
Abstract
PURPOSE:
To assess the changes in balance function in children with cerebral palsy (CP) after two weeks of daily training with personalized balance games.
METHODS:
Twenty-five children with CP, aged 5 to 18 years were randomly selected for experimental or control groups. Over a period of two weeks, all participants received 8–9 game sessions for 15–20 minutes, totaling 150–160 minutes. The experimental group used personalized balance games available from the GAmification for Better LifE (GABLE) online serious gaming platform. Children from the control group played Nintendo Wii games using a handheld Wii Remote. Both groups received the same background treatment. Recorded outcome measures were from a Trunk Control Measurement Scale (TCMS), Timed Up & Go Test (TUG), Center of Pressure Path Length (COP-PL), and Dynamic Balance Test (DBT).
RESULTS:
After two weeks of training in the experimental group TCMS scores increased by 4.5 points (SD
CONCLUSION:
This study demonstrates improvement of balancing function in children with CP after a two-week course of training with personalized rehabilitation computer games.
Introduction
Balance is the ability to maintain posture or vertical orientation throughout a range of tasks from sitting and standing to walking. It depends on the complex interaction of the central neural system, muscles, strength, proprioception, positioning, vision, and the vestibular system [1]. Impairment of balance significantly affects the quality of movements in children with cerebral palsy (CP). Therefore, balance training is an important part of CP rehabilitation [2, 3].
Serious games may be defined as “digital games explicitly serving additional purposes beyond mere fun and entertainment” [4]. Promising results of serious games for balance training have been reported by different research groups [4, 5, 6, 7]. In addition to providing motor skills training for children with CP [8] these games promote motivation and engagement [7, 9, 10] and have a positive effect on brain neuroplasticity [6, 8]. Serious games have great potential to transfer rehabilitation into home settings which can considerably reduce the costs and time commitments of medical staff and families [11].
CP includes disorders of movements and posture as well as disturbances of sensation, perception, cognition, and behavior [12]. To achieve the effective motor learning of new skills, the games need to be properly adjusted to the child’s level of the motor and mental development; they should not be too easy, boring, too difficult or frustrating for the player [4, 7]. Long-time engagement and motivation can often be achieved by using an entertaining story in serious games, not just simple exercises using virtual reality [9, 14].
Prior research has shown benefits after using serious games. One feasibility study demonstrated motor benefits and engagement of the players after neurorehabilitation with serious games that included haptic feedback [14]. Significant results in head and trunk control were also found after therapy with serious video games using an adapted interface and physical exercise [15]. In a study with ten children with CP, there was a significant increase in trunk control and balance after four weeks of training with specially developed serious games [16]. However, the design and small number of participants of these trials indicate the need for further research on the effects of using special serious computer games in CP rehabilitation.
In this pilot study, we used balance games developed for children with cerebral palsy that are available on the GABLE online gaming platform, which was constructed with social networking in mind [17]. All the games could be personalized according to the player’s skills and performance level. The platform has an adjustable graphical user interface to conform to possible visual or cognitive limitations of the child. Performance can be tracked using integrated tools for evaluation of static and dynamic balance.
Our study aimed to assess the changes in balance function in children with CP during a two-week intervention using the personalized rehabilitation computer games for balance training.
Materials and methods
A pre-post quasi-experimental exploratory design with two groups was used.
Full ethical approval was obtained from the Ethics Committee of the International Clinic of Rehabilitation. Before entering the study, written informed consent was obtained from the legal parents/guardians of all participants and verbal assent was obtained from the children by the study coordinator.
Participants
Children who were admitted for a two-week treatment course at a tertiary care rehabilitation clinic from January to April 2019 were invited to participate in this study. Inclusion criteria were that the children had to be 5 to 18 years of age, diagnosed with CP and classified as level I, II or III on the Gross Motor Function Classification System (GMFCS). Exclusion criteria included the presence of uncontrolled seizures, severe intellectual disability or uncooperative behavior, i.e., failure to comply with the instructions required for assessment and computer game training.
Children interested in participation after the baseline evaluation were randomly assigned either to the experimental or control group by the number of their medical record (even – experimental, odd – control group). The experimental group used personalized balance games on the online GABLE platform. Those in the control group played Nintendo Wii games using a handheld Wii Remote. Both groups received the same background rehabilitation treatment provided routinely in the International Clinic of Rehabilitation and that is listed below. The baseline and post-intervention assessments and interventions, i.e., game training sessions were administered by the same therapist.
A total of 26 children were recruited with 13 in each group. One child from the control group failed to finish the study due to somatic illness. Patient flow is presented in Fig. 1.
Patient flow diagram.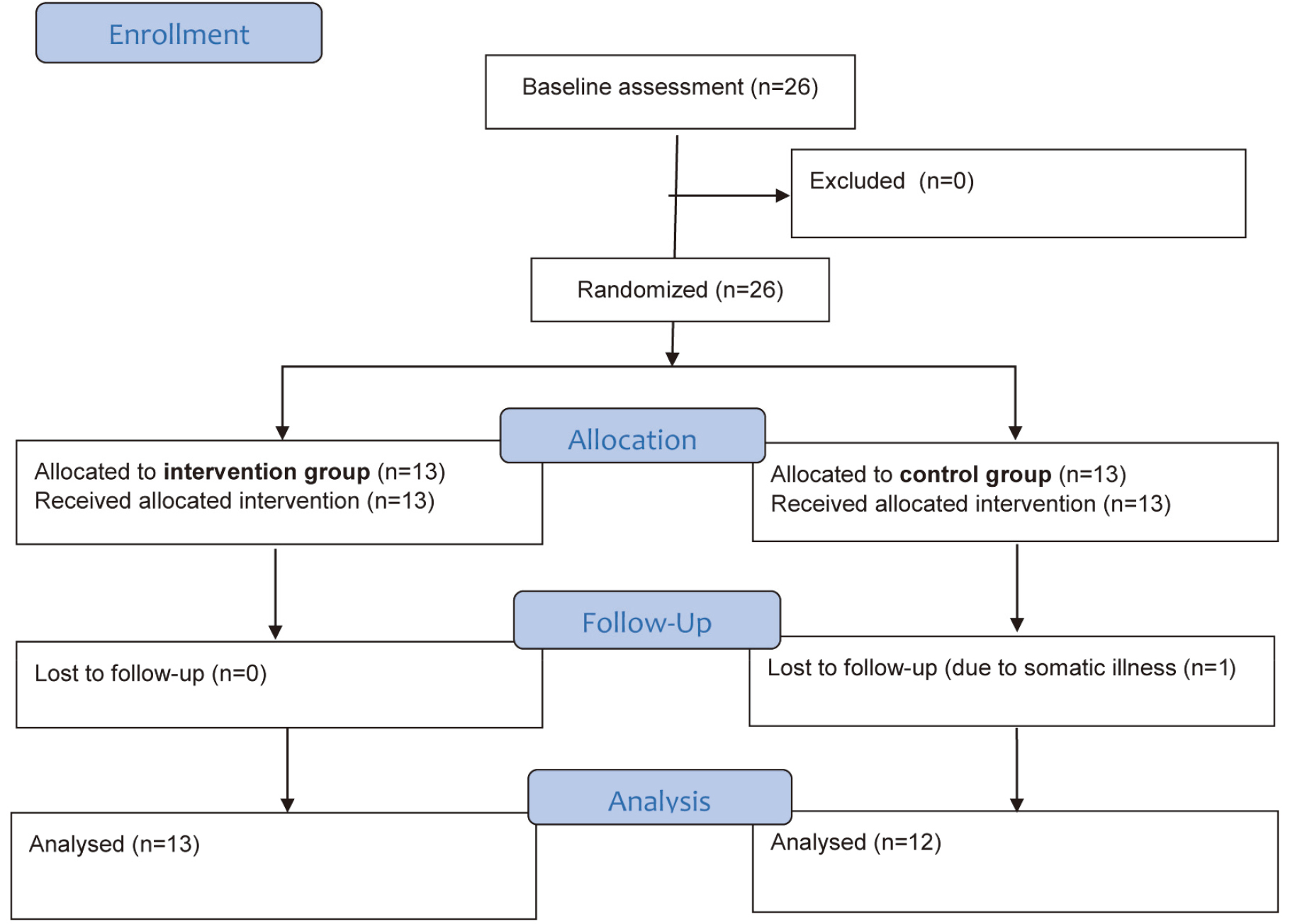
Demographic characteristics of the participants
SD – Standard deviation, CP – cerebral Palsy, GMFCS – Gross Motor Functions Classification System.
The demographics of the participants are presented in Table 1. There was no significant difference between children of the two groups by diagnosis or GMFCS level of motor development. Girls outnumbered boys in the experimental group while the number of boys was higher in the control group.
Over the course of two weeks, all participants participated in 8–9 game sessions, lasting 15–20 minutes each, depending on the individual schedules of each family. To set the same preconditions for every child, the total time after two weeks was 150–160 minutes. Game sessions were conducted by a trained physical therapist. Participants from the experimental group played personalized balance games for children with motor disabilities as described below. Depending on their abilities, participants could play games in a standing position with/without support, kneeling, or sitting on the balance board.
Children from the control group played mainstream commercial Nintendo Wii Sports and Wii Sports Resort games with the handheld Wii Remote, e.g., “Tennis”, “Bowling”, or “Golf” The game was chosen according to the level of motor function and personal preferences of the child. Participants played the games in a standing or sitting position, based on their GMFCS level. The overall time of the game sessions were the same as in the experimental group.
Both groups also received the treatment that is routinely used in the International Clinic of Rehabilitation. For two weeks, all children received daily rehabilitation treatment for up to 150 minutes, which included 40 minutes of physical therapy, 20 minutes of occupational therapy, 60 minutes of full body massage, 5 minutes of spinal manipulative therapy, 15 minutes of gait training, and 10 minutes of vibration therapy. A detailed description of this treatment is available in the Rehabilitation Specialists Manual [18].
Balance games for children with motor disabilities
The balance games used in this study are available on the GABLE online platform [15] which provides serious gaming focused on improving motor skills and visual-motor coordination of youths with CP. In addition to the possibility of being adjusted to each player’s level of motor and mental development these games offer control mechanisms that allow the caregivers to adequately monitor their progress. The platform is constructed with social networking in mind, which allows parents, caregivers, and players to socialize and share experiences and advice in a common, safe environment.
The required hardware includes a standard Nintendo Wii Balance Board connected to a personal computer using Bluetooth. Games are played by shifting body weight left-right or forward-backward while standing on the balance board according to the game action. Participants were safeguarded by a therapist or parent during the sessions, especially in cases of more severe motor disability.
Screenshots of the balance games. A. Paddle Waddle game, B. Woo’s Wonderful World Adventure game, C. Hungry Woo game.
Since children with cerebral palsy range widely in their ability to maintain balance and shift body weight in a controlled manner, the overall difficulty of each game level could be smoothly adjusted on a scale ranging from 0 to 1. The Analytics Module of the GABLE platform analyzes the previous performance of each child, tracks ongoing performance, and suggests a suitable difficulty level for each user in a particular game according to their individual skills. Games have at least 10 “official” levels, with slightly increasing complexity of each progressive level. Official levels are fine-tuned and personalized by the therapist who customizes all important game parameters using a Level Editor. To keep the child engaged in playing for a longer time, levels include different backgrounds, colors, sound effects, and game objects. Also, the therapist or parents can create customized levels for each child.
As children with CP often have a restricted range of motion, balance games should be calibrated according to their capabilities. While standing on the balance board the child’s task is to shift their weight left-right or forward-backward to determine the range in which they can play each game.
Children from the experimental group played the following games: “Paddle Waddle” “Woo’s Wonderful World Adventure” and “Hungry Woo” (See Fig. 2).
The Trunk Control Measurement Scale (TCMS) was the primary outcome measure. TCMS is a clinical test to assess sitting balance in children with CP with good psychometric properties reported for both research and clinical settings [19, 20]. All participants were assessed in the sitting position on a treatment table. During administration of TCMS, one can quantitatively measure trunk control during functional activities [18]. This test includes three subscales (15 items in total) assessing both static and dynamic aspects of trunk control. The TCMS items examine different aspects of static sitting balance, selective movement control, and dynamic reaching. Every item is graded on a two-, three-, or four-point ordinal scale. The total maximum score for all items is 58 points.
The secondary outcome measures were: Timed Up & Go Test, Center of Pressure Path Length, and Dynamic Balance Test.
The Timed Up & Go (TUG) Test is a clinical tool widely used to evaluate the functional mobility of adults. It is proven to be a reliable and objective measure of functional mobility in children with CP [21, 22]. During the test the participant stands up from the chair, walks 3 meters, turns, walks back to the chair, and sits down. The time it takes to complete these tasks in seconds is recorded.
The Center of Pressure Path Length (COP-PL) was measured using the Static Balance Assessment Tool, a component of the GABLE platform developed for measuring basic stabilometry parameters [23].
This tool calculates the displacement of the center of pressure while a person is standing still on the Nintendo Wii Balance Board. An average of three trials of ten seconds each is used to calculate the main displacement and speed parameters in both anterior-posterior and medial-lateral directions. The calculations of the Static Balance Assessment Tool were verified by comparing their results with data measured with the “classical” Stabilometry or Posturography [25, 26].
At the end of the test, the evaluator can see the following stabilometry parameters: COP-PL, area (the area of the 95% confidence ellipse), root mean square of displacement, the distance between the maximum and minimum centre of pressure displacement, mean velocity, and total mean velocity.
The Dynamic Balance Test (DBT) is another diagnostic tool integrated into the GABLE platform. It measures the ability of the child to shift their body weight precisely. To perform the DBT, a child stands on the Nintendo Wii Balance Board and shifts their center of gravity to the left or to the right according to the screen instructions. They hold the position within the specified limits for 3 seconds. The limits for holding the position narrow with each round requiring more precise balancing. The number of rounds completed within the specified time characterizes their balancing capabilities.
In this study the number of completed rounds was added to the time remaining after completion of the last round. The time in seconds is converted into a number as a fraction of one minute. For example, if 7.3 seconds are left after the last round, this is converted into 0.122 points (7.3/60
Statistical analysis
Statistical analysis was performed using IBM SPSS version 23 software. The normality of distribution was checked using Kolmogorov-Smirnov and Shapiro-Wilk tests. For variables with normal distribution, parametric statistics were used, and pre-post differences were calculated using the paired sample
Results
Results of the baseline and post-intervention assessments are presented in Table 2 and Fig. 3. Since TCMS variables have normal distribution during all the measurements, parametric methods were used to process them. Distribution of the DBT, COP-PL and TUG values violated normality assumption, so non-parametric statistics were used.
Results of the baseline and post intervention assessment
Results of the baseline and post intervention assessment
SD – standard deviation, IRQ – Interquartile Range,
Results of the baseline and post intervention assessment.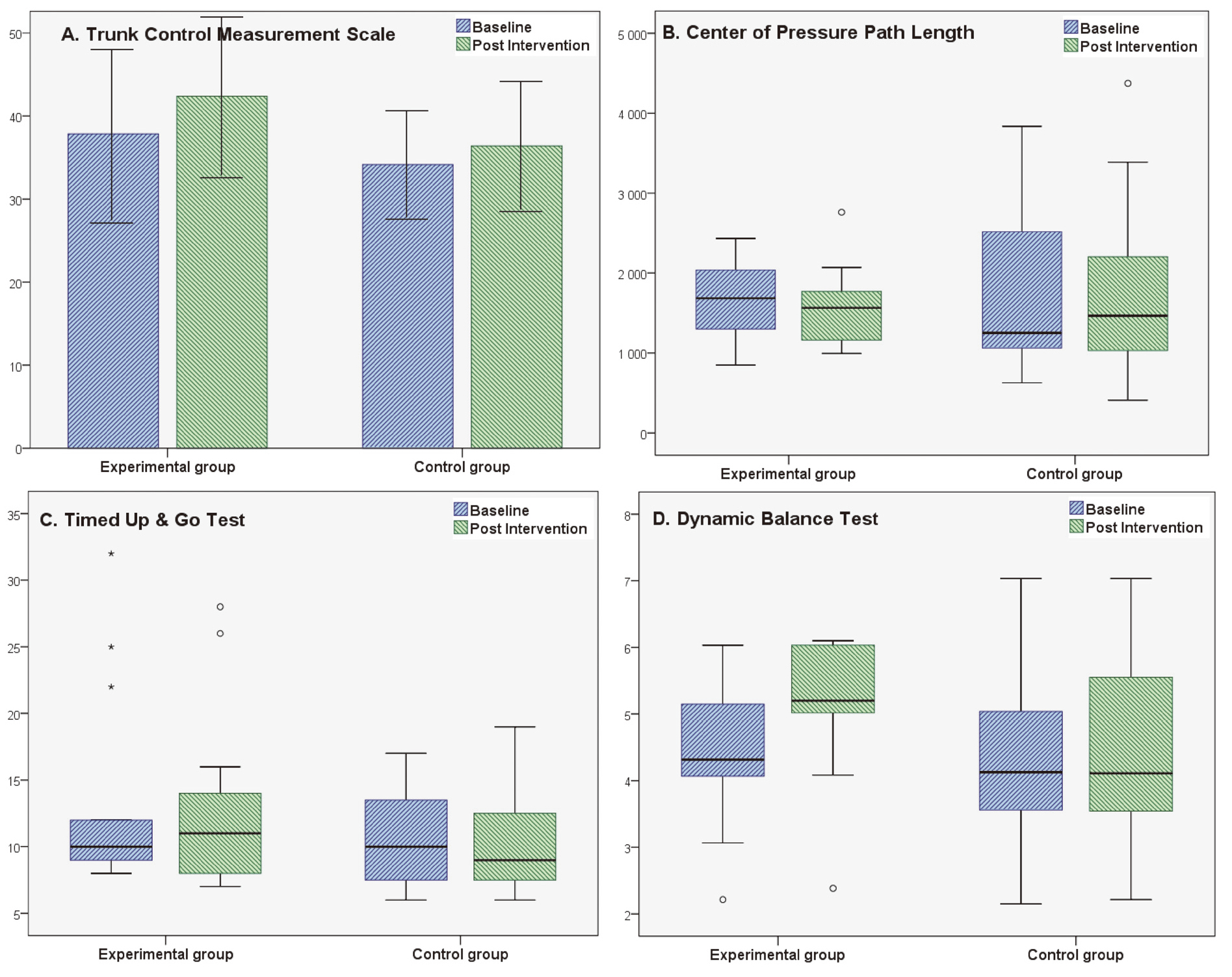
The primary outcome measure was the TCMS (Fig. 3A). Higher values in the TCMS score represent better balance and trunk control. In the experimental group, a statistically significant improvement of 4.5 points (SD
The secondary outcome measure was the COP-PL evaluated using the Static Balance Test (Fig. 3B). Lower values of this parameter indicate a better static balance. A decrease of the median of the path length by 116 mm (IQR
The TUG test (Fig. 3C) was another secondary outcome measure, with lower times indicating better performances. Changes of the TUG score, measured before and after the intervention were not statistically significant in either experimental or control group. Median values of TUG test results decreased by 1 second (IQR
Another secondary outcome measure was the DBT (Fig. 3D). Higher DBT values indicated a better dynamic balance of left-to-right sways. In the experimental group, DBT median values improved by 0.88 points, and this was statistically significant (IQR
Since statistically significant changes were noted in TCMS and DBT, those changes were compared between the experimental and control group. For the TCMS mean, the between-group difference was not significant at 2.29 points (
Positive changes of balance were observed in children with CP after a two-week course using personalized rehabilitation computer games. In particular, statistically significant differences were indicated in the TCMS and the DBT scores. The control group did not significantly change from baseline.
The TCMS change of 4.5 points in the experimental group surpassed the smallest detectable difference (SDD) of 4.39 points for intrarater reliability [27]. Another study previously defined the SDD as 4.66 points for intrarater reliability, but it was conducted earlier and included a relatively small number of participants [20].
The TCMS difference in the experimental group had an effect size of 0.43. According to Cohen’s classification, this is a small effect. Therefore, we can define the TCMS results in the experimental group after just 8–9 training sessions as statistically significant with a small effect.
As for DBT score, the statistically significant change of 0.88 points in the experimental group constituted 20.4% of the baseline value of this group. This change has a medium effect size of 0.78. Therefore, these changes can be interpreted as statistically significant with a medium effect.
A possible mechanism for the improvement of TCMS and DBT scores is a similarity in the movements required for a successful game session while performing these tests [11]. As an illustration, one item of the TCMS tests participants’ ability to touch the table with their elbow [17]. This movement is possible only with sufficient lateral trunk flexion that is also needed during game sessions with the GABLE platform. Likewise, participants need to shift their body weight and hold this position both during DBT and the balance games.
TUG scores did not change significantly in any of the groups, likely because the balance games were intended to focus on balance rather than walking ability. Additionally, detection of the change in TUG is reported to be affected by the duration of follow-up, meaning that two weeks may have been insufficient to allow for the final assessment [28].
The COP-PL test result changes were not significant in any of the groups either. This might be due to the high variability of the data. Alternatively, it is possible that the stabilometry measure simply did not change during the short two-week training with GABLE games.
Children in the two conditions had different exposure to the balance board: while the experimental group was more familiar with this device due to the computer game sessions, participants from the control group used it only during assessments. This could potentially have affected the results of the final assessment. To address this, we chose to use the TCMS, which was performed without the balance board, as a primary outcome measure. Since the GABLE platform includes both the Static Balance Assessment Tool and the DBT, we also included them as secondary outcomes. Given that participants received the same treatment other than the unequal exposure to the balance board, we presume that changes in the trunk control and dynamic balance might have occurred because of the training with special balance games. Previously, similar results were obtained by another research group that used a specially developed gaming system [17].
Since our multidisciplinary team is employed at institutions that have part ownership of the GABLE online rehabilitation gaming portal, this could potentially influence the results of the study. To minimize this possibility, the therapist involved in administration of this study was placed in a tertiary care clinic that was not involved in the development of the GABLE platform. This employee completed allocation using the parity of the last number of the individual medical record and performed the assessment and treatment administration for both groups. The therapist did not take part in either data analysis or in preparing the manuscript. However, the lack of blinding may still increase the risk of bias.
Another possible limitation was the short period of intervention. The reason for only two weeks of game sessions is that it is the standard duration of the rehabilitation treatment in the clinic where this study was conducted. To compensate for this limitation game sessions were conducting every day.
This pilot study included a limited number of participants and served to plan a future clinical trial. The difference between the experimental and control groups in the change of TCMS score was not statistically significant
In conclusion, our pilot study revealed a statistically significant improvement of the TCMS and DBT results in children with CP after a two-week course of intervention with personalized balance games. A possible reason for the achieved results is that the game features were properly adjusted to each player’s developmental level ensuring effective motor learning without losing interest or motivation [8]. Data obtained during the study will help to prepare a future randomized controlled study aimed at evaluating benefits of the special serious computer games on the balance of the children with CP.
Footnotes
Acknowledgments
The authors thank all children and their caregivers who agreed to participate in this study.
This study is conducted as a part of the Horizon 2020 project GABLE which has received funding from the European Commission Horizon 2020 research and innovation program under grant agreement No 732363.
Conflict of interest
The authors of the manuscript are employed at institutions that have part ownership of the GABLE online rehabilitation gaming portal.