0 and 1 month after diagnosis (Fig. 3).
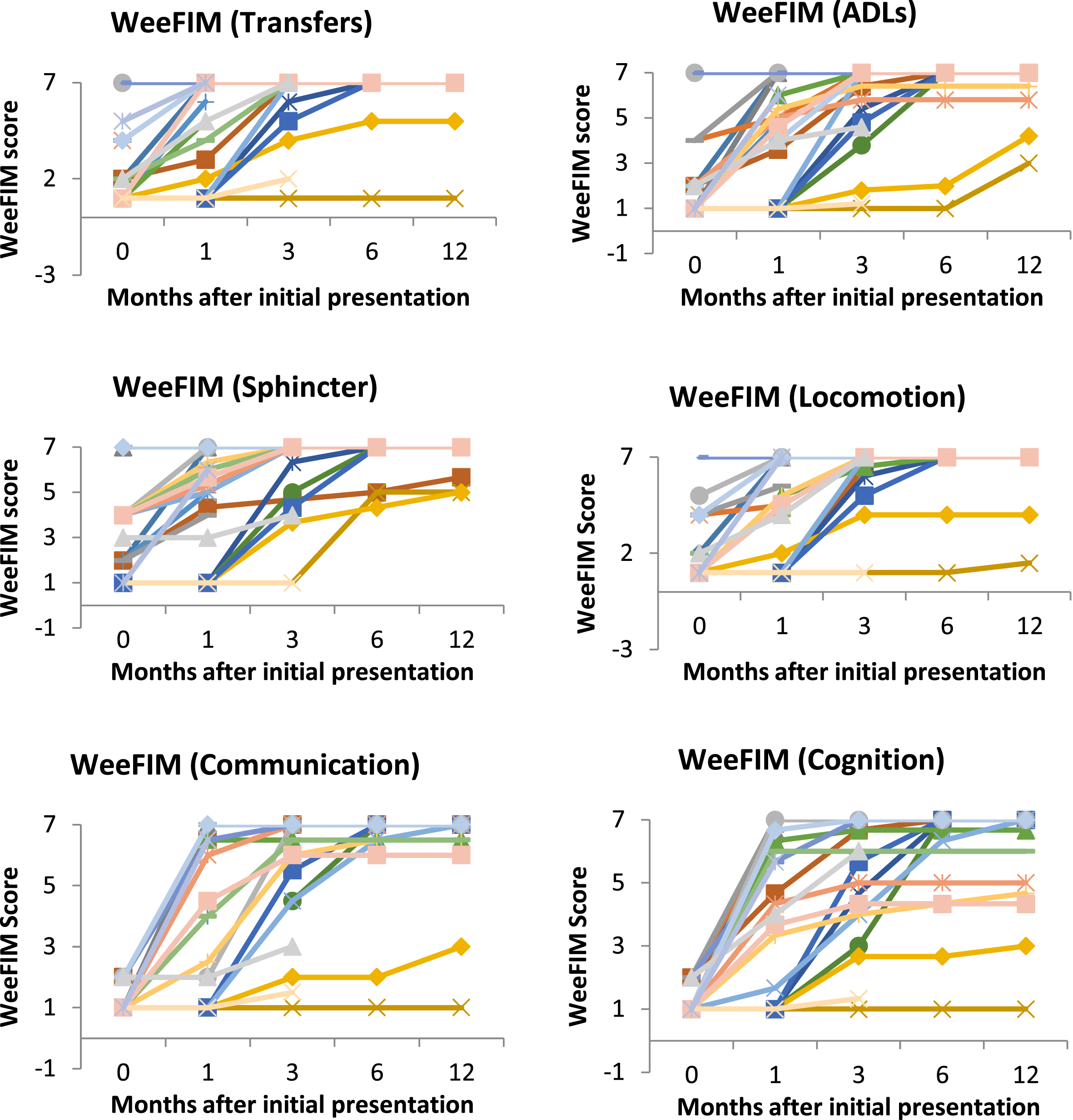
Change in raw scores over time for various WeeFIM domains. Each line represents one patient. A higher score indicates better functional status. Greatest recovery occurs in the first 3 months for all the domains. At the end of 12 months, the spread of scores is greatest in the cognitive domain.
Most patients would have reached their permanent state by 12 months post event, with the majority recovering completely (53.3%from WeeFIM) (Table 3). In addition, it can be seen from the various WeeFIM domains (Fig. 3) that the residual deficits at 12 months are mainly in the cognitive domain, which has the greatest spread from the normal score compared to the other WeeFIM domains.
The baseline WeeFIM score significantly correlated with subsequent WeeFIM scores at 1 and 3 months, with the highest correlation at 1 month (Table 4). Hence, it would be reliable to identify predictors at 1 month.
Correlation between WeeFIM score at baseline of 0 months and WeeFIM score at 1, 3, 6, and 12 months after diagnosis
Correlation between WeeFIM score at baseline of 0 months and WeeFIM score at 1, 3, 6, and 12 months after diagnosis
Four clinical variables significantly correlated with WeeFIM score at 1 month after diagnosis through univariate linear regression analysis. These were the presence of movement disorder, higher number of seizures in the first month, presence of autonomic dysfunction, and the baseline WeeFIM score at 0 months. With multivariate linear regression analysis, three of these variables –presence of movement disorder, autonomic dysfunction and baseline WeeFIM score –remained statistically significant (Table 5).
Univariate and multivariate linear regression analysis of clinical phenotypes in the first few weeks of initial presentation against WeeFIM score at 1 month
High responsiveness of WeeFIM was shown compared to other scoring systems in capturing recovery of children after acute encephalitis. This is in agreement with studies on adults post encephalitis [15–17]. It was reported that the responsiveness of GOS-E and mRS were similar from 0 to 6 months. This finding is also similar to another study showing that GOS correlates with and has no advantage above mRS [28].
In terms of ceiling effect, WeeFIM has less ceiling effect than GOS-E/mRS at 1 month, consistent with other studies on GOS. This may be related to GOS being less sensitive to subtle cognitive deficits which WeeFIM can measure [29].
In patients with complete follow-up to 12 months, WeeFIM and GOS-E/mRS scores at 3 months showed significant difference from baseline. This observed difference may be due to a latency effect of GOS-E and mRS compared to WeeFIM. WeeFIM measures individual domains, but small improvements in individual domains early in the clinical course may not be sufficient to impact level of independence, which was what GOS-E and mRS measure [30]. Another possible explanation was selection bias due to a loss of follow-up. This group of patients was more likely to be severely affected, had slower initial recovery and was therefore followed up for a longer period of time. This would contribute to greater deviation between scores and amplify the latency effect of GOS-E [30].
LOS floor effect and ICF ceiling effect make these scoring systems less useful as measures of function in encephalitis. LOS exhibited a floor effect with little range for change to be detected [29]. LOS was developed specifically for encephalitis and included domains such as seizure control, which does not impair functionality. Hence, low LOS scores may not equate to low function. ICF scores were low at baseline, reflecting good function. But ICF contains domains such as pain and sleep, which were not affected in the majority of patients, and caused a high ceiling effect.
Even though WeeFIM has been used in previous studies that looked at functional outcome post encephalitis in children, it does have several limitations which may affect its applicability [19, 20]. Unlike the other scoring systems, the WeeFIM tool required training and licensing. While they are a good measure of functional independence alone, GOS-E or mRS scores may be more useful in other situations in which independence and illness burden were both required to be assessed to determine caregiver burden or school placement needs.
Clinical course of recovery and predictors of functional outcome
Based on WeeFIM’s trajectory, the greatest recovery occurs between initial presentation and 1 month, coinciding with the average length of hospital stay, with little improvement post discharge. This would be in agreement with previously reported studies [1, 13]. The majority of patients reached their permanent state by 12 months, which was again consistent with the literature [8, 14]. Most patients recover either completely or with minimal deficits as with other studies on long term outcome [11, 31]. In addition, many were found to have residual cognitive impairment as gathered from the WeeFIM scores. This component was not measured in other outcome scores.
This study identified two new variables as clinical predictors of functional outcome: presence of autonomic dysfunction and movement disorders. Baseline functional status was also found to be a predictor but has been reported in other studies [1, 9]. Compared to prior studies, clinical parameters identified as outcome predictors in other studies (GCS, presence of MRI and EEG changes, CSF pleocytosis, length of ICU stay and time to initiation of immunomodulatory treatment) were not statistically significant in this univariate analysis [1, 13]. This is likely due to the broader aetiologies in the study compared to other studies. FIRES, ROHHAD, PRES, and cerebral vasculitis were included, all of which are proposed to have an autoimmune basis [32]. In summary, initial functional status predicts outcome only in the early clinical course up until 3 months as the WeeFIM scores correlated significantly at baseline and at 1 and 3 months post diagnosis. Subsequently the role of rehabilitation may be more important in determining permanent state.
Strengths and limitations
This study design limits the conclusions that can be drawn as it is largely retrospective in nature. Functional scoring was performed based on medical records of patients’ abilities.
This is the first study analyzing a wider range of scoring systems in encephalitis. It showed similar findings to other studies comparing fewer scoring systems. Prospective studies can draw on these findings in the design and execution of future work, such as comparing with other functional scales like the Paediatric Overall Performance Category and the Paediatric Cerebral Performance Category [33].
Neurological examination findings may change depending on who is examining and on which day the examinations were performed, making it harder to determine the presence or absence of certain clinical variables. However, the methodology is more consistent with a real-world setting and clinical practice. Therefore, the external validity was therefore high. Finally, the sample size was small, heterogeneous and not normally distributed. This was accounted for by using non-parametric statistical tests, which provided less statistical power to detect small score differences. Despite these limitations, it was still possible to detect statistically significant differences between the scoring systems.
Conclusion
This study reported that WeeFIM had high responsiveness, low ceiling effect, with individual domain analysis in children with encephalitis. These findings fit with key characteristics of a good measurement system.
WeeFIM is a useful functional outcome tool for patients with acute encephalitis at presentation and follow-up. The 1-month WeeFIM score may help prognosticate outcome in the first 3 months. Subsequently, rehabilitation may play a larger role in determining the permanent disability state. This information will then be useful in anticipatory guidance for parents, anticipation of potential complications after discharge to reduce readmission rates, and for planning for school placement, modification of home setup to facilitate ADLs, and application for additional home help if required.
Footnotes
Acknowledgments
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest
The authors have stated that they have no conflict of interest to report.