
Abstract
PURPOSE:
In children with cerebral palsy (CP), gastrocnemius muscle spasticity may lead to pes equinus posture which causes insufficient ankle joint dorsiflexion for normal gait. The aim of this study was to analyze the stiffness of gastrocnemius and tibialis anterior muscles by shear wave elastography (SWE) in children with pes equinus deformity due to spastic CP.
METHODS:
24 legs of 12 children (6 females and 6 males, mean age 45.8 months) with CP were prospectively included in the study. Tissue stiffness quantification with shear-wave velocity (SWV) was analyzed.
RESULTS:
The mean SWVs of the gastrocnemius and tibialis anterior muscles were 3.91±0.26 m/s and 2.67±0.18 m/s, respectively. The stiffness of the gastrocnemius muscle was significantly higher than the stiffness of the tibialis anterior muscle (p < 0.0001). There was no correlation between the stiffness of these muscles (r = 0.129, p > 0.05).
CONCLUSION:
Gastrocnemius muscles were stiffer than tibialis anterior muscles in patients with spastic CP. But stiffness between these muscles was not correlated with each other. Pes equinus may be related to stiff gastrocnemius in these patients. This study demonstrates the clinical potential for SWE as a non-invasive tool for analyzing calf muscle stiffness.
Introduction
Cerebral palsy (CP) is a group of disorders associated with the development problems of movement and posture caused by damage to the brain during either the prenatal, perinatal or postnatal periods [1]. Spasticity is one of the most common pathologies in patients with CP; gastrocnemius muscle spasticity may lead to pes equinus deformity which causes insufficient ankle joint dorsiflexion for normal gait. This deformity may result in lower extremity dysfunction such as joint contracture and locomotor inability, which subsequently negative affects functional abilities such as walking, transfers and activities of daily living (ADLs) [1].
Shear wave elastography (SWE) is an ultrasound-based technique and provides a quantitative measurement of tissue stiffness by producing “push pulses”. Basically, SWE depends on the displacement of tissues induced by a force, either external pressure or the radiation force from a focused ultrasound beam. The displacement of tissues induces elastic shear waves, which propagate and are detected by the ultrasound transducer. The velocity of the shear waves correlates with tissue elasticity; the stiffer the tissue, the faster the shear wave propagates. Shear wave velocity (SWV) can be expressed in meters per second (m/s) or in kilopascals using the Young modulus, depending on the different manufacturer types [1–3]. At present, in addition to point SWE technique, a two-dimensional SWE technique called virtual touch tissue imaging and quantification (VTIQ; Siemens Medical Solutions, Mountain View, CA, USA) has been applied and used in clinical practice. VTIQ is an acoustic radiation force impulse (ARFI)-generated quantitative technique. It is a two-dimensional shear wave speed measurement method in which the shear wave speed value can be named as SWV, and it is also expressed in m/s. In VTIQ, an ultrasound probe generates a low frequency longitudinal push pulse. The push pulse induces shear waves which travel perpendicular to the ultrasound beam. VTIQ measures the speed of the perpendicular shear waves by detection pulses. Because the speed of the shear waves propagating through the tissue is proportional to the stiffness of the tissue, a color coded map in the region of interest (ROI) gives information on the tissue stiffness. VTIQ can display color-coded images and measure localized SWV from 0.5 to 10 m/s using ARFI push and pulse beams [4]. VTIQ gives the ability to visualize quantifiable differences in tissue elasticity. This technology offers a high level of resolution and can assess and monitor lesions as small as 3 mm [5].
This tool has been recently used for the evaluation of musculoskeletal structures of patients with neurological disorders including Parkinson’s disease, stroke and CP [1, 6–10]. In the previous studies on this subject, the muscles in the spastic extremity were compared with the symmetrical muscles of the contralateral extremity that were intact or less affected. As a result, increased tissue stiffness of spastic muscles compared to the contralateral side was detected. In this study, the elasticity of the muscles that have antagonist functions in the spastic extremity was analyzed. Spasticity has already been detected in the gastrocnemius muscle in patients with spastic CP plus pes equinus deformity, but no spasticity has been observed in the tibialis anterior, which is the antagonist of this muscle. In addition, the gastrocnemius muscle appears to be shortened in the pes equinus posture compared to the normal posture. Similarly, the tibialis anterior muscle seems to be elongated in the pes equinus posture compared to the normal position. The spastic and shortened gastrocnemius muscle was evaluated by elastography, as were the non-spastic and more elongated tibialis anterior muscles that are all located in the same extremity. The aim of this study was to compare the stiffness of gastrocnemius and tibialis anterior muscles by SWE and assess the correlation between the stiffness of these muscles in children with pes equinus deformity due to spastic CP.
Materials and methods
This study was approved by the Baskent University Institutional Review Board and Ethics Committee (number of the project: KA 16/148) and supported by the Institutional Research Fund. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki. Written informed consent was obtained from each child’s parents. Power analysis during the biostatistical preliminary assessment indicated a study population of 24 lower limbs with 95% confidence interval (CI) level and 80% power. Power analysis was performed using mean values of “Transverse Measurement of Elasticity Ratio” variables according to the study by Kesikburun et al. [8].
This prospective study included 24 lower limbs of 12 children with spastic CP. The inclusion criteria were previous diagnosis of CP, a Modified Ashworth Scale (MAS) spasticity score of at least 2 in the gastrocnemius muscles, aged from 2 to 8 years, and observed pes equinus posture in physical examination [6, 11]. MAS is the most commonly used tool for measuring spasticity and includes these categories:
Ambulation level and functional status of all patients were categorized as Gross Motor Function Classification System (GMFCS) Level 3 [6]. The GMFCS was developed to provide a simple method for classifying children with CP aged 12 years or less on the basis of functional abilities and limitations. The GMFCS includes five levels; Level 3 is defined as “walks with assistive mobility devices; limitations on walking outdoors and in the community” [12, 13].
Exclusion criteria were as follows: the presence of lower extremity contracture, injection of botulinum toxin or neurolytic agents and serial casting after these injections within the last six months, previous history of serial casting or any interventional procedures including surgery or trauma to the lower limbs, or diagnosis of any other musculoskeletal or neurologic disorder except CP that affects lower limbs. Patients with “lower extremity stretching” in the active rehabilitation program were not included in the study because it may affect the stiffness and spasticity of the lower extremity muscles.
Elastography measurements
Both the conventional B-mode ultrasound (US) and SWE were performed using a US system (Acuson S2000; Siemens Medical Solutions, Mountain View, CA, USA) by a radiologist with 5 years of experience in musculoskeletal imaging. On B-mode images, the anatomic details of the muscles were identified, after which SWE was performed.
First, each participant was placed in a prone position to evaluate the gastrocnemius muscle while the knee and the ankle were in the neutral position. Then the tibialis anterior muscle was evaluated in the supine position while the knee and the ankle were in neutral position. Belly points of the medial part of the gastrocnemius and tibialis anterior muscles were preferred for the measurements. Tissue stiffness was quantitatively measured by VTIQ application.
The SWVs of the gastrocnemius and tibialis anterior muscles were measured by SWE on a longitudinal plane. A linear transducer that enabled scanning with a frequency ranging from 9 to 4 MHz was used [9, 10]. A 5x5 mm rectangular electronic box-shaped ROI was used for SWV measurements that was automatically provided by the system software.
The quality of the SWE maps was assessed by color-coded maps. The examination was repeated until high-quality data was collected and the best representative image was selected for SWV measurement. If the system displayed the SWV as non-numeric symbols (X.XX), the examination was repeated until numeric values were obtained. SWV values were displayed as m/s and the available range was 0–10 m/s for SWV (Fig. 1).
All images were evaluated using Synapse version 4.0 software (Fujifilm Medical Systems Inc., CT, USA).
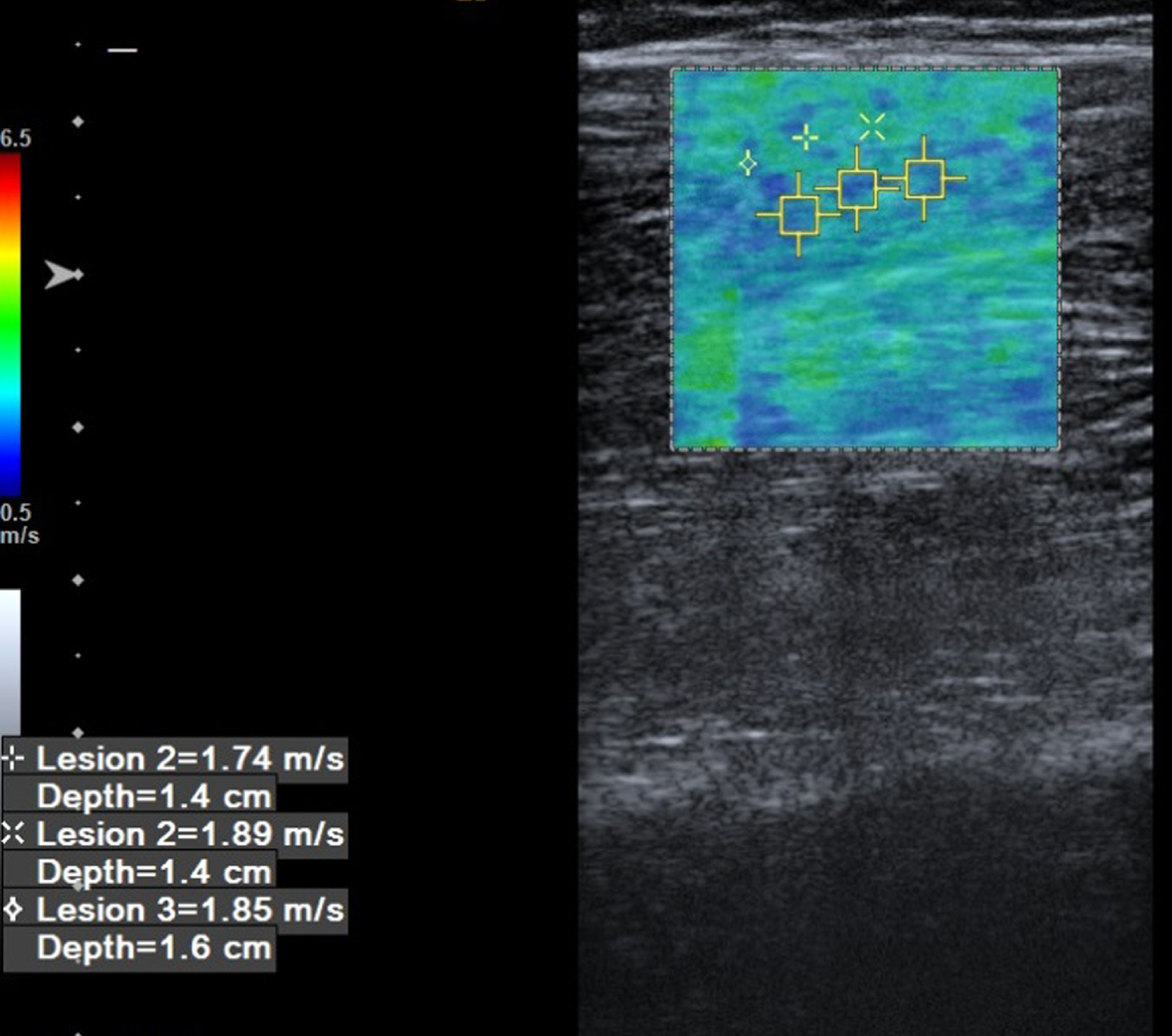
The Shear-Wave Velocity (SWV) of the gastrocnemius muscle was measured at the belly part of the muscle on the longitudinal plane. The lesion defines the different points that at the same muscle. The mean SWV was used for the analyses.
The SPSS 16.0 software package was used for statistical analysis (SPSS Inc., Chicago, IL, USA). The distribution pattern of the data was assessed by the Kolmogorov-Smirnov test. Comparisons between the stiffness of spastic gastrocnemius vs non-spastic tibialis anterior muscles were applied using a paired sample T-test. The correlation between the muscle stiffness values was assessed by an intraclass correlation test. The significance level was determined at p < 0.05.
Results
The mean age of the patients was 45.8±18.2 months (range: 2-8 years). Six of the patients were female and 6 were male. Clinical characteristics of the study population are summarized in Table 1.
Clinical characteristics of the study population
Clinical characteristics of the study population
The mean SWV of the tibialis anterior muscles was 2.67±0.18, 95% CI (2.60-2.75) m/s and the mean SWV of the gastrocnemius muscles was 3.91±0.26, 95% CI (3.81-4.02) m/s. The stiffness of the spastic gastrocnemius muscle was significantly higher than the stiffness of the non-spastic tibialis anterior muscle (p < 0.0001).
There was no correlation between the stiffness of the tibialis anterior and gastrocnemius muscles (r = 0.129, p = 0.539).
This study demonstrated no correlation between the SWV of spastic gastrocnemius muscles and non-spastic tibialis anterior muscles measured by SWE. This result revealed that the stiffness of the spastic gastrocnemius muscle was significantly higher than non-spastic tibialis anterior muscle stiffness in children with pes equinus posture in the ankle due to spastic CP. In these children, gastrocnemius muscle spasticity can lead to equinus posture, but their antagonist muscles, such as ankle and toe dorsiflexors, may have normal muscle tone. Equinus position may result in the elongation of the ankle dorsiflexors, including the tibialis anterior muscle. No correlation was found between the two muscles possibly because there may be factors other than spasticity affecting elasticity. There are multiple factors that may contribute to increased muscle shear wave speed in individuals with CP, including biomechanical components of spasticity, altered properties of passive structures of a muscle, collagen content of the muscle and the extracellular matrix [1, 14].
Lee et al. [7] compared the stiffness of calf muscles between less-affected limbs and more-affected limbs using SWE in patients with hemiplegic CP. They found that SWV was faster in both the medial gastrocnemius and tibialis anterior of the more-affected limb. Their results suggest that individuals with hemiplegic CP have altered muscle material properties, specifically greater stiffness, which can be quantified with SWE. In contrast to their study, the current study’s patient population consisted of patients in whom both lower extremities were similarly affected. In such patients, spasticity is evident in the gastrocnemius muscle while the tibialis anterior is not spastic. Lee et al. evaluated the same muscle of the contralateral extremities (i.e., right gastrocnemius and left gastrocnemius muscles, right tibialis anterior and left tibialis anterior muscles). In the current study, two separate muscles in the same extremity (i.e., right gastrocnemius and right tibialis anterior muscles) were evaluated.
Also, stiffness of the gastrocnemius and soleus muscles of individuals with CP has been reported to be stiffer than that of typically developing children [15]. In another study, Kwon et al. [6] compared the medial gastrocnemius muscle stiffness of 15 children with spastic CP with 13 children without neurologic and musculoskeletal disorders using real-time sonoelastography. Their results showed that gastrocnemius muscle stiffness increases in CP. Their study design was based on the comparison between spastic and healthy children. The current study aimed to analyze the calf muscle elasticity property in the same study population.
This study has some limitations. First, the other muscles that affect pes equinus posture such as the tibialis posterior and the lateral part of the gastrocnemius could not be evaluated. Also, the evaluation method was used while the children were in a static position. Spasticity and equinus posture have a dynamic component that has more affect than the static component in ADLs such as walking. Gastrocnemius and soleus muscles are functionally synergistic at the ankle during walking. Pes equinus posture seems to be related to soleus in addition to gastrocnemius muscles [16]. Dynamic evaluation of these children is very hard, and reliability may not be accurate. Only the medial part of the gastrocnemius muscle was evaluated in the static position. The gait patterns of these children can affect muscle stiffness. Although the tibialis anterior muscle was non-spastic, stiffness of this muscle may affect abnormal biomechanics of the lower extremity due to a spastic gait pattern. A single researcher did all the measurements, so interobserver variability could not be assessed. Abnormal biomechanics of other musculoskeletal structures of lower limbs could affect the calf muscle stiffness characteristics.
Conclusion
Pes equinus posture in children with spastic CP may be related to an increase in the stiffness of the gastrocnemius muscle. The ipsilateral gastrocnemius muscle was stiffer than the tibialis anterior muscle; however, the stiffness of these muscles was not correlated with each other in GMFCS Level 3 patients. This study demonstrates the clinical potential for SWE as a non-invasive tool for analyzing muscle structures in CP.
Footnotes
Acknowledgments
Ethics Committee Approval: The study was approved by the local ethical authority.
Conflict of interest
The authors have no conflict of interest or funding to report.