
Abstract
PURPOSE:
Adolescent idiopathic scoliosis (AIS) is associated with perturbation of orthostatic postural control. In humans, orthostatic postural control is organized around the gravitational vertical (GV). Perception of the GV involves a bottom-up process (central integration of multisensorial information) and a top-down process that uses cognitive mechanisms relying on body image. This study hypothesized that AIS would be associated with an erroneous central representation of verticality. The objective was to demonstrate an altered top-down process of sense of verticality in AIS.
METHODS:
This multicenter, single-blind, case-control study evaluated 63 adolescent girls with AIS divided into two groups (major AIS (n = 31) and minor AIS (n = 32)) and 30 matched non-scoliotic adolescents. Participants scored their perception of trunk appearance in an upright position using a pictographic scale. The outcome measure was the difference between perception score and real trunk deformity.
RESULTS:
Participants with major AIS presented with misperception of their trunk appearance in an upright position when compared with those with minor AIS or controls.
CONCLUSION:
Adolescents with major AIS underestimate their trunk deformity in an upright position. This suggests an altered representation of body image, affecting top-down control of sense of verticality.
Abbreviations
Adolescent Idiopathic Scoliosis
Gravitational Vertical
AIS with frontal Cobb angle < 32°
AIS with frontal Cobb angle≥32°
Body Mass Index
Introduction
Adolescent idiopathic scoliosis (AIS) is a three-dimensional deformity of the spine observed preferentially in adolescent girls aged 10–16 years [1]. This deformation leads to adverse impacts, in particular low self-esteem and disturbed body image [2]. The underlying cause of AIS is probably multifactorial, involving genetic predisposition [3]. Moreover, AIS is associated with neurosensory disturbances such as altered control of orthostatic posture [4].
In humans, orthostatic posture is organized around two main stable reference frames: the supporting surface upon which a person is standing and the Gravitational Vertical (GV) [5]. When the supporting surface fails to provide a constantly stable reference frame, e.g., during walking, a person uses GV perception for postural control [6]. Two processes intervene in GV perception: a bottom-up process involving mental integration of sensorial input, and a top-down process that builds internal models of verticality [7]. These internal models of verticality explain the influence of body posture on vertical perception [7]. The bottom-up process uses multimodal sensorial information coming from somatosensory, visual, and vestibular systems. Recent studies have shown that AIS is associated with poor GV perception [8–12]. All these studies exclusively evaluated the bottom-up process of the sense of verticality, using paradigms based on measurements of the Subjective Visual Vertical and the Subjective Postural Vertical [8–12]. But little is known about alterations in the top-down process of GV perception in AIS. The top-down process relies on cognitive mechanisms, requiring mental representation of body image, more precisely knowledge of body spatial orientation relative to the vertical [7]. However, Gallant et al. found that the primary cause of psychosocial difficulties in AIS is altered body image [13], thought to be part of a pathophysiological process that could cause AIS [14].
The current study explored the top-down process of the sense of verticality in AIS. The aim was to study how the adolescent’s body image is used to align the body vertically [7, 8]. In AIS, trunk deformity can be measured on X-rays taken in an upright position. So, the notion of body image in AIS could be addressed by measuring an adolescent’s perception of their trunk’s appearance in a standing position and comparing this perception with the real deformity [14]. The hypothesis was that patients with AIS, especially major AIS, would present a disturbance of the top-down process of vertical sense, which results in a poor perception of trunk deformity in an upright position. Considering this hypothesis, a study protocol was designed to evaluate the perception of trunk appearance in a standing position in three groups of adolescents: minor AIS; major AIS; and non-scoliotic control subjects. If the hypothesis was correct, a greater alteration of body image in AIS patients with major deformities would be expected.
Methods
Study design and participants
The inclusion period was from June 2016 through December 2016. Inclusion and exclusion criteria are summarized in Table 1. The AIS group, composed of 63 adolescent girls with right thoracic convexity, was divided into two groups (above and below the median thoracic angle on the whole spine X-ray taken in an upright position): AIS with frontal Cobb angle < 32° (AIS-min) and AIS with frontal Cobb angle≥32° (AIS-maj). The control group was composed of 32 non-scoliotic adolescent girls. The control group was comparable in gender, age, and BMI to the two other groups. The characteristic features of the study groups are presented in Table 2.
Inclusion and exclusion criteria
Inclusion and exclusion criteria
AIS: adolescent idiopathic scoliosis.
Baseline population
m: mean; AIS-min: adolescent idiopathic scoliosis with radiographic frontal Cobb’s angle < 32°; AIS-maj: adolescent idiopathic scoliosis with radiographic frontal Cobb’s angle≥32°; SD: standard deviation; BMI: body mass index; NS: non-significant.
The presence of a control group had two advantages: it allowed a comparison of the results with the AIS groups; it also ensured that the pictographic scale was clear and understandable by adolescents. Consent forms were presented with clear oral and written information and were signed by the participant and/or legal guardian(s). The study methodology and future anonymous use of data in the medical chart for research purposes was explained, as were patients’ rights as presented in the Helsinki Declaration. The authors’ regional institutional review board for the protection of people participating in medical research gave its approval for the study protocol (n°2015 A00950 49 - CPP 15 64). For the AIS-min and AIS-maj groups, no additional X-rays were needed for the purpose of this study. All X-rays used for this research were performed with the EOS® system to limit radiation exposure. For the control group, no invasive procedure (no X-ray) was required.
Objectives and evaluation criteria
To address the hypothesis, the primary objective was the assessment of mental representation of body image, specifically knowledge of body spatial orientation relative to the vertical. For this assessment, the primary endpoint was the measurement of the perception of trunk deformation in a standing position by a pictographic scale. A secondary objective was to evaluate whether adolescents with minor AIS have a different perception of trunk deformation than adolescents with major AIS. Therefore, the results of the pictographic scales were compared between the two groups.
Development of the pictographic scale
Different scales available for evaluating body image and trunk perception in AIS were assessed. Pictorial scales are more efficient than verbal scales [14–23], but none of those assessed were relevant to the specifications of the current research (Table 3). The study required a pictorial scale that was simple and quick to complete, with realistic pictures (easy for the participant to recognize), with at least a front and a back view, and with at least 5 items for each view. The whole body (head, trunk, lower limbs) needed to be represented in a vertical position and with radiographic correspondence (Cobb’s angle) for each item. Considering these criteria, a pictographic scale for self-evaluation of trunk appearance in the frontal plane in a standing position was developed. This self-evaluated appearance was compared with the real shape of the trunk in the two AIS groups. For the control group, the shape of the trunk was considered normal, i.e., without scoliosis. The pictographic scale used both the front and back view of the trunk. For AIS patients, the back view correlated with the follow-up X-rays they were familiar with, and the front view corresponded to the image they would see in a mirror. The pictographic scale consisted of five drawings of an adolescent girl with five stages of trunk deformation. These drawings were based on the frontal radiographic angle value of scoliosis (Cobb’s angle).
Pre-existing scales of subject’s self-image and subject’s trunk perception in AIS
Pre-existing scales of subject’s self-image and subject’s trunk perception in AIS
SRS-22 = Scoliosis Research Society–22; WRVAS = Walter Reed Visual Assessment Scale; SAQ = Spinal Appearance Questionnaire; TAPS = Trunk Appearance Perception Scale.
The illustrations also portrayed the asymmetry of the scapular and pelvic girdles. To make them as realistic as possible, the drawings were based on real front and back view photos of an adolescent girl without AIS who consulted for spinal pain (pictograph n° 1) and four adolescent girls with right thoracic convexity AIS with various Cobb’s angles (pictographs n° 2 to 5). These five patients and their legal guardians were informed orally and in writing of the possible use of their medical data for research. They signed a written consent form to approve the anonymous use of their image (e.g., photographs, X-rays) for research purposes. The data were used anonymously to protect these five patients as outlined in the Helsinki Declaration.
Participants were asked to perform the experimental task in the presence of an investigator but without the parent’s attendance. The investigator, who was blinded to the subject’s scoliosis status, presented the pictographic scale composed of two series of pictograms (Fig. 1). The explanation was always the same: “Please fill out this form, one line at a time, and in order. Each line corresponds to a view of your chest (a back view and then a front view). On each line, there are 5 drawings; you have to tick the one that looks the most like you”.
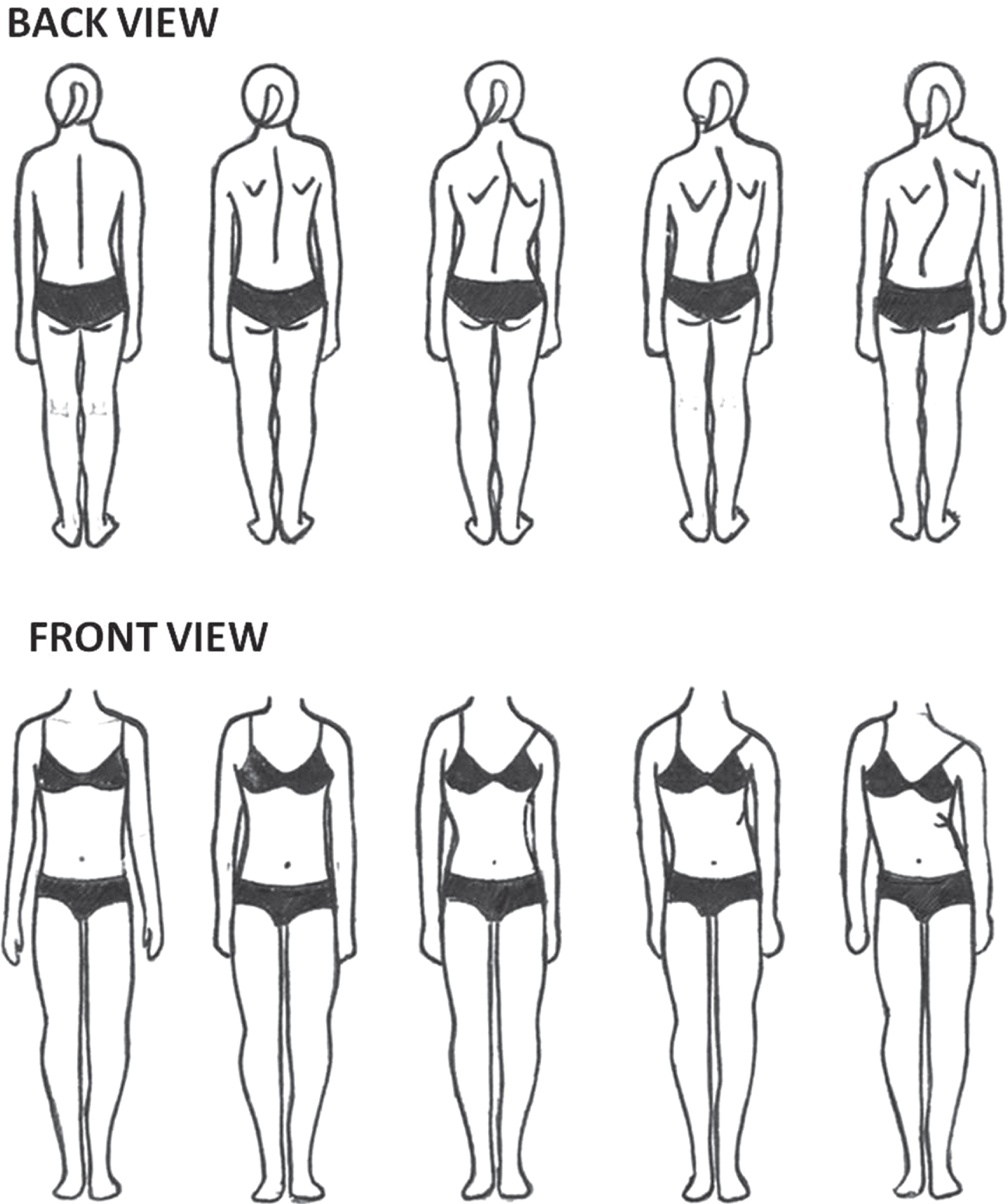
Pictographic scale for self-evaluation of trunk appearance in the frontal plane in a standing position.
The investigator did not provide any further information. A second investigator who was aware of the patient’s scoliosis status computed scores, defined as follows. Perception scores were defined for the back view (score a) and the front view (score b) as the pictogram number checked by the adolescent for the back view and front view respectively (possible score range 1–5). A real deformity score (score c) reflecting the Cobb’s angles corresponding to trunk deformations illustrated in the pictograms was determined for each participant by the second experienced investigator using a recent (less than 3 month old) whole spine X-ray in a standing position according to the following scale: Cobb’s angle < 10°= 1 (no scoliosis); 10–20°= 2 (minor scoliosis); 21–35°= 3 (moderate scoliosis); 36–50°= 4 (major scoliosis); > 50°= 5 (surgical scoliosis). This is the usual radiological distribution of AIS severity [24, 25].
The real deformity score was set at 1 for participants in the control group. The absolute difference between the perception score and the real deformity score was defined as the subject’s difference score, calculated for the back view (score d = a - c) and the front view (score e = b - c). Radio-clinical assessments were age, body mass index (BMI), age at the diagnosis of AIS, number of years wearing a brace, Cobb’s angle, and Risser radiographic test.
Data recorded included spinal tilt in the frontal plane assessed clinically with a plumb line from the spinous process of the 7th cervical vertebrae in relation to the inter-gluteal fold (mm) as well as gibbous deformity measured with a scoliometer (degrees).
The Shapiro-Wilks test was used to check normal data distribution. In this study, the values had a normal distribution. Likewise, the Bartlett test showed that the variances were homogeneous. This normality allowed for ANOVA analysis of the three groups. The search for correlations between pictorial scores and radio-clinical assessments was performed with Pearson’s coefficient. Differences were considered significant with a 5% alpha risk. The p-value was adjusted for the comparison of pictorial scores in the three groups. For that, the Bonferroni adjustment was used: α* =α/3 = 0.016. For the pictorial scores, the significant threshold was α* < 0.016.
Results
The three groups were not significantly different regarding age and BMI.
The perception scores a, b and c were between 1 and 5 (1 = no scoliosis, 5 = scoliosis > 50°) (Fig. 1). For scores d and e, the results were in absolute value, with possible range 0 –4, in which zero indicated perfect perception of real trunk appearance and higher scores indicated increasingly poor perception of trunk appearance (Fig. 2).
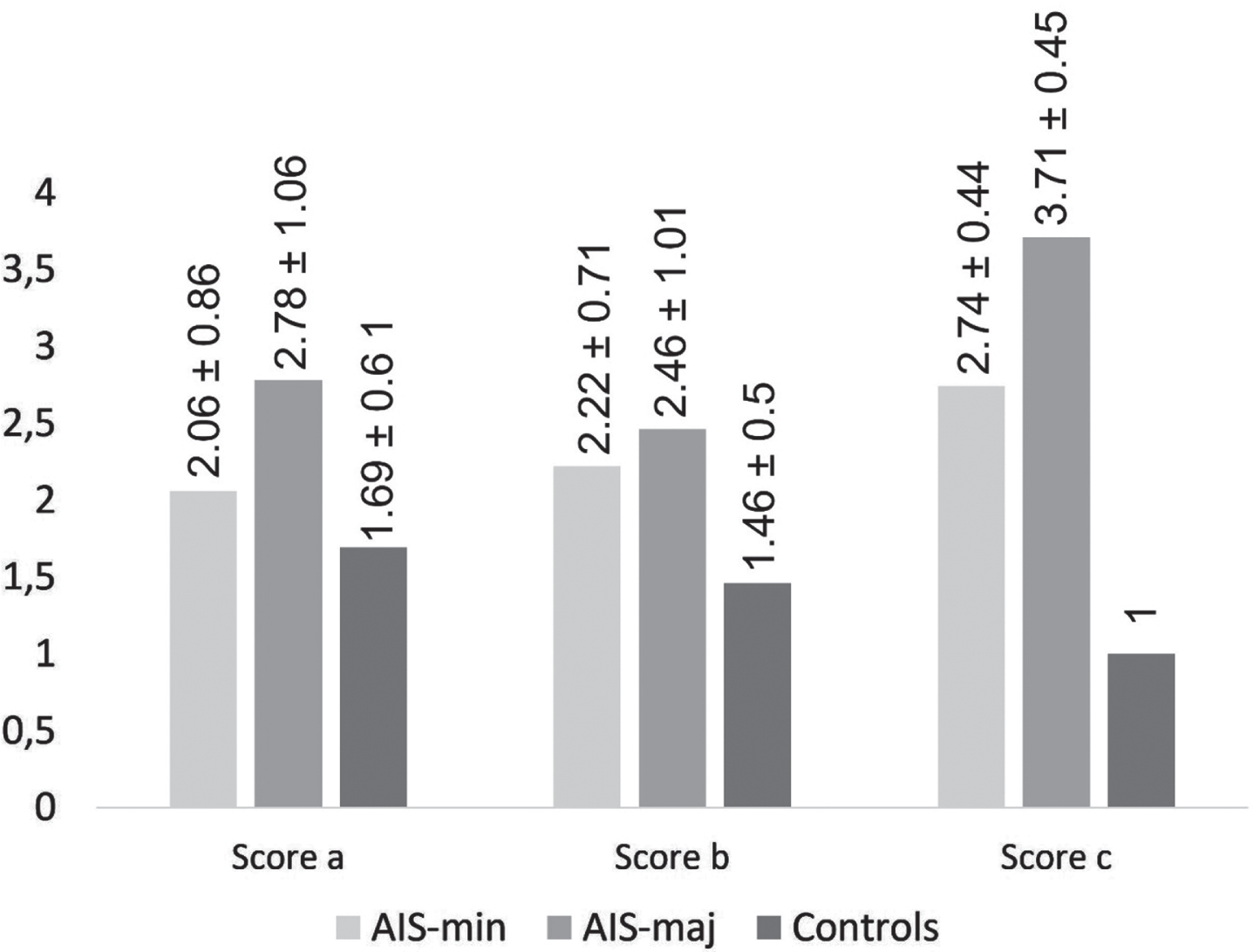
Scores a, b and c: results. AIS-min: adolescent idiopathic scoliosis with radiographic frontal Cobb’s angle < 32°; AIS-maj: adolescent idiopathic scoliosis with radiographic frontal Cobb’s angle≥32°; score a: perception scores for the back view; score b: perception scores for the front view; score c: real deformity score.
The difference scores were significantly different between the three groups. Participants in the AIS-maj group had a poorer perception of their trunk deformity than the two other groups (Fig. 3). This difference was most significant for the front view.
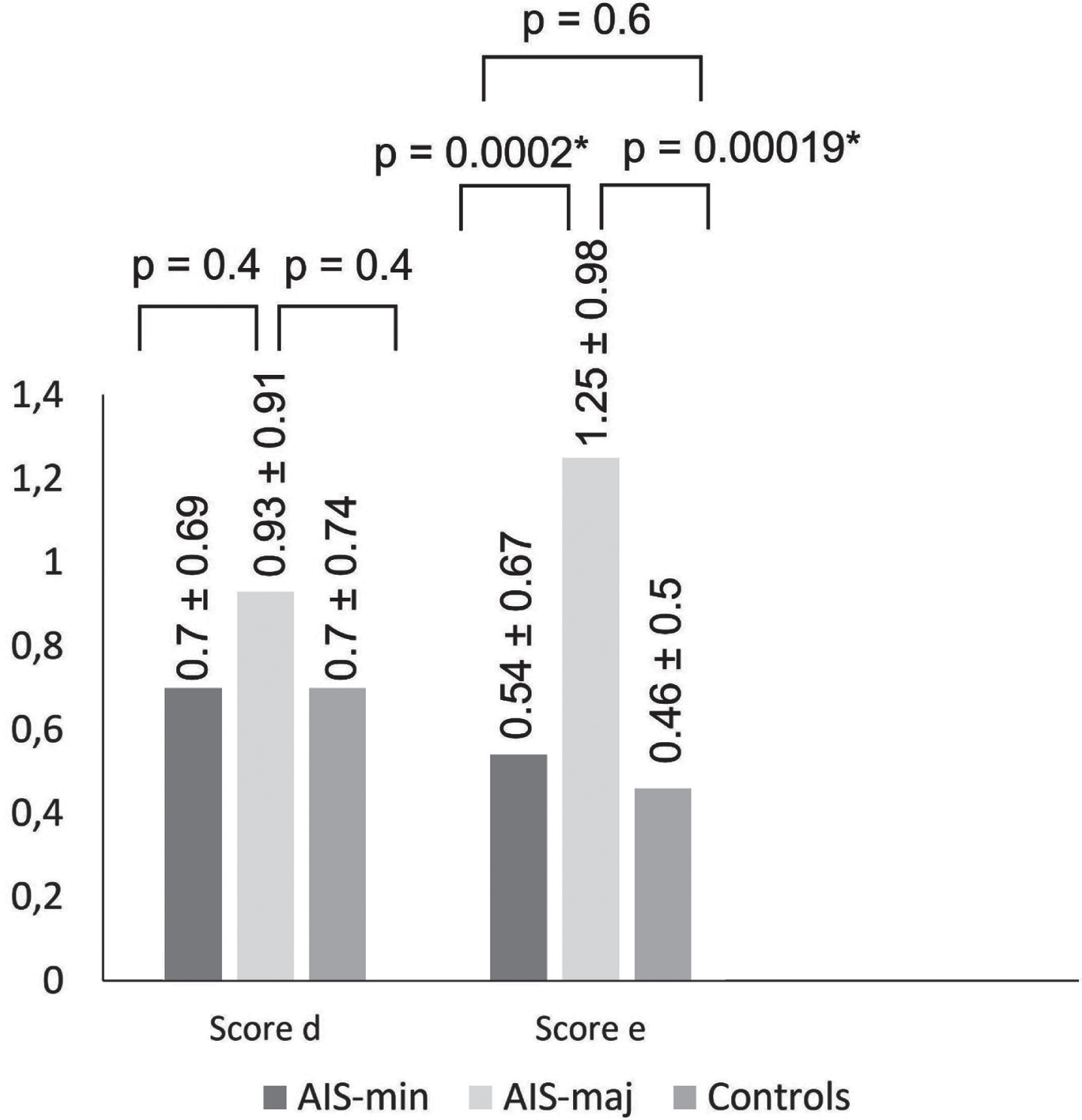
Scores d and e: results. AIS-min: adolescent idiopathic scoliosis with radiographic frontal Cobb’s angle < 32°; AIS-maj: adolescent idiopathic scoliosis with radiographic frontal Cobb’s angle≥32°; score d: difference score for the back view; score e: difference score for the front view.
In most cases, AIS patients who described an inaccurate perception of their trunk deformity underestimated their scoliosis, especially in the front view. In the AIS-min group, among the 14 participants who presented inaccurate perception of their trunk deformity, 12 underestimated their scoliosis. In the AIS-maj group (n = 32), all 29 patients (100%) who reported an inaccurate perception of their trunk deformity underestimated their scoliosis. Moreover, in the AIS-maj group, there was a difference between perception of the trunk deformity in the back view (more accurate perception) than in the front view (more inaccurate perception). No significant correlation between pictographic scale scores and radio-clinical assessments was found in the three groups.
The findings show that patients with major right thoracic AIS have a poor perception of their trunk deformity in a standing position. A disturbance of body image in major AIS can explain this misperception, especially the trunk shape in an upright position. The results are in line with recent hypotheses suggesting a body image anomaly in AIS [26] and prove that it can improved with adapted treatment [14, 27–30]. In 100% of patients with major AIS, the perception error was an underestimation of the degree of deformity. The difference was significant between the AIS-maj group and both the AIS-min group and the control group. This body image disturbance in major AIS can be interpreted as a consequence of scoliosis: the more severe the AIS, the more altered the perception of the trunk deformity. Prior studies have focused on the perception that surgical AIS patients have of their bodies after spinal fusion [20]. The aim of the questionnaires used for these studies was to assess the link between body image (i.e., perception of trunk appearance) and quality-of-life [21]. Therefore, pictographic scales that would be more relevant for evaluating body image and perception of trunk deformity were developed for the current study [15, 18]. Among the previous scales that inspired the 5-point pictographic scale, Piscelli et al.’s scale is the only one that brings together the adolescent’s self-perception of trunk appearance with the real scoliotic deformity [14]. Unlike in the current study, those authors found that AIS patients overestimated their deformity. It is noteworthy that Piscelli et al.’s scale only provided a back view [14], whereas the current study used both a front and a back view. Adolescents with major right thoracic AIS had a rather accurate perception of their trunk appearance when using the back view but underestimated the scoliotic deformity in the front view. In everyday life, there is no equivalent to the back view of one’s trunk. For scoliotic adolescents, familiarity with their own X-rays that provide a back view of the trunk probably gives them a reference. For the front view, the reference would be one’s reflection in a mirror. Apparently, the scoliotic patients in this study did not use their radiographic knowledge to evaluate their deformity in the front view. This study highlights several factors that could explain why adolescents with major right thoracic AIS underestimate their scoliotic deformity in the front view.
Neurocognitive factor
The neurocognitive mechanisms are different for visual analysis of the back view (i.e., the photographic reference) and the front view (i.e., the mirror reflection) [31]. In this study, a whole spine X-ray could be likened to a photograph. A recent neurofunctional study showed that the mechanisms of body image representation use different neuronal pathways depending on whether the adolescent observes a photograph of himself/herself or his/her reflection in a mirror [31]. Flagrant discordance between reality and expectations when looking in a mirror, called mirrored self-misidentification, has been described in anorexia [32]. The person can recognize himself/herself in a photograph, but the reflection he or she sees in the mirror is distorted. The same mechanism could be evoked in some AIS patients who experience discordance between the trunk deformity they recognize in the back view (X-ray) but not in the front view (mirror reflection).
Neurosensorial factor
Perception of the trunk appearance in an upright position is a constituent element of body image, which is a constantly updated internal representation of the body’s appearance [33]. People build their body image progressively from childhood by integrating changes affecting the body and environment [5]. Sensorial input is constantly providing the brain with a “snapshot” of the body image that is placed in memory [5, 34]. This updating mechanism could be defective in certain scoliotic patients because of alterations and/or poor use of multimodal sensorial information [8, 9]. This explains why body image cannot be dissociated from the shape, the position, and the body’s spatial actions [5, 34]. Moreover, body image is at the heart of the top-down process of controlling posture and the sense of verticality [7, 35]. A recent study suggested that the body reflected in a mirror is incorporated into an individual’s body image if the sensorial system operates correctly [36]. Visual and somatosensory inputs were long considered to dominate the construction of body image [37]. However, the predominant role of the vestibular system in updating body image is a more recent discovery [38–40]. Construction of body image involves central multimodal visuo-vestibulo-somato-sensorial interactions [38–41]. Abnormal processing of the visual and/or vestibular and/or somatosensory inputs could disturb body image updates, leading to a distorted perception of body shape [38, 41]. Most authors agree that AIS patients present altered processing of sensorial conflicts and sensory reweighting. [4, 42]. These arguments are in favor of a poor central integration of sensorial signals in AIS: visuo-spatial deficiencies, altered oculo-manual coordination, and learning disorders [43, 44]. In AIS, all these elements could change the body image seen in the mirror (front view) and modify body image updating [5, 34]. Thus, AIS patients may be aware of their deformity through information gathered from parents and medical staff without really perceiving it.
Neuropsychological factor
Loss of self-esteem is known to disrupt body image [45] and consequently the perception of the body’s appearance, in particular the trunk’s appearance in a mirror [25, 45]. Several theories argue that people with AIS experience a loss of self-esteem. Indeed, adolescence is a period involving great changes in body image [46]. For girls in the first part of adolescence, these physical transformations can induce potentially negative psychological impacts including lack of self-confidence and fear of what others will say. The psychiatrist Françoise Dolto compared the adolescent to a lobster who sheds its outer shell and must hide behind rocks at the bottom of the sea while waiting to find new effective defenses [46]. During adolescence, the child gets the impression that former perceptions, including body image, lose validity since change is ongoing and continuous [45]. Yet, throughout adolescence, a large part of self-esteem is conditioned by body satisfaction [47]. Moreover, self-esteem is weakened during adolescence and can also be degraded by AIS itself. The patient must accept the AIS diagnosis, which is said to be chronic but not perceived as such due to the lack of constant physical symptoms.
Moreover, success of the AIS treatment is not necessarily defined as an improved state of health but rather as a stabilization of the deformity [48]. The most difficult issue that adolescent girls with AIS face is an almost impossible projection into a “normal” future, with a disease evolving “behind their backs.” The overall effect of these different elements creates a psychic conflict which results in psychological vulnerability and an altered quality-of-life [49]. AIS studies have revealed higher prevalence of personality disorders, schizophrenia and anxiety-depressive syndromes [2], which are frequently associated with a distorted body image, and could thus explain poor perception of trunk deformity in the front view for AIS patients.
Affective factor
One’s body image reflected in the mirror is a representation of the “normal” human body in a straight, upright symmetrical configuration [50]. Since childhood, the body image seen in a mirror builds an expected representation that corresponds to an attractive image, but not necessarily to reality. The reflection in the mirror becomes an “idealized person,” rejecting defects and deformities such as trunk curvature [46, 50]. This mechanism reinforces the “distorted” reflection in the mirror and could be part of the explanation behind the discordance between the front view (idealized image) and the back view (imagined from X rays). Wearing a brace that keeps adolescents, physically and psychologically, attached to childhood reinforces the “distorted” reflection in the mirror [2]. The brace also complicates the acceptance of the physical transformations of adolescence and compromises the acquisition of a new equilibrium [2, 46].
Therapeutic intervention
The “distorted” reflection in the mirror can be improved with therapeutic intervention. Moreover, the use of a mirror is pertinent for many scoliosis rehabilitation methods (e.g., Schroth method, Lyon method) [51]. The current study showed that body image representation, especially trunk deformity in an upright position, is distorted in major AIS. Previously, interlinked neurosensory, neuropsychological, and affective factors were shown to be involved in altered body image. For AIS patients, this anomaly should be considered by multidisciplinary treatment focusing on therapeutic education, psychological acceptance of the disease and its treatments, and improved awareness of the deformity by multimodal sensorial stimulation [52].
Conclusion
This study confirms that major AIS is associated with the defective perception of trunk deformity about the GV. These findings are in favor of an altered top-down control of internal models of verticality. Prospective studies are needed to determine whether this distorted perception of trunk deformity could be an AIS prognostic factor and could explain poor therapeutic adherence. In light of these results, AIS rehabilitation should be multidisciplinary and begin with an awareness of trunk deformity.
Footnotes
Acknowledgments
This research is supported by funding from the “Fondation de l’Avenir pour la Recherche Médicale” (AP-RM-16-025) (http://www.fondationdelavenir.org) and from the “Fondation Cotrel de l’Institut de France” (Cotrel-10-2017) (![]() ).
).
The authors are grateful to the “La Maison de la Scoliose” (Villeneuve d’Ascq - France) and to the HARPS Association members (Seclin - France) for their helpful comments.
Conflict of interest
The authors have no conflict of interest to report.