
Abstract
PURPOSE:
To perform a scoping review of the evidence for therapeutic interventions to manage functional impairments associated with Rett syndrome (RTT) throughout the lifespan.
METHODS:
MEDLINE, EMBASE, PsycINFO, CENTRAL, CINAHL, Scopus and Index to Chiropractic Literature were searched systematically up to December 2019. Two investigators independently reviewed all search results and extracted those that met the inclusion criteria. Human and animal model studies pertaining to therapies that increase functional ability or treat RTT-associated symptoms in all age groups were included. Relevant studies were grouped into intervention categories and rated using the Oxford Centre of Evidence Based Medicine Levels of Evidence. Demographics of participants, interventions, and outcomes were summarized.
RESULTS:
Ninety-one articles representing 88 studies met the inclusion criteria, of which 80 were human clinical studies and eight were studies using animal models. Study designs were primarily case series and only six studies involved participants above the age of 40.
CONCLUSION:
A small number of rigorously studied rehabilitation interventions have been published. Published studies aim to address a wide variety of functional impairments. Research regarding implementation of therapies for older patients with RTT is lacking and requires further exploration.
Introduction
Rett syndrome (RTT) is a complex neurodevelopmental condition that predominantly affects females and has an incidence of 1 in 8500 by the age of 15 [1]. Individuals with classical RTT may have typical development until six to 18 months of age, followed by onset of symptoms such as regression, seizures, bruxism, gastrointestinal dysmotility and vasomotor disturbances [2]. The diagnostic criteria for RTT has changed over the years. Currently, a clinical diagnosis of classical RTT is made when a child who experiences a period of regression followed by stabilization meets four essential criteria: partial or complete loss of acquired purposeful hand skills and spoken language, abnormal gait, and repetitive hand movements (wringing, clapping, mouthing, washing, etc.). Brain injury and psychomotor development during the first six months of life that is grossly abnormal are exclusion criteria [2]. Atypical RTT may be diagnosed if two of the four essential criteria, plus at least five of eleven supportive criteria, are present [5].
The causative gene for RTT was discovered to be MECP2 in 1999 [3]. MECP2 mutations are found in most, but not all, individuals with a clinical diagnosis of RTT [4]. Many different MECP2 mutations can cause RTT, but even individuals with the same mutation may vary with respect to clinical severity. The wide range of phenotypes displayed in RTT complicate the ability to study interventions rigorously, as the diverse spectrum of clinical severity must be considered when designing clinical trials.
Recently, systematic reviews in cerebral palsy and other neurodevelopmental disorders have been well received clinically and have allowed clinicians to understand the efficacy and quality of evidence associated with various rehabilitation interventions. Outcome measures are often derived from these major topics in rehabilitation research and allow for downstream clinical applications of research findings to lesser-known conditions with limited literature. However, unlike many other neurodevelopmental disorders, RTT symptoms are variable throughout the lifespan. This aspect often complicates the application of non-RTT research findings as specific therapies may be more effective at particular timepoints in the life of an individual with RTT. This suggests the need for increased RTT-specific research.
The assessment of functional outcomes in RTT is an emerging field. A recent systematic review into adaptive functioning in RTT concluded that this population has extremely impaired adaptive functioning skills. Additionally, current evaluation measures lack validity when assessing individuals with RTT [5]. Another recent systematic review into clinical tools for assessing gross motor, physical activity, and musculoskeletal impairments in individuals with RTT also concluded that research regarding functional evaluation tools for individuals with RTT is lacking [6]. These findings highlight some of the possible challenges faced when comparing RTT therapy intervention studies.
Research using animal genetic models has many benefits. Relevant to RTT, the use of animal models in research reduces between-subject phenotypic variation. As RTT is a relatively rare condition, animal studies are vital for identifying the potential outcomes of interventions prior to their translation towards human clinical research. Several RTT mouse models have been generated that accurately replicate RTT symptoms and have been used to demonstrate response to therapy [7, 8]. For example, one study found that increasing brain-derived neurotrophic factor improved motor impairments in RTT model mice [9]. This information ultimately led to the establishment of a clinical trial exploring a drug that increases brain-derived neurotrophic factor in humans [10].
In many ways, the gold-standard of clinical research evidence is the randomized-controlled trial. Accordingly, systematic reviews often include studies based largely, or only, on that study design. However, other study methodologies such as cohort studies, case reports, and case series are of particular value in the case of rare and heterogenous conditions [11]. Although these study types have limitations in external validity, reliability, and replicability, they provide valuable information for hypothesis generation and can often be applied towards clinical practice. The inclusion of case reports in the present scoping review is therefore appropriate given the clinical presentation of RTT.
Previous systematic reviews have been valuable in presenting available literature exploring therapies for individuals with RTT. A recent systematic review identified 22 articles providing evidence of non-pharmacological interventions for individuals with RTT [12]. Another recent systematic review studying developmental regression in RTT identified 12 articles demonstrating positive effects of behavioral interventions [13]. These previous systematic reviews have focused entirely on human clinical research and have excluded case studies and animal research, both of which provide valuable information with downstream translational potential to human clinical research. This review is more inclusive of such studies. Additionally, the current review aims to view the topic of therapies for RTT from a wider perspective and identify knowledge gaps in the field in order to inform future studies and clinical trials. As such, a scoping review methodology was adopted.
Many individuals with RTT live well into adulthood. A large cohort study found that 60% of individuals with RTT in North America were alive at age 50 [14]. The clinical features of RTT are variable as the individual ages, raising the need for dynamic therapeutic interventions that coincide with features as they come, go, and progress. A Dutch questionnaire study found that communication ability through verbalization or signs is demonstrated in one third of individuals with RTT and improves as the individual ages [15]. It has also been previously demonstrated that ambulation ability can be regained in adulthood [16, 17]. The aforementioned knowledge about lifespan and functional ability in RTT spurs the need for the implementation of intervention programs that support individuals with RTT throughout the lifespan.
The current scoping review aims to summarize and contrast all available evidence of therapeutic interventions targeted towards improving function conducted in both humans and animals. This scoping review discusses available evidence for interventions through a lifespan lens. This article aims to highlight future research areas, as well as to provide clinicians and researchers with a comprehensive summary of all available information regarding the themes and quality of the current literature.
Method
Items demonstrating the thorough conduct of this scoping review are specified in a Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist [18] (Appendix A). However, an a priori protocol was not registered or published for this scoping review.
Data sources
Interventions of interest were those aimed at increasing functional ability or treating a symptom associated with RTT.
All study designs were included. Study populations of females in all age groups with a primary diagnosis of RTT were included. Human studies involving males with RTT were excluded as males generally have a distinct phenotype from females with the same MECP2 mutations [23]. Studies that involved participants with a variety of conditions were included if RTT participant results could be distinguished. Studies utilizing RTT animal models of either sex were included if a therapy aimed to improve functional impairments or symptoms seen in human patients with RTT. Studies involving male mice were included as current male mice models more closely recapitulate the human female RTT phenotype [19]
Studies that included individuals diagnosed with RTT variants (“RTT-like” syndromes such as CDKL5 deficiency disorder or MECP2 duplication syndrome) were excluded. Epidemiological studies, natural history studies, basic science (cell) studies, textbooks or textbook chapters, opinion articles, and grey literature were excluded. Of note, interventions pertaining to pharmacology interventions, gene therapy, scoliosis, bone health, epilepsy, and perioperative management strategies were excluded, as these areas are extensive fields that warrant their own exhaustive review. Additionally, many of these excluded interventions already have been reviewed or have guidelines in the context of RTT. Cohort survey studies such as those focusing on natural history were excluded if treatment outcomes were not evaluated. Publications with non-English full-texts were excluded.
A search strategy was created by a medical librarian and one investigator (HLR, VG). Citations were obtained by systematically searching from the earliest date found to June 15, 2019 and then re-run on December 19, 2019. The search included the following databases: MEDLINE, EMBASE, PsycINFO, CENTRAL, CINAHL, Scopus and Index to Chiropractic Literature. Search terms used included the following subject headings plus keywords and synonyms derived from them: Rett Syndrome, Methyl-CpG-Binding Protein 2, Therapeutics, Physical Therapy Modalities, Exercise, Animal Assisted Therapy, Transcutaneous Electric Nerve Stimulation, Language Therapy, Deglutition, Respiratory Therapy, Hyperbaric Oxygenation, Complementary Therapies, Counseling, Self-Help Devices, Communication Aids for Disabled, Patient Positioning. The full search strategy is lengthy, please see Appendix B for the detailed OVID MEDLINE strategy. A manual search of reference lists from manuscripts was performed to identify additional literature not found by the original search strategy.
Study selection
Duplicates were removed. Two investigators (DY, VG) independently reviewed all titles and abstracts using Rayyan QRCI [20] to select articles for full-text review. Full-texts were reviewed using Covidence [21]. Conflicts were resolved upon discussion (DY, VG).
PRISMA flow diagram.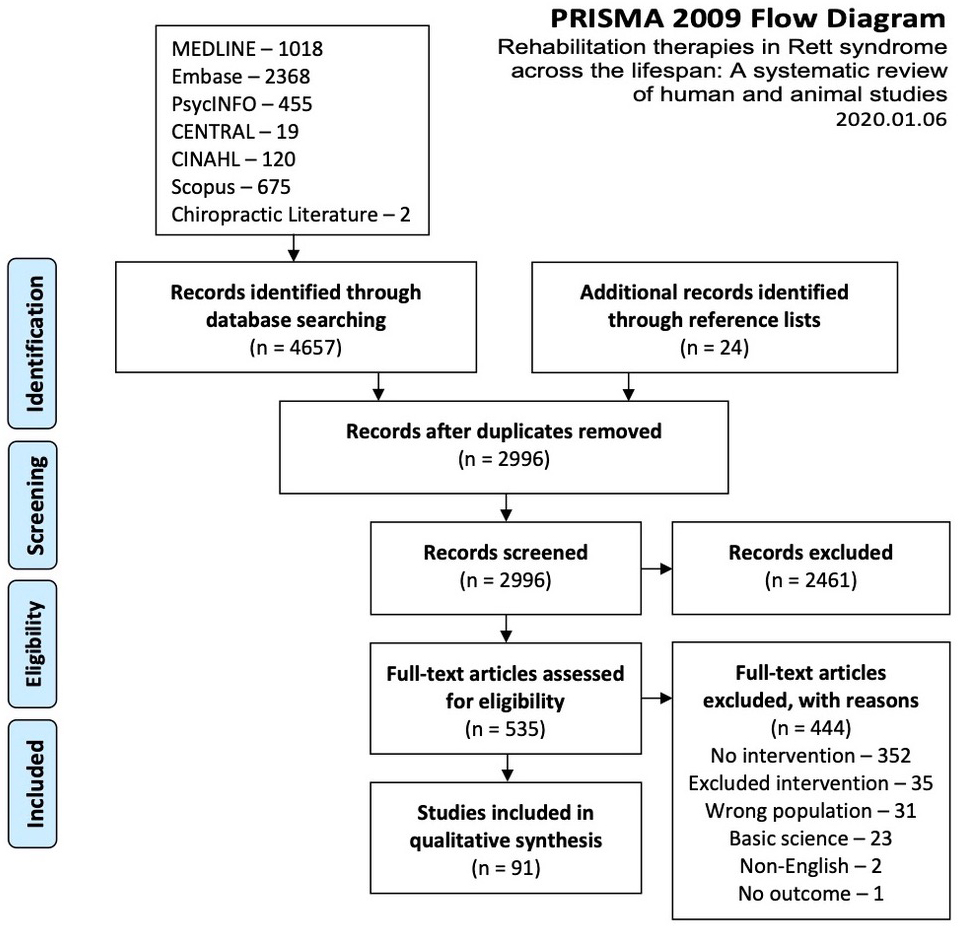
Relevant information from included studies was extracted. This included: study design, participant demographics and diagnosis details, intervention, and outcome. Age of animals can be extrapolated into approximately equivalent human phases of development based on growth and physiologic processes. However, the RTT animal models do not develop symptoms on the same time course as humans. Thus, the age of RTT animal models cannot be generalized to humans with RTT. As such, animal model ages were not extracted.
The Oxford Centre of Evidence Based Medicine Levels of Evidence 2 were utilized to assess the quality of study results [22].
Results
There were 4657 articles originally identified along with an additional 24 articles found by manually searching reference lists. There remained 2996 articles after removal of duplicates. Title and abstract screening identified 535 articles that met selection criteria. Of these, 444 articles were excluded during full-text screening as a result of six broad exclusion categories. Many did not study a therapeutic intervention (
In two instances, one study was published more than once [23, 24, 25, 26]. All articles are presented in the results (Tables 1–8), but papers describing the same study were counted once in summary tables (Table 9). As such, 88 studies were included.
The 80 human studies are categorized into the following broad study design categories: randomized controlled trials (
To optimize clarity in presentation of the findings, studies were grouped broadly by intervention type because some interventions targeted a variety of functional outcomes.
Of 80 human studies, 25 included participants over 18-years-old and only six included participants over 40-years-old. The remaining human studies focused entirely on children and adolescents. As many studies only reported a range of participant ages, it was impossible
Communication, cognition, and behavior interventions
Communication, cognition, and behavior interventions
Gross motor interventions
Fine motor interventions
Music therapy
Environmental enrichment
Brain stimulation
| Lead author and year Study location | Title | Study design (CEBM level of evidence) | Number of study participants with RTT Age Method of diagnosis | Intervention | Outcome |
|---|---|---|---|---|---|
| Bumin 2003 [91] Turkey | Hydrotherapy for Rett syndrome | Experimental case report (5) | 1 female Age: 11 years Diagnosis method not reported | Halliwick method hydrotherapy. | Decreased stereotypical movements, hyperactive behavior, and anxiety. Increased feeding activities, hand skills, balance, and interaction with environment. |
| Escobar-Torres 2019 [93] Spain | Efficacy of an aquatic exercise program for 3 cases of Rett syndrome | Experimental case series (4) | 3 females Age: 4, 6, 7 years Diagnosis method not reported | Individualized aquatic exercise. | Improved exercise heart rates, endurance during functional activities, mood, and others. |
| Lotan 2009 [92] Israel | Hydrotherapy for a young child with Rett syndrome. Review of the literature and a case study | Observational case report (5) | 1 female Age: Received water therapy age5–8 years Diagnosis method not reported | Structured hydrotherapy, as part of therapy program. | Improved communication with eye pointing, movement in water, land locomotion, and assisted stair walking. |
Other interventions
to determine the exact number of participants in each age group included in the cumulative total of 546 participants across all studies.
The studies fell under four subcategories: communication (
Of the 13 studies pertaining to communication therapies, one study coached or trained teachers or therapists, resulting in increased “bids” of communication by RTT participants [27]. Similarly, three articles from one single study investigated trained mother-daughter dyads to improve communication interactions during storybook reading [24, 25, 28]. Eleven studies trained participants to use various technologies to communicate needs or answer questions [29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39]. These interventions used various modes of communication such as touch screens, eye tracking, head- or hand-activated switches, or picture exchange systems.
The studies are also diverse with respect to intervention duration. For example, one study of 17 participants utilizing eye tracking allowed users to practice using the technology prior to assessment while other studies did not allow time for practice. The authors suggest this was the reason why subjects performed better than in previous studies [29].
An animal study found that RTT model rats benefited from intensive speech discrimination training in noisy environments and revealed improved ability to discriminate sounds to levels comparable to control rats with similar training [40].
Eight studies investigated cognitive therapies. Two case reports aimed to teach language skills. In one, the sounds and written appearances of five letters were successfully taught to a 14-year-old participant using a literacy curriculum [41]. In another case report, a participant was enrolled in a reading and writing program, as well as a cognitive rehabilitation program between age eight and 21. The individual learned to write sentences by 15 years of age [42]. The other studies implemented cognitive training programs, educational programs, computer games, contingency games, and other techniques to improve outcomes such as cognitive performance, attention span, symbol learning, writing sentences, and eye gaze [43, 44, 45, 46, 47, 48]. The studies in this subcategory generally showed some benefit over time. In one study, participants were unable to use eye gaze to answer questions about color, shape and position, but it is unknown if those subjects had the ability to answer those questions correctly in another way [39]. As such, this study may be better characterized as a knowledge assessment study, rather than an eye gaze intervention study.
Four observational and two experimental case series studied behavioral therapies. The interventions and outcomes were varied, and generalizability would be challenging. For example, one case reported that a reduction in demands on a six-year-old student improved pleasure and resulted in reduced stereotypic hand movements [49]. Alternatively, in a study of two subjects aged 14 and 23, physically interrupting hand wringing and hand mouthing resulted in reductions in the levels of these behaviors [50].
Gross motor therapies (Table 2)
The studies fell under two subcategories: ambulation (
Thirteen studies pertained to improving ambulation. Four investigated treadmill walking. A cohort study in 2004 demonstrated functional benefits of a two-month daily treadmill intervention [51]. Two subsequent cross-sectional studies showed that participants with RTT have benefits such as improved gait variability on a treadmill compared to over ground walking [52], and that within a certain range, increased treadmill speeds are able to increase participant gait speed [53]. A cohort study showed that treadmill walking normalized abnormal breathing in participants [54]. A relatively small number of participants with RTT were included in these treadmill studies, three of which were single event assessments. The 2004 cohort study of four participants remains the only long-term treadmill intervention study [51].
A group of case series and a cohort study described gross motor interventions, and how they improved or restored ambulation. Interventions include using a toy shopping cart prior to introducing a walker to a preschooler, using a microswitch-equipped walker to play a preferred stimuli (ex. a song or familiar voice), behavioral interventions, walkers, orthoses, and other individualized therapies [16, 17, 51, 55, 56, 57, 58, 59, 60].
The final study in the ambulation therapies category is a survey of physiotherapists, reporting on their patients with RTT. They described a negative correlation between foot position weight bearing and walking ability. This was assessed in conjunction with the role of orthopedic footwear, orthoses, and gross motor function [61].
The five studies in the multimodal therapies are diverse. This category is entirely comprised of case reports and series. They described multidisciplinary physical therapy, cognitive, and conductive education programs, among many others. They observed functional improvements in contractures, posture, sialorrhea, self-care skills, social skills, stereotypic hand movements, ataxia, and other positive outcomes [62, 63, 64, 65, 66].
Fine motor therapies (Table 3)
The studies fell under two subcategories: orthoses (
The seven orthotics studies examined heterogenous interventions resulting in diverse outcomes. Various orthoses were used such as: elbow splints, hand and thumb splints, and wrist cuffs of various designs. Outcomes studied included feeding ability with hands or utensils, switch use, environmental interaction, hand wringing, hand mouthing, and other stereotypic behavior. These studies reported positive outcomes, with the exception of two case series which found no improvement in stereotypic movements or independent feeding with the use of hand splints [67, 68].
Three studies, aimed to increase upper extremity-related independence or function without the use of orthoses, were grouped together. Two studies assessed therapy directed at increasing independent feeding. A study on independent eating using physical and verbal guidance in three individuals suggested that guided eating increased participation in the eating process and improved arm and mouth movements compared with caregiver feeding [69]. Similarly, a case series of five suggested that using hands-on instructions and verbal praise resulted in improved self-feeding skills and communication [70]. More recently, a 12-week virtual reality intervention was associated with improved reaching and reduced stereotypic movements in one participant [71].
Music therapy (Table 4)
Of the 10 studies, study designs included a cross-sectional study (
Music therapy was studied in groups of one to 23 patients. All studies described benefits to varying degrees. These included improvements in social interaction, communication, eye contact, hand function, mood, choice-making, vocalization, social play, turn-taking, and parent stress [72, 73, 74, 75, 76, 77, 78, 79].
Two studies used music therapy to increase patient engagement, enrich a physiotherapy session, or complete a gross motor assessment [23, 73].
As part of a survey done through the Swedish Rett Centre, 70 parents and caregivers outlined the functional benefits they believed were gained from music therapy. Almost all respondents described that participants responded positively to music by eliciting physical responses such as rocking, clapping, vocalizations, smiling [80].
Environmental enrichment (Table 5)
Of the five studies, the one human study was an observational case series. Other studies consisted of one randomized controlled and three non-randomized animal studies.
In a case series of three participants, a Snoezelen multisensory environment facilitated the successful implementation of a behavioral modification program. These environments provide immersive atmospheres through specialized equipment that target all senses through lights, textures, sounds, and other forms of sensory stimulation. Authors suggested that this was facilitated through relaxation and reduced agitation in a 63-year-old. A functional therapy and reaching program to reduce falls in a 58-year-old and a range of motion program to reduce contractures in a 24-year-old [81] were also facilitated with multisensory environments.
A randomized controlled trial had 12 preschool-aged participants participate in a sensory stimulation intervention for two to three hours, six days per week, for six months. During the intervention period, children participated in balance and walking activities, visual stimulation with toys and electronic devices, auditory stimulation, and taste stimulation. Improvements in gross motor skills were quantified using the Rett Syndrome Gross Motor Scale. Additionally, sleep and mood changes were studied using questionnaires, but were unaffected [82].
Four animal studies were included. These studies found that stimulating RTT model mice through environmental enrichment and physical activity had a range of benefits including anxiety reduction, improved motor coordination, spatial learning, and cognitive performance. These four studies used various RTT genetic models of both male and female sexes and compared standard housing to enriched housing. Enriched environments included a variety of toys or running wheels to encourage physical activity [83, 84]. Behavioral testing for anxiety, depression, and memory was done using previously established assessments such as elevated mazes, the Morris water maze, observations of mouse behavior in open areas, and food-seeking tasks. Locomotor activity was measured using sensors and motor learning was assessed with a rotarod performance test [83, 84, 85]. One study reported that the reduced response to fear conditioning by freezing seen in RTT model mice was improved by environmental enrichment [86]. However, these findings did not reach statistical significance. No negative effects of environmental enrichment were reported in these four animal studies.
Brain stimulation (Table 6)
Of the four studies, study designs included a randomized controlled trial and an experimental case series, in addition to one non-randomized and one randomized controlled animal study.
Transcranial direct current stimulation (tDCS) together with linguistic training improved language abilities and motor coordination in three participants with RTT [87]. tDCS in another study of seven subjects (seven treatment, seven placebo) showed similar results [88].
Female MECP2
Hydrotherapy (Table 8)
Of the three studies, study designs included an experimental case series, an experimental case report, and an observational case report.
Two case studies examined the effectiveness of hydrotherapy programs of different lengths in two participants aged five and 11 years, on a wide range of symptoms. The authors describe improved anxiety, hand skills, communication with pointing, and stair walking in both participants, among others [91, 92]. A case series of three participants aged four, six, and seven years who received a 20-month individualized aquatic exercise intervention underwent baseline and follow up assessments in physiological, functional and psychosocial domains. Improvements were assessed quantitatively or qualitatively, and included reduced resting heart rate, increased joint mobility, improved peer relationships, and improvements in the Functional Independence measure (FIM) [93].
Other therapies (Table 8)
Included studies not pertaining to the aforementioned categories are as follows: breathing therapies, vision therapy, therapy for aerophagia, sleep, dental and chiropractic intervention.
A cross sectional study and an observational case report studied breathing therapies. Two participants who underwent polysomnography to assess sleep disordered breathing demonstrated that severe central apneas resolved from the implementation of noninvasive ventilation or nocturnal oxygen therapy [94]. Long apneas and prominent Valsalva maneuvers were reduced in a 25-year-old patient with the introduction of continuous positive airway pressure (CPAP) [95].
A cross sectional study and an observational case report studied aerophagia therapies. The placement of a gastrostomy tube in a 13-year-old helped with severe abdominal distension [96]. A study on air-swallowing reported various beneficial therapies including: gum shields, specialized pacifiers, palatal training devices, and manual placement of fingers between the child’s teeth. The exact number of patients receiving these interventions was not reported [97].
Included study summary
Included study summary
A cross sectional study and a case-control animal study explored vision therapy. One study pertained to vision function. In the cross-sectional study, 11 participants underwent an ocular and vision assessment, and an unspecified number received glasses [98]. Authors describe participants and caregivers as enthusiastic about the benefits of the glasses. An animal study on MECP2 knockout mice used an optomotor functional task to assess vision and used visual evoked potentials along with other tests localizing the functional deficit to a visual pathway rather than motor pathway. The RTT model mice showed decline in vision after about four weeks of age. However, mice who were raised in the dark from birth or eye-opening showed visual acuity comparable to wild-type animals [99].
An experimental case series aiming to improve sleep in three patients with RTT was included. Baseline data was collected, which helped establish initial sleep and wake times. Various behavioral techniques were used such as a “fading procedure” to gradually advance bedtimes based on sleep latency the night before, reducing non-scheduled daytime sleep, and removing individuals from bed if they were not sleeping. This resulted in more regular sleep patterns and increased nighttime sleep [100].
One cross-sectional study regarding dental therapies was included. Observations of a group of 13 patients with RTT suggested the effectiveness of bruxism treatments including modified biteplates for daytime use and acupuncture [101].
One observational case report on chiropractic treatment was included. It described a 13-year-old patient who received several treatment modalities from a chiropractor over one year [102]. Numerous benefits were reported. Causality cannot be attributed.
This is the most comprehensive published review of therapeutic interventions for individuals with RTT to date. It is also the first review of RTT therapies to include clinical studies, animal model studies, and case studies, recognizing the value that these study designs play in this rare and heterogenous disorder. Previous reviews have omitted such publications despite the potentially meaningful information that they provide.
There is a clear lack of high-quality literature regarding outcomes of therapeutic interventions for individuals with RTT. The majority of identified studies were lower-quality study designs according to the Oxford Centre of Evidence-based Medicine Levels of Evidence with all but 17 studies belonging to the two lowest-quality levels [22]. The number of participants were usually small, control groups were lacking, and investigators were not blinded.
Communication, behavior, and cognition interventions were most often studied in humans while environmental enrichment was most often studied in animal RTT models. Several interventions indicated positive outcomes. Cognitive and behavioral therapies improved cognitive performance, increased attention skills, and reduced stereotypic movements. The majority of studies examining arm and hand orthoses and upper-extremity independence programs found numerous improvements in stereotypic movements, feeding, and communication, among other positive outcomes. Improvements in social skills, communication, and mood were observed in all studies pertaining to music therapy. Despite the low-quality study designs of the mentioned studies, this information provides vital information for the development of future studies and clinical implementation.
Older individuals with RTT were seldom included in the identified studies, indicating a clear lack of data pertaining to this age group. As individuals with RTT often live to an advanced age and are able to regain functional ability such as ambulation following therapy or use of assistive devices, this deficiency of research in adults is concerning. The natural history of RTT is becoming better understood, but given lack of knowledge, it is unclear whether the interventions under study are similarly effective across the lifespan. Additionally, it has been demonstrated that health service use decreases as the individual with RTT ages [103]. This suggests that older individuals with RTT are relatively medically stable and are in a position to benefit from gait, communication, or other therapy interventions. As such, increased research efforts must be directed towards therapies for older individuals with RTT. The current review found preliminary evidence of positive outcomes using Snoezelen environments in older individuals with RTT, suggesting the potential for future use of this intervention in this age range.
Over one-quarter of the 88 identified studies involved communication, cognition, or behaviour therapies. Functional outcomes such as attention, verbalization, and learning, among others, were reported. This highlighted an emphasis on enhancing functional communication in these patients. However, these studies possessed very low to low quality of evidence. In 2009, communication interventions in individuals with RTT were systematically reviewed. The authors found that “the evidence base supporting current approaches to communication interventions for individuals with Rett syndrome remains inconclusive” [104]. Only four additional studies addressing communication interventions for RTT have been published in the intervening decade.
Half of the animal studies explored the impact of environmental enrichment in mouse RTT models. Stimulating RTT mice by means of their physical and social surroundings has a range of benefits including anxiety reduction, improved motor coordination, spatial learning and cognitive performance effects [83, 84, 85, 86]. These findings potentially have downstream influences on the design of human clinical trials but should however be approached with caution as environmental enrichment studies in animals have often been criticized to be misrepresentative of human conditions [105]. Preclinical characteristics of animal studies such as dose and age at treatment onset cannot be generalized to the human population. However, concepts of functional benefit following therapy is important to note.
As with all systematic and scoping reviews, the present study was vulnerable to publication bias. Most included articles report some degree of functional improvement in response to the intervention under study; only two studies showed an entirely neutral or negative response to intervention [49, 106] and a small number of studies discussed neutral or negative secondary outcomes. As authors and journals are more inclined to publish positive results, this may have led to the over-representation of beneficial therapies.
Because the diagnostic criteria for RTT has changed over time, articles published prior to 2010 may include patients who would not meet current criteria for RTT diagnosis [2]. All studies with patients diagnosed with RTT at the time of the study were included, as the criteria by which the diagnosis was made (clinical and/or genetic) was often not specified. This is a study limitation as the findings potentially included results from individuals who were incorrectly diagnosed.
Significant heterogeneity in therapeutic interventions is apparent in this scoping review. For example, hand splint design and implementation differ widely from one study to the next. While three studies demonstrated reductions in stereotypic hand movements using similar hand splint designs [68, 107, 108], another study demonstrated similar outcomes with a different form of hand splint [109]. Furthermore, although stereotypic hand movements become more frequent during times of stress [110], it is still unclear if these behaviors are maladaptive or beneficial. This heterogeneity and lack of knowledge about natural history complicates clinical decision making and future study design. Caution should be taken, and the original manuscript should be consulted prior to making clinical treatment decisions.
Future studies will benefit from more consistent use of outcome measures, specifically those validated for RTT. Currently, there is a small number of measures that consider RTT-specific medical, behavioural, genetic, or psychosocial outcomes. These measures lack consistency and often do not consider behavioural or physiological characteristics of RTT. With some measures considering clinical severity and others only considering genetic diagnoses, these measures are inconsistent in their conclusions [111]. The inconsistency of these non-inclusive measures influences the need for comprehensive, RTT-specific outcome measures. This would ultimately help facilitate the comparison of study results and creation of cohesive conclusions to intervention outcomes.
In conclusion, this scoping review of therapeutic interventions for RTT is the first to include valuable findings from animal studies and case reports. The included studies demonstrate that there is a paucity of high-quality evidence, particularly pertaining to therapies for older individuals with RTT. Current human RTT research emphasizes the support of communication, cognition, and behaviour, while animal studies primarily examine environmental enrichment interventions. Future studies inclusive of the older age groups of individuals with RTT will provide age-specific information regarding the effectiveness of therapies at advanced points along an individual’s lifespan. Natural history knowledge of RTT and standardized, comprehensive outcome measures will inform future therapy studies if further elucidated. This review allows for an understanding of the current available approaches to improving function in individuals with RTT, which informs future research design and clinical practice.
Footnotes
Conflict of interest
The authors have no conflicts of interest to disclose.
Supplementary data
The Appendix files are available to download from http://dx.doi.org/10.3233/PRM-200683.