
Abstract
PURPOSE:
To evaluate postural symmetry in sitting and standing for children with hemiplegic cerebral palsy (hCP) following the Combined Approach to Treatment for Children with Hemiplegia (CATCH) protocol, an intervention combining Constraint Induced Movement Therapy, Bimanual Intensive Therapy and Neuro-Developmental Treatment.
METHODS:
The study included 10 children with a diagnosis of hCP and 10 typically developing age-matched peers. Subjects participated in a CATCH camp for six hours daily for eight consecutive days. Postural symmetry measurements in quiet sitting and standing were obtained using a Boditrak pressure-mapping system at four time points: prior to start of camp (T1), first day of camp (T2), last day of camp (T3), and one month post-camp (T4).
RESULTS:
Significant differences (
CONCLUSIONS:
Children with hCP demonstrate improvement in postural symmetry in sitting and standing following participation in a CATCH camp. Following the intervention, children with hCP continued to improve postural symmetry and approach age-matched peers.
Introduction
Cerebral palsy (CP) is a non-progressive disorder of movement and posture caused by a lesion or abnormality of the immature brain occurring before, during, or soon after birth and resulting in activity/participation limitations [1, 2]. Prevalence in the US was previously estimated to be 3.1–3.6 per 1000 children [3, 4]. Cerebral palsy is a lifelong condition often resulting in the need for costly medical intervention. The lifetime medical cost of caring for a child with CP is $1,000,000, 12 times larger than those for a typically developing child [5]. Approximately 35% of children with CP are diagnosed with hemiplegia due to an asymmetrical brain injury [6].
Children diagnosed with hemiplegic cerebral palsy (hCP) present with more pronounced impairments on one side of the body that compromise functional use of upper and lower extremities [6, 7]. These children are typically independent ambulators and active participants in activities of daily living (ADLs) by two years of age [8, 9]. To accomplish functional tasks, children with hCP rely on compensatory strategies that contribute to asymmetrical postures and movements [10].
Postural asymmetry is a hallmark of children with a diagnosis of hCP. Children with hCP present with impaired postural control, exhibiting asymmetrical weight bearing distribution over the base of support (BOS) during static and dynamic activities [10, 11, 12]. These asymmetrical postures may contribute to compensatory strategies of upper and lower extremity function, gait, and participation in ADLs [13, 14].
Postural symmetry allows for an equal distribution of weight bearing over an active BOS in both sitting and standing [8, 11]. Symmetrical postural alignment is achieved very early in development as a child sits and transitions to stand during exploratory play in his or her environment [15]. Postural symmetry is dependent on adequate postural control, which is defined as the ability to control the body position in space to achieve orientation and stability. A child demonstrates postural control when they are able to sit or stand while maintaining center of body mass within the limits of the BOS during static or dynamic activities [10, 12, 15, 16].
A current intervention for hCP is Constraint Induced Movement Therapy (CIMT) which aims to overcome developmental disregard, a discrepancy between capacity and performance of the more impaired upper extremity (UE) [17, 18]. Expert consensus of CIMT identifies the use of a constraint on the less impaired UE as the critical ingredient in this intervention. Another key component of CIMT is intensive repetitive practice of age-appropriate motivating skills with the more impaired UE [19, 20]. Variables include type of constraint, duration, intensity, and environment. Clinical findings yield improved performance in unimanual capacity on the more impaired UE [20, 21].
Another approach to treating children with hCP is bimanual intensive training (BIT), which encourages the use of the more impaired UE in structured, bimanual, goal-directed play. Intense repetitive practice is a required element of BIT [22, 23]. Results of BIT demonstrate improvement in bimanual performance [21, 24, 25].
Neuro-developmental therapy (NDT) is a third approach to treating children with hCP. NDT is a clinical intervention that emphasizes posture and movement analysis specific to a child who has neuromuscular dysfunction. NDT is similar to CIMT and BIT in that it targets developmental disregard and impaired sensorimotor systems to improve function. In addition, NDT utilizes therapeutic handling to enhance postural and movement components that support functional task performance and skill acquisition [26]. These therapeutic handling strategies result in improved postural symmetry and control in children with hCP [27, 28].
Demographics
Demographics
xx
CIMT and BIT have been shown to be effective and complementary interventions to enhance functional outcomes for children with hCP [20, 29, 30, 31]. NDT has been a successful intervention used to impact postural symmetry and complement functional outcomes for children with hCP [26, 32, 33, 34]. The CATCH (Combined Approach to Treatment for Children with Hemiplegia) protocol combines key elements of CIMT, BIT, and NDT. The targeted outcome is reduction of asymmetrical postures and enhancement of UE/LE function for participation in daily life skills. The influence of postural symmetry on bilateral upper/lower extremity function is an area yet to be explored and documented in the literature.
The CATCH protocol is an eight-day program that uses play-based, goal directed activities to engage the more impaired UE/LE using principles of CIMT, BIT, and NDT. Supervised, trained volunteers implement the protocol. Building from the CIMT framework, on days one to five, the children wear a cast on the less impaired extremity and engage in repetitive, intensive practice of individualized functional tasks. On day five, BIT is introduced and in 50% of the camp activities, the children engage in individualized bimanual tasks. NDT-based clinical problem solving, task analysis, and therapeutic handling strategies are integrated throughout the program to promote postural symmetry. Prior to and during all activities, the interventionist uses NDT-specific hand placement and/or verbal cues to emphasize postural symmetry. On the last day of the protocol, children and their guardians are provided with an individualized home program and instructed in how to accomplish activities and exercises to facilitate maintenance of gained skills.
The CATCH protocol is designed to improve postural symmetry and enhance function and participation in activities. However, functional outcomes were not measured in this study, but are indicated for further research.
Pressure mapping is an outcome tool to evaluate posture and pressure in wheelchair seating and positioning [35, 36, 37]. Forces are measured using a sensor pad positioned between the client and wheelchair. Alternative applications for pressure mapping include evaluation of seating and standing postures of children with hCP [38]. Therefore, pressure mapping may prove to be a reliable and psychometrically valid tool to assess changes in postural symmetry in sitting and standing for children with hCP.
The purpose of this study was to explore the feasibility and effectiveness of the CATCH protocol to improve postural symmetry in children with hCP. This study also seeks to examine the feasibility of using pressure mapping as a clinical tool to assess postural symmetry.
Study design
This study utilizes a case series design with a convenience sample of children with hCP who attended a CATCH camp. Eleven typically developing (TD) children also participated in the study to serve as a comparison group. TD children were age-matched to a participant with hCP within six months of the participant’s age. Due to time constraints and availability, this group was tested twice within the same day to establish reliability of the measuring tool and to show symmetrical posture in TD children. The institutional review board of The University of North Carolina approved the study. Written, informed consent was obtained from participants’ guardians. In addition, assent was obtained from participants per institutional policy.
Participants
Eleven of the thirty-five children enrolled in the CATCH camp volunteered to participate in this study to serve as the intervention group. Descriptive information for each child is shown in Table 1. Inclusion criteria for participation were as follows: diagnosis of hCP, age between 3 and 10 years, ambulate without an assistive device, follow single step directions, and attend all eight days of camp. Participants in the study were recruited by an open invitation to guardians of children that met the inclusion criteria. Exclusion criteria were as follows: inability to grasp or participate in purposeful play or functional activity. Participant 2 could not complete all eight days of camp due to illness, so she was unable to complete the study. Therefore, her age-matched TD comparison was removed from the study.
Apparatus
The standard seat Boditrak pressure mat (Vista Medical)1
Boditrak Vista Medical Ltd, 3–55 Henlow Bay Winnipeg, Manitoba R3Y 1G4, Manitoba, Canada.
460 mm 16 Frequency of measurement: 100 Hz. 0–200 mmHg sensing range.
The children participated in a CATCH camp for eight consecutive days for six consecutive hours each day. The program had three primary components: (1) casting the child’s less impaired UE, (2) using CATCH principles to train volunteers to administer structured intervention, and (3) engaging the children in activities to improve strength, posture, motor skills, and functional use of the more impaired UE/LE.
At the initial assessment for each participant with hCP, an occupational therapist (HH) or occupational therapy student (AD) supervised by HH casted the child’s less impaired UE in a long arm (fingers to above elbow) removable fiberglass cast. The therapist, child, and guardian worked together to establish age appropriate camp goals/functional outcomes. During the first four days of intervention, the children wore their cast for five hours. From days five to eight, they participated in three hours of bimanual activities interspersed throughout the day. For further details on camp structure, please see the Appendix.
During the CATCH camp, children participated in individualized activities organized by the research team. ADLs and activities were focused on fine/gross motor skills, motor planning, balance, visual-motor skills, coordination, and sensorimotor integration. The camp’s daily schedule provided adequate practice opportunities based on the child’s individual functional goals. For further details on activities and intervention, please see the Appendix.
Trained volunteers consisting of undergraduate students, physical therapy (PT) students, and occupational therapy (OT) students administered the intervention. Prior to the start of camp, volunteers completed the training program in person or attended via video conference. The training included background information on hCP, developmental disregard, CIMT, BIT, NDT, and camp logistics. The research team that trained the volunteers consisted of a clinician (OTR/L) who trained through the University of Alabama at Birmingham (UAB) Constraint Induced (CI) Therapy Pediatric Training Program and a clinician (DPT, PCS) who is an NDTA Coordinator Pediatric Certified Instructor. Before the start of camp each day, volunteers attended a one-hour instructional lab to learn strategies to implement the CATCH protocol. Licensed occupational therapists and physical therapists supervised the volunteers.
Measurements of postural symmetry in quiet sitting and quiet standing were obtained using a Boditrak pressure-mapping system at four time points during the project: one month prior to the start of camp (T1), the first day of camp (T2), the last day of camp (T3), and one-month post-camp (T4). In this study, the term “quiet” refers to maintaining the same posture with weight remaining within the limits of the BOS. Socks, shoes, and orthotics were removed prior to measurement. Each child sat on the pressure map on a height adjustable bench with ankles, knees, and hips at 90
Data analysis
The quiet sitting center of pressure (COP) for each child was determined by first identifying bilateral ischial tuberosities (ITs). The ITs are known informally as the sit bones. In order to identify the ITs in our study, the total for each data point was averaged across 1000 frames to create a mean amount of pressure for each data point in the 16 by 16 matrix of the Boditrak sensor pad. Averages for the 256 data points identified were calculated. The prominent pressure points on the left and right sides of the body were confirmed as the ITs by these authors. If a child was sitting on their coccyx resulting in one prominent pressure point in the center of the overall weight distribution, the researcher identified the two notable points on both the left and right sides. The nine data points (total 18) surrounding each of the participants’ ITs were utilized for analysis of asymmetry in sitting.
Example sitting pressure mapping results. One time point during the 1000 frames for one participant. Data points relative to the IT, IT left (L) and IT right (R), represent the nine sensors surrounding the L and R IT.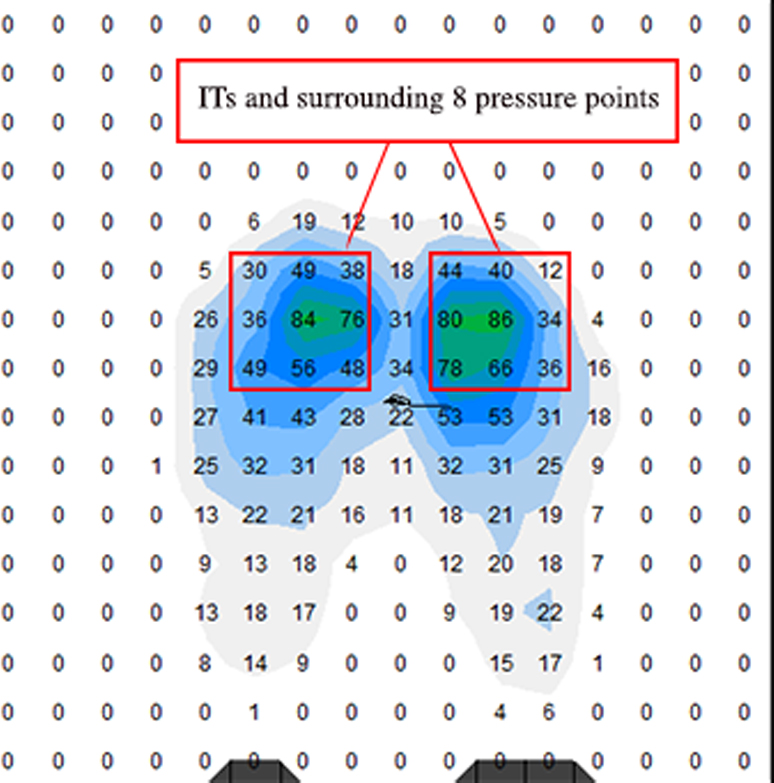
Example standing pressure mapping results. One time point during the 1000 frames for one participant. Data points relative to the IT, IT left (L) and IT right (R), represent the nine sensors surrounding the L and R IT.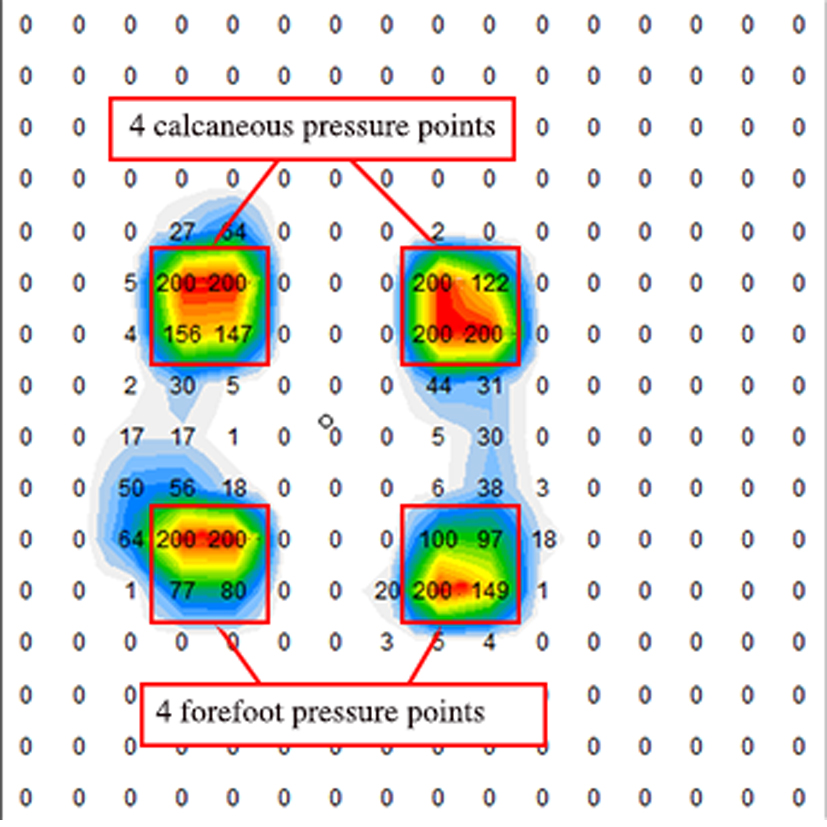
The weighted mean pressure was calculated using the following formula adapted from Fradet et al. [38]:
where the mirrored data points were compared across both left and right sides (Figs 1 and 2). The denominator is equal to the mean of the sum of all 18 points (nine from the left plus the nine from the right) squared. Once calculated for each of the nine data points, a resulting asymmetry figure is given.
Comparisons were made between the mirrored data points (sensor cells) to ensure accurate coordinate comparisons lateral to medial of bilateral LEs (Figs 1 and 2). Theoretically, the more symmetrical the posture, the closer the scores would approach zero (0). The more severe the asymmetrical posture, the greater the asymmetry number value.
The quiet standing data was analyzed using the same method. Each of the 256 data points were averaged creating a 16 by 16 matrix with an average of 1000 frames. The prominent pressure points on bilateral feet (heel and forefoot) were confirmed. Four data points were selected for each heel and forefoot. A total of 16 total data points were compared; eight on the left foot and eight on the right foot. Figure 2 is a representation of how asymmetry was calculated in standing.
Each parameter was compared across the four (T1–T4) time points using the Wilcoxon signed-rank test. The alpha was set to
Asymmetry posture standing measurements for participants TD and with CP
Asymmetry posture standing measurements for participants TD and with CP
T1
Asymmetry sitting posture measurements for participants TD and with CP
T1
Comparison of asymmetry measurements of sitting and standing postures in participants with CP over time
*
Comparing asymmetry postures of participants TD and CP over time
*significant at 0.05 level.
Baseline sitting measurements, T1 and T2, occurred prior to camp intervention (Table 2). There were no significant differences between T1 and T2. This indicated that symmetry remained stable prior to participation in the camp, and pressure mapping was a reliable tool. Non-significant differences were noted between T2 and T3. Significant differences were found between T2 and T4 (
Baseline standing measurements between T1 and T2 presented non-significant differences (Table 3). Non-significant differences were found between T3 and T4. Differences were approaching significance between T2 to T3 (
Symmetry calculations were also computed for the TD participants. These calculations revealed a relatively symmetrical posture based on age (Tables 2 and 3).
A Wilcoxon-signed rank test was performed to test for differences between the TD group and the participants with hCP.
Discussion
This study investigated whether the CATCH protocol resulted in improvement in postural symmetry in children with hCP. Postural asymmetry is expected to persist throughout the lifespan for a person with hCP [1]. However, the results showed that CATCH camp participants made positive changes in postural symmetry in both sitting and standing and these positive changes were maintained one month post-intervention. Posture was more symmetrical one-month post intervention with weight more equally distributed over the BOS. When comparing the pressure mapping results of children with hCP with their age-matched TD peers at one-month post intervention, there were no significant differences between the groups. This remarkable finding emphasizes the effectiveness of the CATCH protocol in improving postural symmetry in quiet sitting and quiet standing in children with hCP.
During quiet sitting, significant differences were not found when comparing children with hCP at baseline versus on the last day of camp. One explanation may be that children frequently sit during daily activities (school, eating, play, etc.). These routine periods of sitting result in more practice which may cause postural motor habits that are resistant to change. Our intervention may not result in immediate changes, but may have revised these motor habits. Children get opportunities to practice these new motor patterns over the course of the month after camp, resulting in significant differences between T2 and T4. Fatigue may also be one explanation for the non-significant difference between T2–T3 in sitting as the children have participated in a long intense week of a CATCH camp. Clinical observations documented during testing at T3 revealed that the children could not maintain the recommended testing position even with multiple verbal cues, but this was not the case at T1, T2, or T4.
A possible explanation for the significant difference between T3 and T4 would be that the children had additional interventions in the month after camp that further improved their postural symmetry. However, the most therapy that any participant received was eight hours spread over four weeks. Overall, most children had less than four hours of therapy (See Table 1). Recommended dosing for CIMT/BIT is at least 30 hours of therapy to see changes [16, 19, 20, 21, 39]. Therefore, the dosage of therapy received by participants after camp is likely not enough to elicit these changes. In addition, the children received the same frequency of therapy services between T1 and T2 and there was no significant difference between these timepoints.
Children often move in and out of standing, but experience difficulty stabilizing in quiet standing during daily activities. This postural instability along with muscle weakness is a primary impairment inherent in CP which impacts their daily activities [40, 41]. As upright skills occur later in life, the postural habits may not be as fully developed in quiet standing compared to those in sitting, making them more susceptible to change. This may explain why standing results are approaching significance when comparing T2 and T3, but are not significant in sitting.
One participant with hCP (CP8) did not show positive changes in postural symmetry, neither in sitting nor in standing. This camper presented with additional comorbid conditions, including seizures with abnormal EEG findings and ADHD. This participant was the only GMFCS Level II.
The growing research on neuroplasticity supports fine motor and gross motor improvement following CIMT and BIT intervention [29, 42, 43, 44]. Our results compliment these findings, suggesting that the CATCH protocol also improves postural symmetry at one month post-intervention in both quiet sitting and standing. The findings of our study identified positive changes in symmetry from T1–T4, which supports the occurrence of neuroplasticity, as children either continued to improve or maintained improvement in postural symmetry at one month post-intervention. These positive postural changes support the use of the CATCH protocol to improve postural symmetry, resulting in enhanced performance of functional tasks.
In contrast to other CIMT/BIT day camps, our intervention emphasized improving postural symmetry in conjunction with quality of UE/LE function [23, 25, 45]. Postural symmetry, a primary focus of our intervention, is correlated with improved UE/LE function making it easier to use the more impaired side of the body [13, 41]. Utilizing handling strategies based on the NDT clinical practice model, postural and UE/LE alignment were addressed prior to the initiation of and during any camp activity. The children were guided through play and age appropriate, functional ADL skills. In our CATCH protocol, play focused on increased use and awareness of the more impaired extremities to address developmental disregard, provide sensory information, and prepare the body for postural changes. Structured play transitioned from a unilateral activity (cast donned) to the same or similar bilateral activity (cast doffed).
Improvements in fine and gross motor skills after CIMT and BIT are well documented in the literature and therefore, were not chosen as a focus of this study. This study aimed to show positive changes in postural symmetry following the CATCH protocol. The limited research available has documented that improved postural symmetry positively impacts UE/LE function [10, 46]. However, further research is needed to explore the relationship between improved postural symmetry and UE/LE function for children with hCP.
With improved posture, there is potential to decrease and possibly prevent the development of secondary impairments such as contractures and scoliosis. UE and LE contractures are often noted in hCP early in development. Improved symmetry and increased use of the involved side may decrease or prevent the onset of contractures. Based on the research, children with hCP have a minimal increased risk for scoliosis that often leads to respiratory issues. However, increased symmetry may further decrease that risk [48, 49].
Pressure mapping was used successfully in our CATCH camp to evaluate postural symmetry/align- ment both in sitting and standing. This pressure mapping system can be easily used in a clinical setting with a variety of diagnoses. It provides a cost effective alternative to a force plate to evaluate postural symmetry, weight bearing, and center of pressure in sitting and standing. Data are easily downloaded and interpretable.
Limitations
The limitations of this study include: a small sample size, lack of randomization, and lack of a control group consisting of children with hCP that did not participate in the CATCH intervention. This study also lacks functional outcome measures that could determine ICF-function and participation improvements. Another limitation is the undetermined reliability with which the intervention was administered. There was not an established protocol for volunteer selection and no attempt was made to control for volunteer area of specialty, years of experience, etc. In this study, the researchers did not require hCP participants to record constraint wear or participation in traditional therapy and/or home exercise programs post-intervention, which could have affected the T4 results. Finally, there is limited normative data available for pressure mapping of typically developing children in sitting or standing [35, 38, 47].
Implication for future research
The investigators feel that the study should be replicated with a larger sample size in a controlled trial in order to generalize the findings. Data collection should include not only pressure mapping, but also a standardized measurement of UE/LE function to explore the relationship between improved postural symmetry and UE/LE function. Future research should also assess the fidelity of intervention delivery.
Conclusion
Children with hCP that participated in the CATCH camp intervention made significant positive changes toward postural symmetry in both sitting and standing postures. Post intervention children with hCP demonstrated similar postural symmetry when compared to their age-matched peers. Pressure mapping is a reliable and valid tool to evaluate postural symmetry for children with a diagnosis of hCP.
Footnotes
Acknowledgments
The authors would like to thank the families and their children who participated in the study while attending the CATCH camp. A special thank you is extended to all of the student volunteers who participated in the training and regularly attended the camp to work and play with the children.
Conflict of interest
The authors declare that there is no conflict of interest.
Appendix
The camp took place at an elementary school for six hours per day for eight consecutive days. There were 35 hCP camp participants, divided into six groups. For the first 30 minutes each day, before donning their cast, campers worked on activities of daily living, such as brushing their teeth, buttoning a shirt, or tying shoes. At the end of ADLs, all campers donned their cast with the help of their volunteer assistants. Throughout the day, the children followed a schedule and rotated through all activities in their groups. Participants ate snacks and lunch with the cast donned but were allowed to remove the cast for toileting. At the end of each day, casts were removed and stored at the camp.
Activities were organized by room. The themes in each room were gross motor, fine motor, sensory, computer, art, game room, and outdoor/water play. Examples of gross motor play included completing obstacle courses, riding bikes, and playing ball. Games that focused on fine motor skills included checkers, cutting Velcro food, and putting coins in a container. Sensory play consisted of looking for hidden objects in sand, (rice/beans), or noodles; playing with shaving cream or playdough; and playing games with ice. Computer play included a Wii, switch games, and remote-control toys. During arts and crafts, the children completed projects with bottle caps, paint, and sand art. Examples in the game room included board games, card games, pinball, and finger basketball. Outdoor/water play consisted of bubbles, fishing in a small pool, rockets and water shooters.
Some days there were specific activities led by a volunteer for all the campers to participate in as a large group. For example, there was a car wash where children had to fill buckets with water, soak sponges, and wash a car. Another example was making lemonade. The children had to pick out their lemon, roll it back and forth, pound it with a hammer, slice it, and then press the lemon.
There were several theme days including Western day, Sports day, and Pirate day. On these days, activities were organized based on the theme. During the camp week several “special guests” were present, including a Tae Kwon Do instructor, therapy dogs, and the local firefighters.
During the first four days of the intervention, the participants wore their cast for five hours per day. From days five to eight, the participants were engaged in three hours of bimanual activities in addition to three hours of cast wear. Play often moved from activities with cast donned to the same activity with cast doffed to allow for bilateral integration. For example, participants played with Velcro catch first with their cast on, practicing holding the self-stick paddle with the more impaired UE. Then the cast was removed and the participant played Velcro catch with two hands, holding the self-stick paddle with the more impaired UE.
During our camp structure, participants had the opportunity to engage in activities with ample practice of the more impaired UE/side of the body. Symmetrical posture was emphasized and facilitated beginning day one and continued for the entire eight days of camp. Before the initiation of any organized activity, the volunteers facilitated postural symmetry. The volunteers promoted symmetrical weight bearing and symmetrical posture during sitting and standing activities and adjusted table or chair height or provided foot boxes or stools to meet the needs of each camper. The volunteers set up games at midline and positioned themselves on the more impaired side of the participant to optimize facilitation. Volunteers would grade activities
as needed to tailor the intervention for the participant’s success and to maximize function. Volunteers also provided positive verbal feedback to reinforce appropriate alignment.