
Abstract
This case study documents a 13-year-old female who presented to our intensive inpatient chronic pain rehabilitation program with complex regional pain syndrome (CRPS) of her left leg, which was significantly interfering with her normal daily functioning. She participated in a full day of traditional interdisciplinary therapies, including physical and occupational therapy for 3 hours daily. As assistive equipment was altered or weaned her physical mobility, balance, and tremors worsened and/or increased. As she began advancing her legs more independently (versus requiring physical assist), she demonstrated more variable functional strength and stability, inconsistent balance reactions, and a more unsteady gait pattern. The team was treating her according to her incoming CRPS diagnosis; however, as treatment progressed, her physical and psychological presentation seemed more aligned with diagnostic criteria of functional neurologic symptom disorder (FND). Staff then treated according to the FND diagnosis resulting in successful long-term outcomes. The clinical impact from this case study includes highlighting the commonalities between CPRS and FND clinically, discussing treatment suggestions depending on the diagnosis, and emphasizing key components of family/patient education.
Keywords
Abbreviations
Introduction
Pediatric treatment for complex chronic pain diagnoses can be challenging due to the multifaceted nature of diagnoses, treatment options, and variable outcomes. Terminology has been changing over the past decade for complex diagnoses, such as complex regional pain syndrome (CRPS) and functional neurologic symptom disorder (FND). At times, diagnostic and treatment criteria are not properly reflected in many systematic reviews, making it challenging for clinicians to find information on prognosis, treatment, and outcomes. In addition, both diagnoses are complex, have biopsychosocial comorbidities, worsen over time, and often have poor outcomes [1, 2, 3]. Multidisciplinary treatment is recommended for best outcomes with CRPS and FND [4, 5].
CRPS is a pain condition affecting limbs which is believed to be caused by damage or malfunction of the peripheral and central nervous system with alterations in brain function. This causes high levels of nerve impulses and pain signals, immune and autonomic responses, and has physical and psychological characteristics that impact functioning. Common characteristics include allodynia, edema, cyanosis, tremors, fear-avoidance, and kinesiophobia. Magnetic resonance imaging (MRI) has shown reductions in gray matter almost immediately in sensory, motor, emotional, cognitive, and pain modulatory regions of the brain which only improve with treatment [6, 7]. CRPS can be synonymous with reflex neurovascular dystrophy (RND), reflex sympathetic dystrophy (RSD), or causalgia [3, 8, 9, 10, 11]. Also, CRPS can often be misdiagnosed simply as an amplified pain syndrome [5]. There are around 5,500 new cases every year [12] and CRPS is commonly associated with anxiety and depression [5, 8, 13, 14].
FND is a condition in which neurologic symptoms of psychological and/or physical nature are present without changes in the brain structure. With FND, there tend to be triggered or worsened clinical manifestations due to external stimuli that can include physical, social, or emotional components and cause increased self-attention to symptoms [15]. Other diagnostic labels with similar conceptual understanding and incompatible pathophysiology include conversion disorder, psychogenic movement disorder, functional movement disorder, and non-epileptic seizures [16, 17, 18]. Although prevalence in pediatric populations is elusive, it is common among adolescent females, highly associated with stressful events and frequently occurs with co-morbid anxiety and depression [19].
FND and CRPS are caused by abnormal, malfunctioning nervous systems and have clinical overlap and common pathology. Ensuring that patients are diagnosed and treated properly is imperative as there are subtle differences and necessary adjustments in treatment and education strategies that should occur for each entity. While a patient with CRPS participates in intensive rehabilitation, it is not uncommon for the team to notice that their FND symptoms are contributing more to their impaired function. Psychology, physical therapy (PT), and occupational therapy (OT) play an important role in multidisciplinary rehab for these complex diagnoses [15]. There are several areas of focus for this case study. First, this case study aims to highlight the commonalities between CPRS and FND from a clinical standpoint. Secondly, this case study intends to bring awareness of the changing clinical presentations so clinicians can best treat complex patients and provide optimal care. Lastly, it is important to educate families and patients about new or different diagnoses which providers may consider or add, explain how they impact or change care, and discuss how they might impact them long term.
Physical and Occupational therapy case outcomes with admission, discharge, and follow up information. (Pain, LEFS, UEFI, planks, step ups, COPM).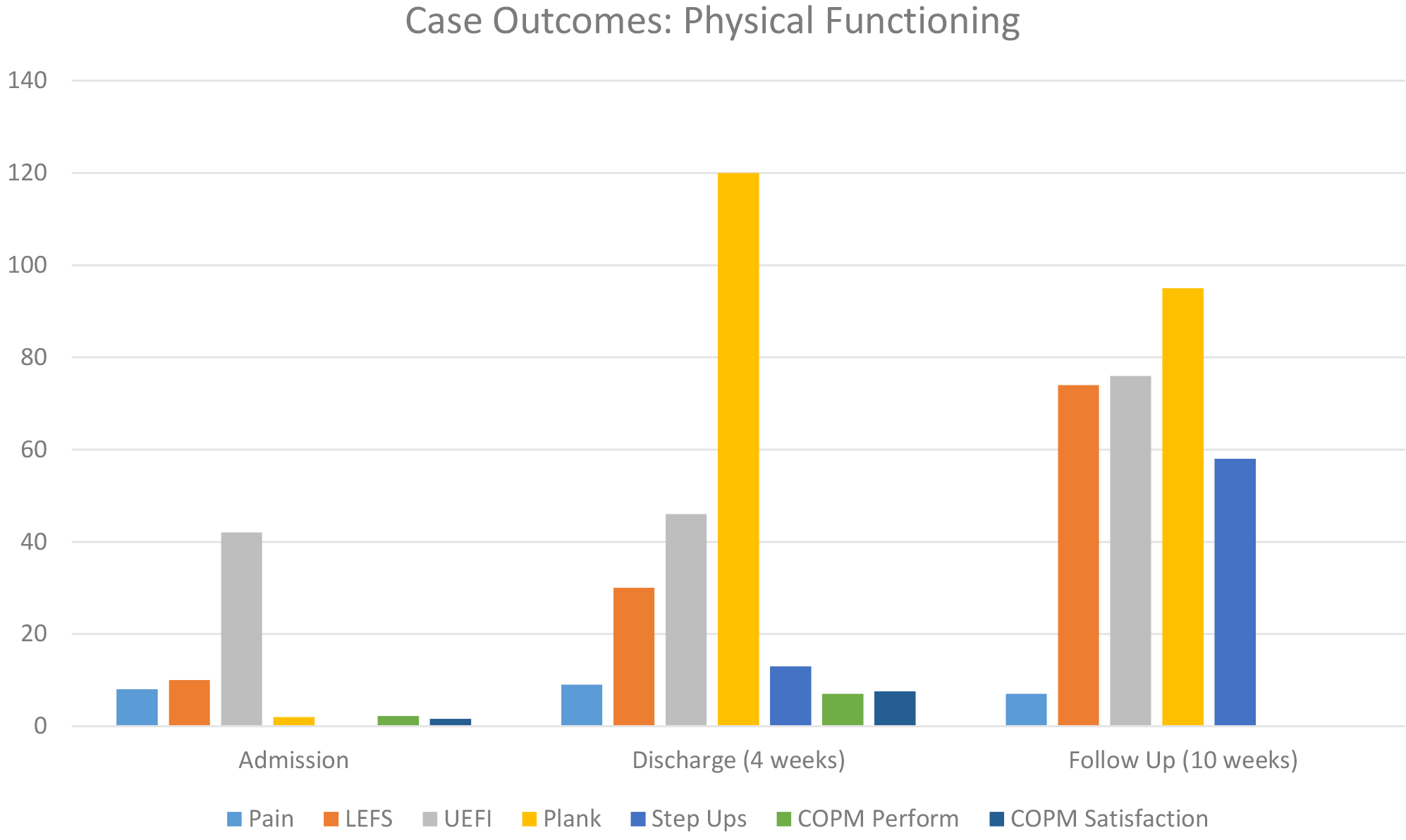
History
A 13-year-old female presented to clinic due to a diagnosis of CRPS of her left leg which was significantly interfering with her normal daily functioning. She had a significant past medical history that included depression, conversion disorder, panic attacks, and a more recent diagnosis of generalized anxiety disorder. In addition, she had a history of frequent sprains and peroneal tendonitis secondary to dance.
She reported that her pain began while on a hiking trip, without inciting injury, three months prior to admission. She was seen by a doctor upon return home, and it was recommended that she use crutches with weight-bearing as tolerated for her left lower extremity. Her pain increased, she began having color and edema changes, and was eventually diagnosed with CRPS.
Outpatient services
Upon receiving a diagnosis of CRPS, she began attending outpatient physical therapy 1–3 times per week with chronic pain providers at a nearby hospital. She then began having foot drop and numbness episodically which improved after three weeks of intensive physical therapy. A few weeks later, she became unable to move her lower extremities which resulted in the use of a wheelchair for mobility. Her family sought alternate interdisciplinary treatment for chronic pain and temporarily transitioned care to this out-of-state therapist’s team.
Admission to interdisciplinary pain rehabilitation
On the day of admission to the program, she reported she had pain (8/10) in both legs, abdomen, hands, back, neck, and shoulders which was described as “sharp, stabby, radiating, and spider webby.” She had poor proprioceptive awareness including difficulty identifying left and right side as well as positioning, and she felt variable numbness, tingling, or pain in both legs. She reported feeling that weakness changed “day-to-day.” Pain was worse with activity, temperature changes, stress, school, and light touch. Pain was better with distraction and heat. Although her diagnosis had not changed, the admitting team was suspicious that the patient also had FND.
Admission evaluations
Initial data collection and admission assessments were limited due to clinical presentation and difficulty with active motor planning. Staff had to rely greatly on patient/family reports, observed functional mobility, and visual assessments without manual input in order to gauge strength and endurance. With CRPS and/or FND, it is highly challenging to get accurate and appropriate manual muscle testing, active range of motion assessments, and completion of standardized testing due to sensitivity to touch (allodynia), fear avoidance, kinesiophobia, and difficulty with body awareness, especially before clinicians have built appropriate rapport [8, 20].
During her medical evaluation, she had positive signs of edema and cyanosis in both of her legs. She was currently taking Zoloft for anxiety and had previously trialed gabapentin, Flexeril, and ibuprofen with no improvement and some mild side effects. Prior diagnostic testing was all within normal limits including a thoracolumbar MRI, left ankle X-ray, and labs (Erythrocyte Sedimentation Rate (ESR), Complete blood count (CBC), C-reactive protein (CRP), Thyroid Function Tests (TFTs), and Basic Metabolic Panel (BMP)). There were no documented abnormalities on neurologic exams on the day of her admission.
During her PT evaluation (Fig. 1), she demonstrated trace lower extremity activation in all planes of motion bilaterally. However, she demonstrated increased active range of motion with transfers and other functional mobility tasks when paying less attention. She tolerated wearing shoes and socks, utilized a self-propelling wheelchair with her upper extremities, and was agreeable to ambulating short distances with a walker. With ambulation, she required assistance to advance both legs and used a shuffling pattern with the absence of knee flexion, hip flexion, and ankle control. She was only able to ambulate 7 feet using a rollator walker during the 6-minute walk test and was unable to complete or trial all other functional testing for lower extremity strength secondary to decreased mobility, balance, and strength. Lastly, she scored a 10 out of 80 on the lower extremity functioning scale (LEFS). The LEFS is a self-report tool that can track perceived functioning specific to the patient’s ability to perform everyday tasks using their lower extremities. Individuals rate each item on a 0–4 Likert scale (0
During her OT evaluation, she reported decreased proprioception and kinesthetic awareness and was hyposensitive during her tactile sensory system assessment. She was only able to complete one of four functional strength tests for the upper extremities secondary to decreased mobility, balance, and strength. She scored herself a 42 out of 80 on the upper extremity functioning scale (UEFI) which is a self-report tool that can track perceived functioning specific to one’s ability to perform everyday tasks using upper extremities. Individuals rate each item on a 0–4 Likert scale (0
Case discussion and outcomes
The patient participated in a 4-week interdisciplinary pain program with inpatient and day hospital treatment components. The program included 3 hours of PT and OT per day, recreation therapy, psychology (individual and group), medical services, and educational services to stay caught up on schoolwork.
Similar and differentiating characteristics of FND and CRPS, and specific characteristics of case example for comparison
Similar and differentiating characteristics of FND and CRPS, and specific characteristics of case example for comparison
No structural correlate for motor and sensory symptoms on routine imaging.
As she completed functional activities more independently and assistive equipment was altered or weaned, staff from various discipline noticed abnormalities in her gait and functional mobility. As she began using her legs more independently (without assist to scoot foot forward as initially required), she was noted to have an unsteady gait pattern, less reliable functional strength, inconsistent balance, and more frequent non-epileptic events (i.e. lowering to floor with appropriate eccentric control, inability to respond to verbal cues, limited visual tracking, and poor recall of events following). Staff documented gait as “excess rhythmic movement in all planes of motion at all lower extremity joints and pelvis” and “inconsistent foot placement, altered cadence, and heavy reliance on upper extremities.” By the end of her first week, despite other physical challenges, staff noticed her color changes and swelling seemed to be resolved.
This case had significant complexity as the patient met criteria for both CRPS and FND diagnoses and her physical presentation varied, not based on specific challenge level or activity. For example, she could complete more advanced balance skills with better technique and stability than typical mobility and her presentation became worse with specific cues about her technique. As seen in Table 1, her physical presentation contained many similar characteristics of both CRPS and FND [15]. Although her initial diagnosis was CRPS, her physical and psychological presentation seemed to highlight that FND was impacting her participation and functioning to a greater extent than the CRPS.
The patient had a daily program to complete in addition to daily therapy intervention. This program included daily stretching (3 times per day), strengthening (20–30 minutes per day), and sensory (every 2 hours) activities. Primary treatment techniques included treadmill training, standing endurance and stability activities, functional mobility skills, floor ladder sequencing, motor planning activities, balance reaction strategies, and proprioceptive input. Weaning of assistive equipment to the least restrictive device was an initial goal, along with a gradual increase in functional mobility skills and dynamic challenges. Therapy staff utilized typical rehabilitation interventions for mobility and gait; however, abnormal movement patterns were generally ignored unless deemed unsafe. PT and OT treatments highlighted that diagnosis and pain related to exercise were not correlated with worsening structural damage and that motor retraining was key [15]. Staff focused on the patient first being able to do skills without assistive equipment or external support before working on improved technique or form [24]. Staff focused more on what she could do or did well, versus what she couldn’t do, to help her gain confidence in physical abilities as seen with behavioral shaping and modification [25, 26, 27]. Also, the clinicians made sure to verbalize acceptance of the diagnosis and physical symptoms versus challenging physical abilities [28].
In psychology, there is much focus on assessing social, emotional, and cognitive risk factors and bringing patient awareness to these risk factors [15]. In addition, since research has shown that anxiety and pain are linked closely with CRPS and FND [3, 29], it was imperative that she worked on anxiety and stress management. Included in the initial treatment were definitions and manifestations of anxiety, how stress impacts functioning, and how to identify anxiety and stress before it impacts pain and functioning. Specific to FND, it has been found that the level of somatization can impact outcomes. Psychological treatment often involved recognizing how stress, depression, and anxiety manifested and impacted function, altering thoughts and beliefs about symptoms, and helping family to understand the occurrence of new symptoms and appropriate treatment [30].
Parents also participated in education with various interdisciplinary team members [31]. Psychology met with both the patient and available family members at least once weekly with an individual focus. They also participated in a parenting group run by social work and psychology twice weekly, focusing on general pain, specific parenting skills, and strategies. Physical and occupational therapy provided individual education regarding her participation, effort, the progression of skills, and discharge planning as needed. To support her progress short and long term, family education focused on skills parents needed to know to better understand her diagnosis of FND, current clinical presentation, and typical rehab progression. It was also geared to help them gain essential skills to guide continued and ongoing functioning once home (i.e. relapse prevention, behavior modification, self-wellness, life balance, and creating routine/maintaining structure, etc.).
Outcomes (Fig. 1)
At discharge, she participated in all functional strength tests, reported improved self-assessment of functional abilities, and ambulated safely without a device (still with variable stability and technique). It should be noted that the patient’s pain level was fairly stable both pre and post treatment, demonstrating an improvement in functioning despite the continuation of pain symptoms. Her motivation to return to dance and her eagerness to participate in therapies facilitated functional gains.
Examples of therapist cuing and focus depending on FND or CRPS diagnosis
Examples of therapist cuing and focus depending on FND or CRPS diagnosis
Upon return home, the patient sustained two acute injuries (mild concussion, wrist sprain) which were associated with mild relapse. During this time, family promoted continued function using appropriate modifications without assistive support. The patient also continued with outpatient physical therapy and psychology. At follow-up 10 weeks post-discharge, her self-reported function and physical function were further improved. She had returned to high-level dance, was helping to teach dance to younger students, was attending school regularly, and gait abnormalities had resolved. Eighteen months post-discharge, she maintained function. She had fully resumed all activities which included participating in a sleep-away camp, regularly attending school, and partaking in high-level dance consistently.
Feedback from the family was provided regarding the patient’s diagnoses, treatment, and outcomes to support this case report. Her father stated, “The patient considers herself recovered from both CRPS and FND. She was generally functional after leaving the program. Recurrences of CRPS and FND did happen secondary to routine injuries such as hitting her head or minor injuries with amplification of normal pain. A year after the program, we passed an invisible milestone and have had normal responses to routine injuries since then. She has recently indicated that nerve pain gradually faded in the months following the program and that pain is generally not present.
“The comprehensive program with parent education was tremendously helpful. Focusing on function and the patient as a whole was critical. FND can lead to a lot of symptom chasing, but we had a framework that was ultimately very simple. We couldn’t have gotten as far as we did without understanding the many interconnected and counter-intuitive things we were dealing with. A major turning point in getting back to normal activity for the patient was as a volunteer teaching ballet to 3-year-olds. She was able to return to this before she returned to her own dance and it made huge improvements to her well-being. As parents, we gained a lot of specialty knowledge and readily share it with other parents going through similar challenges.”
Discussion
Similarities and differences of treatment
As both CRPS and FND involve abnormal malfunctioning of the nervous system, general treatment interventions and goals are similar. The goal is to improve functional mobility and help the patient to self-manage pain and symptoms more independently [14, 28]. Also, it is emphasized that pain with exercise is not related to damage occurring and that motor retraining is key. For both diagnoses there is also shared importance on the psychological aspects and risk factors that play a role in functioning. The difference between treatment of FND and CPRS lies within the approach taken including the language or terminology used, education, expectations, and progression of skills. In addition, specific to FND, treatment evidence is limited and largely opinion-based using clinical knowledge [32].
When treating CRPS, therapists ensure proper technique and progression of weight-bearing and specific attention is drawn to compensatory strategies through non-involved areas of the body (i.e. pelvis, trunk, non-involved extremity, etc.). Bracing and the use of assistive equipment is used to support alignment due to weakness. It is suggested to ensure proper alignment and safety as patients work on increased mobility and higher-level skills and then can be weaned later on [33]. However, this should not include immobilization as that is contraindicated for CRPS [34, 35].
Patients with FND typically feel they lack control over their limbs (i.e. dissociative) but at the same time tend to spend too much time attending to limbs and movement expectations [15]. Clinically, this team has found that an over-focus on technique or specific attention to involved limbs seems to worsen or increase symptoms and is often counter-productive (see Table 2) [36]. In addition, often it is not helpful to use bracing that stabilizes or immobilizes specific body areas as they can be challenging to wean as a patient’s body begins to rely on them over time [24, 28]. Bracing can also increase attention to involved limbs and foster self-doubt regarding physical ability to function more independently. Bracing should be considered with caution, keeping in mind other psychological comorbidities, current mobility level, and level of deconditioning (bone density, contractures, and muscle strength). With FND, it is important for clinicians to emphasize the importance of the patient understanding their own motor symptoms specific to FND and consider psychological comorbidities separately (i.e. understanding how stress impacts mobility, pointing out how an over focus on body area and expectations results in worsening of mobility and increased frustration, etc.) [15].
Additionally, with CRPS, the patient begins to “neglect” the limb by not using it as often or appropriately, which becomes worse over time [15]. With brain plasticity and gray matter changes in mind [6], pain causes a negative adaptation and decrease in function. They tend to pay increased attention to the pain that movement causes with anxiety and depression worsening over time leading to kinesiophobia [13, 37]. With FND, they may feel as if the limb(s) are not connected to their body and/or mind (i.e. they don’t have full control), overly self-monitor limb movement or technique, and struggle to use the limb either because they do not know how or they have fear of pain [15, 36]. With brain plasticity in mind [38], the stress associated with patients not being able to move their body when and how they want to results in a negative adaptation and decreased functioning. This can significantly impact areas of focus and technique for verbal cuing by clinicians as they work with those with CRPS and FND. Table 2 provides further examples of verbal cuing specific to diagnosis.
Case discussion
This case was fairly complex for our team due to the patient’s initial co-morbid diagnoses, variable clinical presentation, mobility issues, and non-epileptic events early in the program. The team collaborated to ultimately determine that treatment should be altered to primarily treat the patient’s FND in order for her mobility and functioning to progress.
CRPS and FND have similar diagnostic and clinical characteristics and both benefit from intensive, interdisciplinary treatment with a focus on restored functional mobility, patient education, and focus on resolution of symptoms over time [8]. A few factors that played an important role in outcomes included the team recognizing and addressing how diagnoses were impacting treatment and participation, changing how and what staff worked on clinically, and the patient and family’s openness and internal motivation. Also, parents reported that parenting interventions, education, and understanding played a large role in long term functioning and continued relapse prevention.
The patient’s improvement in functioning demonstrates the utility of intensive pain programs in effective treatment of FND and other functional disorders due to the interdisciplinary nature. In summary, there are several ways in which this case report can provide clinical impact. First, this case report aims to highlight the commonalities between CPRS and FND from a clinical standpoint. Secondly, this case report intends to bring awareness to the changing clinical presentations so that clinicians can best treat complex patients and provide optimal care. Lastly, it is important to educate families and patients on new or different diagnoses clinicians may consider or add, explain how it impacts or changes care, and how it might impact them long term.
Funding
No funding was received for this study.
Footnotes
Conflict of interest
The author does not have any conflicts of interest to report.