
Abstract
PURPOSE:
Though knowledge of normal childhood developmental milestones, essential for physician subspecialists, begins in medical school, it continues in pediatric subspecialty residency and fellowship training. Despite widespread education in developmental milestones, published curricula related to this content area are lacking. This pilot curriculum was developed to address the lack of published developmental curricula.
METHODS:
Participants included pediatric rehabilitation trainees who completed 8–12 sessions per year of a novel, adult-learner centered child development curriculum, for two consecutive years. Outcome measures included a novel survey, knowledge based test, verbal feedback sessions, and the end of the year program evaluation committee meeting.
RESULTS:
Trainees were successfully able to attend curricula sessions within their typical fellowship and residency responsibilities. Pediatric rehabilitation medicine fellows reported improved competence in normal growth and development. Pediatric rehabilitation residents rated the curriculum as a high value to their education (3.5
CONCLUSION:
This study introduces a novel approach to developmental milestones education that is tailored to the adult learner and pediatric rehabilitation trainees.
Introduction
Normal childhood developmental milestones are taught at every level of medical training. The Liaison Committee on Medical Education requires that medical school curricula include “content and clinical experiences related to…each phase of the human life cycle” [1]. To meet this requirement, medical schools require a pediatric clerkship during the clinical years. This rotation is typically the first exposure to childhood developmental milestones for budding physicians. Medical schools choose how to cover this material, however very few publications describe curricula to educate on developmental milestones. Eddins-Folensbee et al. presented a multi-module, comprehensive curriculum to teach child development along with factors that influence development to medical students. Their curriculum includes modules on: developmental neurobiology [2]; familial, extrafamilial and cultural influences on development [3]; psychosocial, psychosexual, cognitive, and moral “lines” of development [4], developmental theories/frameworks for infant development [5]; developmental theories/frameworks for adolescent development [6]; and the impact of chronic illness on development [7]. Another peer-reviewed curriculum to teach childhood developmental milestones to medical students presents information in a podcast format and teaches the approach to a developmental evaluation as well as developmental milestones [8].
For many physicians, especially those training in pediatrics and the pediatric subspecialties, further understanding of childhood developmental milestones will be essential. However, published residency and/or fellowship training curricula relating to this important content area are lacking. Pediatric rehabilitation is one specialty which requires in depth knowledge of childhood developmental milestones. “Growth and development” is a targeted knowledge area for the Part I Certification Examination by the American Board of Physical Medicine and Rehabilitation [9]. In addition, the pediatric rehabilitation medicine milestone project stresses the importance of childhood development with the inclusion of a medical knowledge milestone related to this content area [10].
Two pediatric rehabilitation training programs are supported at our institution. Previously, trainees from these programs noted that educational activities dedicated to learning normal childhood development were suboptimal and requested additional learning opportunities. More specifically, on the annual program survey, more than 50% of the respondents strongly disagreed that the training program facilitated competence in normal growth and development. Anecdotally, this concern was shared in previous years as well. Thus, this report discusses the curriculum that was developed to address the trainees’ concerns.
Methods
Curriculum development and related educational theory
The target audience for this curriculum was pediatric rehabilitation trainees (pediatric rehabilitation medicine (PRM) fellows and triple board pediatric rehabilitation residents). No pre-requisite knowledge was required, however learners were encouraged to review applicable developmental milestones prior to each session.
This curriculum was developed with the adult learner as a primary focus. Components of various educational theories and concepts were utilized as the basis for the curriculum. The first was Knowles Andragogy Model of Adult Learning [11, 12]. The aspects of this theory that were used in this curriculum included: a self-directed learning style, covering topics relevant to learner’s current education, completing curriculum during pediatric rehabilitation training where it is necessary to know the developmental milestones, and ensuring learners understand the importance of developmental milestones as they relate to a career in pediatric rehabilitation. Learner sensory preferences were also considered when developing the curriculum [13]: Each learner prefers using different senses when learning and tend to be most successful when information is presented with their preferred sense (i.e., auditory, visual, kinesthetic). In developing the curriculum, close attention was given to including components that would appeal to as many of the senses as possible and presenting the same information in multiple ways. The final learning concept that was incorporated was promoting positive transfer: Transfer is defined as “the ability to learn in one situation and then use that learning…in other situations” [13]. Various strategies were used to ensure that transfer was likely to occur. Each session was limited to learning a small amount of new knowledge (i.e. focused on a specific age group for each session). Connecting past-learning was promoted by asking about previously discussed developmental milestones at the beginning of each session. Lastly association was promoted by having the learners create a drawing of a fictional “person” to associate with a particular developmental age.
Implementation
This pilot curriculum was implemented at a large pediatric hospital in the Midwest. The curriculum encompassed 8–12 sessions. (Note: The first year included 12 sessions, but after completion of the first year and trainee feedback, the number of sessions was decreased to eight.) (Fig. 1). Each session consisted of a review of developmental milestones for the particular age, discussion regarding specific details related to these milestones, viewing of publicly accessible videos demonstrating important milestones, and drawing a typical child that incorporated normal developmental milestones. All of these aimed to promote retention of milestones. Trainees began this curriculum in their first year of PRM fellowship or PGY-2 year of the triple board pediatric rehabilitation residency. Each session was approximately 20–30 minutes in length and was structured such that the first ten minutes were spent reviewing developmental milestones for the particular age (based on pre-reading by the trainees). Approximately 2 minutes were spent distributing the summary handout and discussing any milestones that were not originally discussed. Five to ten minutes were spent viewing of videos depicting children performing milestones, and the last ten minutes were spent with the trainees creating a drawing of a person/character to associate with developmental age.
Sessions included in curriculum by year.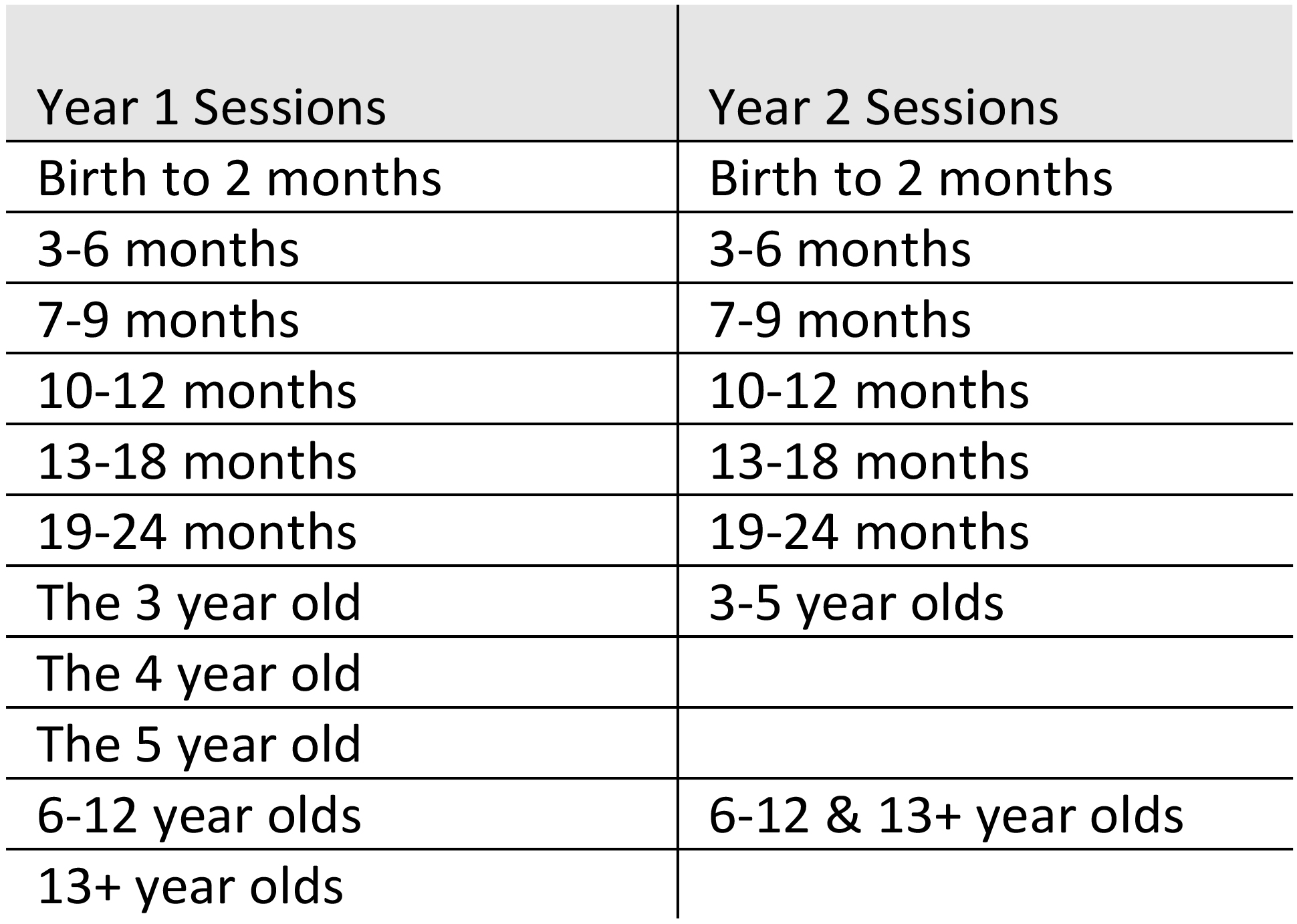
This curriculum employed a mixed methods approach to analysis including both quantitative and qualitative outcome measures including a novel survey, knowledge-based test, verbal feedback sessions, and the end-of-the-year program evaluation committee meeting. The novel survey included questions in the following categories: demographics, trainee exposure to developmental lectures, perceived knowledge, and interest level in developmental milestones. The knowledge based test included 10 multiple-choice questions from the Developmental and Behavioral Pediatrics Study Kit produced by the American Academy of Pediatrics [14]. The survey and test were given to trainees at the beginning and end of each academic year (the first and last sessions of this curriculum). Descriptive statistics were utilized. Means and standard deviations were calculated for quantitative data. T-tests were used to compare pre- and post-curriculum scores, and significance was set at
Results
During the first academic year after implementation, nine trainees attended various numbers of sessions (three pediatric rehab fellows, five triple board pediatric rehab residents). During the second academic year after implementation, eight trainees attended various numbers of sessions (four pediatric rehab fellows, four triple board pediatric rehab residents). A single pediatric rehabilitation faculty member was responsible for overseeing all sessions throughout both academic years. However, all pediatric rehabilitation faculty at our institution were made aware of curriculum implementation. For each session the participating trainees created a character/representation to help remember the covered developmental age (Fig. 2).
Developmental characters created by trainees. (a) 2 months (b) 9 months (c) 2 years.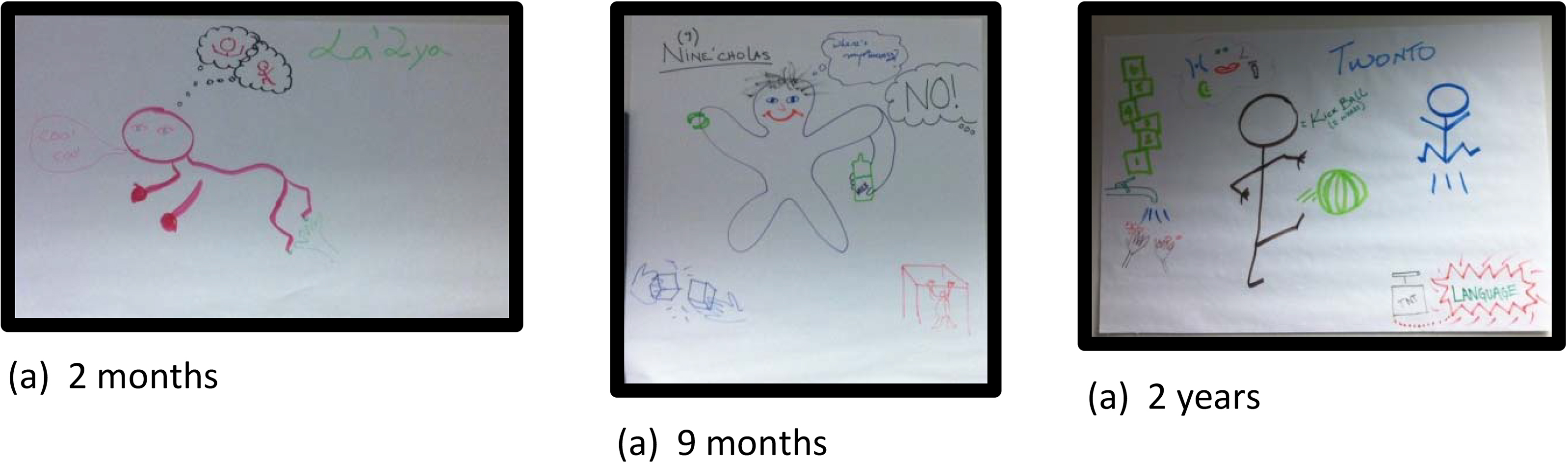
Outcome measures pre- and post- curriculum.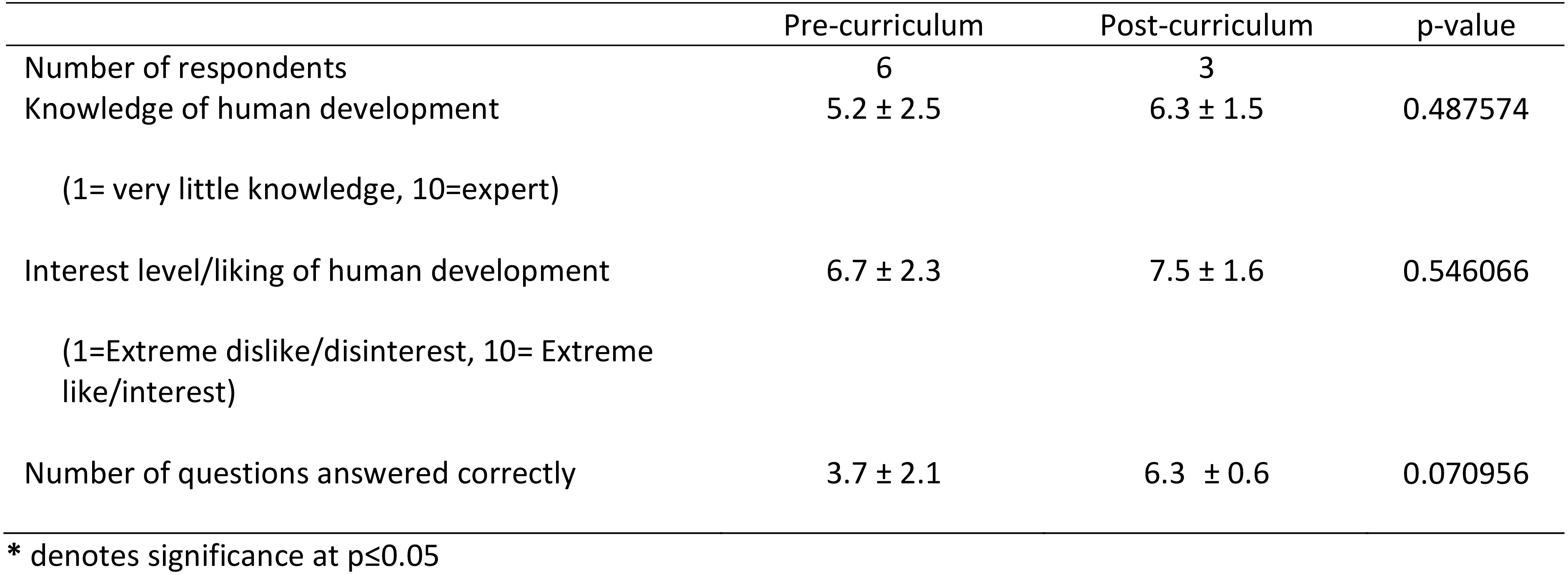
During qualitative feedback sessions held after the first year of implementation, PRM fellows voiced concerns regarding the ability to attend many of the lunchtime lectures due to clinics running over or inpatient meetings being scheduled. In response to this feedback, the time of the sessions was changed to follow pediatric rehab lectures (considered protected time for all pediatric rehabilitation trainees at our institution). At the conclusion of the second academic year of implementation, no pediatric rehab fellows voiced concerns regarding the ability to attend lectures without protection from other clinical activities. During the first year of implementation, pediatric rehabilitation residents similarly found it difficult to attend lunchtime lectures as they were often at a different off-site location for rotations. In the second year of implementation, pediatric rehabilitation residents did not voice concerns regarding ability to attend morning sessions while on physical medicine and rehabilitation (PM&R) or pediatric PM&R rotations, although they did have difficulties attending sessions while on inpatient pediatric months.
Both the scheduling and the number of sessions overall changed between year one and two. During the first year, twelve sessions occurred at the frequency of one time per month. Feedback after completion of the first year suggested that some sessions related to the older age groups could be combined without losing effectiveness (i.e. sessions related to preschool ages and beyond). Thus, the number of sessions was decreased to eight total (Fig. 1).
Responses related to child development on the annual PRM fellowship program survey were reviewed. The year prior to implementation one fellow strongly agreed and the other fellow strongly disagreed with the statement “The program facilitates competence in normal growth and development.” After the first year of implementation, two out of three fellows “strongly agreed” with the aforementioned statement and the remaining fellow chose “agree.” The second year after implementation 3 out of 4 fellows “agreed” that the program facilitates competence in normal growth and development and the other fellow chose “strongly agree”.
Pediatric rehabilitation residents also complete a program survey annually to evaluate the residency program. However questions regarding developmental milestone training were not asked until 2 years after implementation of the curriculum. They were asked whether they agreed or disagreed with the following statement: “The developmental curriculum is of high quality and value to my education”. On a scale from 1–4 with one being strongly disagree and four being strongly agree the weighted average was 3.5
Participation in developmental education sessions.
The novel survey and knowledge-based test as described previously were given to the trainees prior to the series beginning and at the completion of the first year. Six trainees completed the pre-test and three trainees completed the post-test. Over the course of the first year, ratings of perceived knowledge of developmental milestones, the number of structured educational sessions participated in related to development, and interest level increased (Figs 3 and 4), but no differences reached statistical significance.
Various curriculum models have been proposed over the last few decades in an effort to more effectively educate the adult learner within the realm of medical education. These include but are not limited to the flipped classroom [15], team based learning [16], and simulation based training [17]. When developing and initiating new curriculum, the medical educator must take into account the learners, goals of the curriculum, and resources when determining the most effective and appropriate strategies.
Medical students, residents and fellows in various fields are required to learn developmental milestones. While there are curricula utilizing various published structures and models that relate to this topic, to our knowledge, none use this type of novel approach that is tailored to the adult learner. Furthermore, there are no published curricula that target pediatric rehabilitation trainees.
We implemented our pilot curriculum at a single institution with a small group of pediatric rehabilitation trainees. However, it can be utilized at any stage in medical education to teach developmental milestones to learners at any stage in medical education, from medical students to fellows, and, as a curriculum teaching normal developmental milestones, can be used in other specialties. It could also be utilized in programs with smaller numbers of pediatric rehabilitation trainees. The sessions were purposely designed to be short in time and thus could be scheduled within didactic series of various structures without too much difficulty. As we found, implementing the curriculum may take a few reiterations to find the time that maximizes attendance, and this should be tailored to individual programs.
Initially, the main goal of developing this curriculum was to provide a more interactive way to learn developmental milestones. All too often, learners try to memorize milestones a few days before a test, and then quickly forget them. Learners then have difficulty applying knowledge to pediatric patients in the clinical setting. This curriculum is not based on solely memorizing but rather capitalizes on adult learning theory concepts to solidify knowledge gained. Trainees at our institution found that developing the drawing of the specific age child to be helpful. Anecdotally, greater than a year after drawing the initial child, trainees still remembered the name of the child and what they were doing in the picture. This is thought to be related to the sensory preference of the learner [13].
There are a number of potential factors contributing to the lack of statistically significant changes on our study measures. First, this was a pilot study with a small sample size, and not all participants completed post-outcome measures. There are also inherent difficulties with using Likert scales without specific anchor statements to measure trainee satisfaction/opinion. This difficulty potentially occurred in this study between the first and second years post-implementation when fewer trainees chose “strongly agree” that “The program facilitates competence in normal growth and development.” Following results over multiple years, matching trainees pre- and post-tests, and providing anchor statements for annual program evaluations/curriculum outcome measures have the potential ability to strengthen these inherent weaknesses of the pilot study. Also, the knowledge based outcome test was only ten questions. While this knowledge based test utilized well vetted AAP PREP questions, using only ten questions to assess overall knowledge of developmental milestones could certainly lead to inaccuracies, and thus this should looked at more closely as the curriculum continues.
Conclusion
We believe that this study introduces a novel approach augmenting education related to developmental milestones. The curriculum is tailored to the adult learner and is well-suited to pediatric rehabilitation trainees. Our pilot was with a small number of trainees, and we were able to demonstrate anecdotal success in achieving greater competence in the subject area, though statistically significant study measures were not demonstrated. Therefore, we believe this approach warrants further investigation.
The first main goal for future development of this curriculum is to develop/utilize more robust outcome measures to ensure that trainees are truly benefitting from the curriculum as discussed above (i.e. SAE scores, board exam scores, pediatrics inservice exam scores). The second is to incorporate clinical evaluations of typically developing children into the curriculum. This goal could be met by having trainees observe at a local day care center or in a general pediatrics clinic. This would be outside the scope of the current curriculum; however we believe that it would serve as one more way to solidify concepts, specifically for the more kinesthetic learner.
Footnotes
Acknowledgments
The author would like to acknowledge David Pruitt, MD for his support related to development of the curriculum and provision of protected educational time for the PRM fellows at our institution.
Conflict of interest
The author has no conflict of interest to report.