
Abstract
There is emerging evidence from patient-reported questionnaires that participation restrictions related to employment, parenting, and leisure pursuits emerge in adulthood after a brachial plexus birth injury (BPBI). However, little is known about the lived experiences of young adults with BPBI and their participation during this transitional phase. This Interpretive Description qualitative study was informed by the self-determination theory to guide our perspective of how transformations in the areas of autonomy, competency, and relatedness may influence participation throughout the lifespan. Semi-structured interviews with nine young adults between 19 and 34 years of age with BPBI’s were conducted, transcribed, and analyzed using thematic analysis to explore their lifelong participation. There were three main themes that arose during the analysis of these interviews: Navigating everyday life, Navigating uncertainties, and Navigating BPBI identity. Within navigating everyday life participants shared narratives of how opportunities in childhood helped them figure out how to adapt to their BPBI which led to habitual adaptations in adulthood; self-awareness and self-advocacy skills evolved over time. Common experiences of navigating uncertainties during major life transitions (e.g., parenting, post-secondary studies) was expressed as a conscious process of relearning and reintegrating the impacts of BPBI. During transition to adulthood, the lived experiences of the visibility and invisibility of disability emerged as a central aspect of BPBI identity. These narratives from the lifelong participation of adults with BPBI provide important insights to inform transitional care programming of children with BPBI within pediatric hand and upper limb clinical settings.
Keywords
Introduction
Brachial plexus injury is one of the most impactful peripheral nerve injuries, resulting in upper limb motor and sensory impairments that may lead to lifelong impacts on health-related quality of life. 1 Brachial Plexus Birth Injury (BPBI) occurs in neonates during birth and has an incidence of 0.38 to 1.56 per 1000 live births. 2 The most common pattern of injury after BPBI involves the upper plexus (C5, C6 ± C7), largely affecting shoulder and elbow function, while a total plexus injury (C5-C8 ±T1) affects functioning in the entire limb. 3 The physical impairments that occur in persistent muscle denervation after BPBI are muscle weakness, muscle imbalances, joint deformities, and joint contractures. 4 Total plexus injuries will also result in impairments in hand function. 5
The World Health Organization ICF (International Classification of Functioning Disability and Health) biopsychosocial model is highly accepted and adopted as a comprehensive model of functioning after BPBI.6,7 This model considers functioning through interactions between environmental and personal factors, and distinguishes an individual’s physical capacity (i.e., body function and structure), ability to execute tasks (i.e., activity), and engagement in life situations (i.e., participation). 6 Therefore, upper limb impairment after BPBI does not necessarily lead to participation restrictions. The latter is contextual and dependent on the individual’s life situation, contexts, and what matters most to them.
Being a birth-related condition, greater attention has been placed on understanding participation during childhood than adulthood. In childhood, difficulties with bimanual tasks such as eating with two hands, styling hair, doing up fasteners, and writing are cited to be more difficult compared to peers.8–10 Children and adolescents with total plexus injuries who have impairments in their hand are reported to experience more activity limitations.11,12 However, overall studies of these children indicate that they are independent in their daily activities and compensate for their upper limb impairments while engaging in sports and other leisure pursuits.8,10 Therefore, despite the severity of their injury and resultant activity limitations, participation restrictions in childhood are minimized due to enabling personal and contextual factors.
Personal and contextual factors change after childhood and there is emerging literature that participation restrictions emerge in adulthood.13–15 In 2018, Van der Holst et al. examined participation restrictions in adolescents and adults with BPBI using a standardized patient reported-outcome measure (PROM), the Utrecht Scale of Evaluation of Rehabilitation - Participation (USER-P). They found that overall health-related quality of life was good in this cohort; however, participation restrictions were reported in areas such as work performance, and educational and career choices. 13 Yau et al. explored the health related quality of life for adults with BPBI using the standardized PROM, EQ-5D-5 L questionnaire that focused on five different areas of measurement: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. 14 In comparison to the general population, the cohort of adults with BPBI had lower quality of life and associated impacts of surgery, employment status, disability benefits and marital status were found. Another study conducted by De Heer et al. explored the relationship between arm-hand function, pain, and daily functioning in adults with BPBI. Of the 27 participants in this study, 19 demonstrated that they experienced work-related complaints and limitations with their BPBI. Fifty percent reported moderate-severe pain and overall low to moderate associations were found between pain and daily functioning. 16 These studies illustrate a connection between the physical impairments and pain after BPBI with participation in adulthood.
Most recently, Dorich et al. surveyed 183 participants with BPBI between 21 and 87 years using social media. In their 2024 study, 79% of participants reported negative impacts on participation including aspects of their activities of daily living, sports, recreation, exercise, and general activity participation. Further, 76% of participants reported that their life roles were impacted specifically through parenting. Lastly, 73% of participants reported that self-esteem, relationships and appearance-related concerns had impacts on their overall quality of life. 15 Their study supports the need to explore the connection between the overall impacts of social roles, relations, and psychosocial factors and lifelong participation.
What the overall literature highlights is that participation restrictions emerge in adulthood related to life stage. However, little is known about the lived experiences during the transitional period to adulthood after BPBI. It is important to help bridge the gap and explore the physical, social, and psychological mechanisms and contextual factors that may influence participation restrictions. In this context, the self-determination theory (SDT) is helpful because the occupational profile and role of the individual changes through the lifespan as well as their contextual factors which may positively or negatively impact their participation outcome. 17 According to SDT, there are three psychological needs that motivate choice and engagement in activities promoting well-being: autonomy, competence, and relatedness. These areas are helpful in framing our understanding of how transformations occur that may influence lifelong participation.
Therefore, this qualitative study was informed by the SDT to guide our exploration of how transformations in the areas of autonomy, competency, and relatedness may influence participation throughout the lifespan in young adults with BPBI. The overarching goal of the research was to generate insights about this transition period to inform transitional care programming for children with BPBI and their families.
Methods
An Interpretive Description qualitative study was designed to gain rich information from narratives of adults with BPBI in the context of a clinical purpose. 18 A driving aim of this study is to gain information to further support rehabilitation and intervention planning from a client-centered perspective within this population’s childhood and adulthood healthcare services. Our methodology was informed by the SDT and a constructionism epistemological approach that encourages an understanding of how individuals interact with the world around them based on their cultural, social and historical experiences. 19
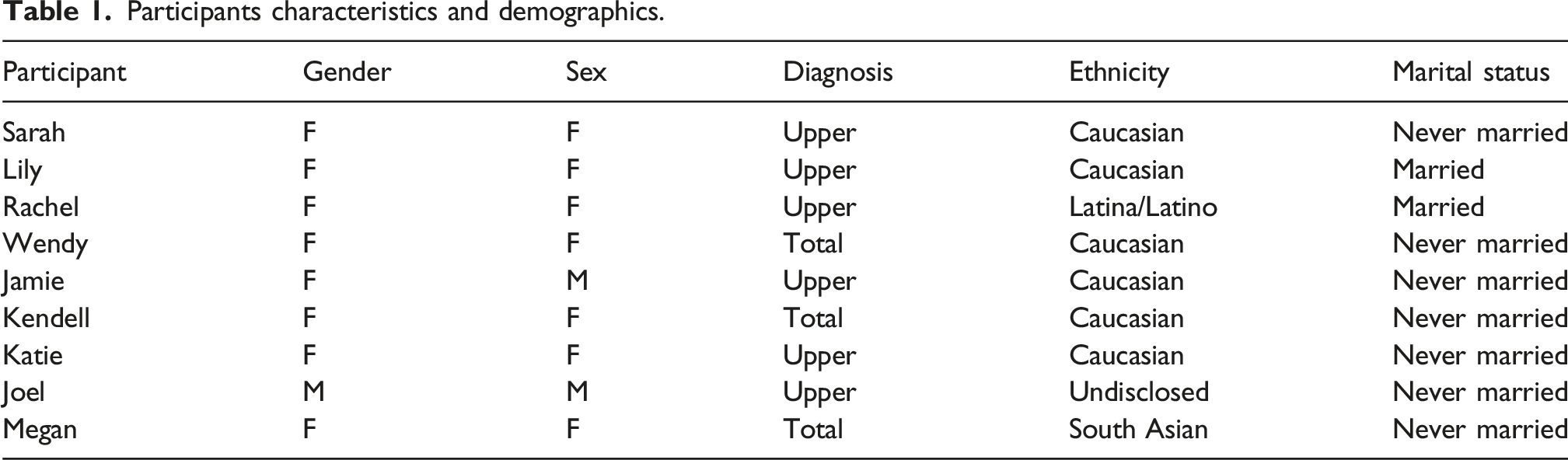
Participants characteristics and demographics.
Three trained interviewers [SR, LI, LD] used a predetermined semi-structured research guide composed of open-ended questions. Informed by the SDT, the interview questions were adapted from the Perceived Parental Autonomy Supporting Scale, the General Self-Efficacy Scale, and the Social Connectedness Scale-Revised.20–22 An interviewing approach that encouraged the collection of comprehensive and descriptive data was used and organized into four parts: (1) A warm-up question, (2) Current participation, (3) Childhood/adolescent factors, and 4) Transitional care. The interviews were conducted virtually on Microsoft Teams, audio recorded, and auto transcribed. 23 The accuracy of the transcriptions was verified by two independent researchers [SR, LI].
Data analysis was conducted through an Interpretive Description lens and procedurally followed the six steps recommended by Braun and Clarke to code and thematically analyze the transcribed interviews. 24 An interview transcript was independently coded by the three researchers [SR, LI, ESH] and collectively discussed. Following, a second interview was independently coded to ensure simultaneous coding of categories aligned well among all researchers. During this first iteration of coding, 37 different categories arose which were developed into a central codebook. Then, all interviews were analyzed in which 16 initial topics were generated by the research team, collectively defined, and refined into nine themes through consensus of the researchers [SR, LI, ESH]. Lastly, analysis of these nine themes with emphasis on their meanings, their relationships to each other, and the overall narrative of the dataset, resulted in narrowing down to three main themes and subthemes. Reflective journaling and an audit trail are available to show a clear explanation of the data collection and analysis processes used to produce the findings. 25
Results
The three main themes that arose from the nine interviews about transitioning to adulthood after BPBI were: Navigating everyday life, Navigating uncertainties and Navigating BPBI identity. Themes are discussed below alongside quotes represented in italicized text and denoted with pseudonyms (Table 1).
Navigating everyday life
Among the participants interviewed, their competency in choosing and engaging in daily activities was communicated through evolving stories surrounding self-awareness of the need to adapt and advocate for their needs. Consistently conveyed through participant interviews was a resolve to not let physical limitations be a barrier to participation. Participants described that they did not allow their upper limb impairments stop them from trying new activities such as joining a team or getting a job. It was important that they figured out what modifications worked best for them, tried alternative ways than the stereotypical normal method, and worked hard to prove to themselves that they could do something even if they didn’t enjoy the activity.
For some, this resolve and willingness to try all activities was expressed alongside important moments of self-discovery during childhood about how their physical limitations led to participation restrictions. In her interview, Katie expressed the desire to be in control of the choice to participate in gymnastics. Yet, she accepted the situation in which her physical impairments and lack of accommodations resulted in being cut from the gymnastics team despite her strong interest in the activity: “I try whatever I want and decide for myself whether or not it’s something I could do, or something I was interested in...The gymnastics team, I totally understand, I could do maybe a front roll and that was about it, but I think I was in grade five or six at this time, so it would have been nice to be involved somehow even be the teacher’s assistant, or something just because all of my friends were on the team and it was something that I was really interested in, so it would have been nice to have some sort of involvement with it, and even if I couldn't be competing like just be able to even come watch the practices or try things.”
Parents also played a key role in providing opportunities, support, and freedom to explore different activities. These important opportunities were embedded alongside stories of advocacy, indicating that they influenced the development of self-awareness of physical capabilities and interests. In the following interviews, Megan describes how her parents supported her to try different activities: “They gave me the freedom for it, they didn't give any limits, they were fine with me trying anything if I wanted to because even with the whole sports and stuff, the only thing I have done is dancing and swimming; but for the dance one it was like, ‘Oh, they heard, it’s good. Do you want to try?' And I was like, ‘sure;' same thing for swimming.”
Similarly, Wendy’s childhood experience illustrated how her parents supported her to pursue any activity of interest; however her journey was described as a process of trying an activity, learning through trial and error, and moving on due to lack of progress in her physical skills. In her situation, the open invitation to pursue any activity may not have been the right approach. “...at home was just like, obviously you can do whatever you want to do. But my ability to do whatever I decided, I wanted to do was never in question... when I wanted to do swimming lessons they put me in some lessons. When I wanted to do gymnastics they would put me in. I wanted to learn rock climbing - I was learning rock climbing; and it was only after I was in gymnastics for a year and I was not making any progress, and I was feeling very frustrated that my mom was like, ‘Do you think maybe you'd rather do something that your arm would not get in the way of?'”
Therefore, parental support alongside messaging that validated their child’s limb difference was important. Sarah appreciated that her parents were supportive of her but never stated that she could do anything she set her mind to. She explained why she felt it was important that her parents coached her to acknowledge her upper limb difference: “It's not acknowledging the disability... in turn, I believe these children are going to get less support and less accommodations given to them, and they're going to have a harder time coping when they realize that they are disabled.”
Her perspective is substantiated by Katie who recalled that her parents would tell her she could do anything. Looking back, she felt that it set her up for disappointment, “So, it was kind of times that, where I was, I guess, defeated because, growing up my parents... were 'you can do anything' but then there really is stuff that I can't do and, I understand that now, but growing up, it was kind of like upsetting to see”
By adulthood, participants’ interests were more established and they were more accustomed to their abilities. Often, they expressed that less attention was paid to the ways they were adapting until someone noticed or a resource was introduced such as a device or adaptive aid to make the activity easier. Katie and Kendell shared: “As I got older, and I’ve like stuck to things that I’m familiar with now. There's not really a whole lot of new things that I’m interested in that I would try now.” “I am very used to living with my disability, so I do find ways and have found ways to do things in my day-to-day life that for me are normal.”
The introduction of new resources such as a cordless vacuum or motion-detected soap dispensers were helpful in alleviating pain or muscle fatigue in their affected upper limb or increasing their efficiency in completing an activity. Megan explained that having a cordless vacuum was easier on her body which allowed her to participate in vacuuming more often: “I got one of the wireless Dyson vacuums because I had just a cheap cord vacuum, and I was not vacuuming just so I didn’t have to coil the cord after.” Yet, implementing these resources often required effort to plan or costs to consider.
Lastly, the evolution of self-advocacy skills was heard among the shared narratives regarding the physical adaptations required to navigate everyday life. During childhood, participants reported a tendency to lean on family members, peers, teachers, and coaches to advocate for their needs, while they described being more equipped and ready to speak up for themselves as adults. Katie illustrated how she relied on others to advocate for them during childhood: “Because I was so young my mom would advocate for me a lot more than I would.” She went on to talk about how having someone with her who knows her, to help advocate, was a source of comfort: “If I’m ever trying something new, I definitely don't do it alone, I will find a friend that knows me and what happened. To do it with just because even now I’m really bad at advocating for myself.”
She further shared how her dance teacher was instrumental in her continual participation in dance because of the safe and supportive environment she fostered: “My dance teacher was a big part of my life; I had dance with her since I was three years old. Even as I was getting older, I wasn't really interested in dancing anymore, but I stuck with it because she made me feel comfortable and she kind of understood me so there was a sense of comfort there. Whereas, if I went to try something new, I would have to explain, and they would have to learn all over again. So, my dance teacher was a big part of me staying active and kind of getting involved.”
Transitioning out of these childhood experiences, participants learned to advocate for themselves in adulthood through expressing their abilities, asking for help, and requesting adaptations and accommodation. Being able to advocate and feeling comfortable to do so reflected them feeling understood by their peers and those in their life. In contrast to her childhood experiences, Katie describes how she self-advocates for her needs after joining a new team and job. “But if I did go I would definitely, before I even did anything talk to whoever was in charge, whether it was a coach or the manager or something, and talk to them about [BPBI limb impairment] and just let them know before I even do anything.”
Similarly, Megan explains how she became accustomed to asking for help on the job if the demands were too much. “But I have also learned, for example, with the Co-Op job, if there were limitations in my motion and stuff, I did get used to asking for help if it's too much to do, if I won't be able to finish in the time that’s given.”
Navigating uncertainties
Collectively among participants, navigating uncertainties of lifelong participation was expressed as feeling unprepared and unsure of their physical abilities while embarking on novel situations related to life transitions. Insecurities arose from doubts about their overall competency to achieve the tasks required at the next life stage such as parenthood and post-secondary studies. These life transitions were described as periods of conscious relearning and reintegrating their BPBI into daily life. As Wendy shared, “I have this theory that every time I move into a new phase of life, I need to reintegrate my disability with it.” “You don't every time you want to learn a new skill you don’t just have to learn the skill, you also have to learn how it's going to work for you and by nature, you are just stumbling along because there’s ... you know, figure it out yourself. And then you get there, and you look back and you don't know how that happened. But here we are chopping potatoes; we now have chopped potatoes. I still couldn’t tell you how I do it, but I do it; there's definitely potatoes in my meals a lot.”
Two participants shared narratives about their experiences regarding the emotional and physical impacts BPBI had on caring for their child. They did not receive a great deal of support in terms of how to navigate parenting and it brought on challenges related to pain and insecurities surrounding holding and caring for their babies. Lily summarizes: “So, parenthood has been quite the eye opener for me, ‘cause my whole life, I’ve kind of just adapted and adjusted and I haven’t really had new things that I’ve had to try. So parenthood was terrifying for me because I didn't know how I was going to hold baby, feed baby, take care of baby.”
As new moms, Rachel and Lily talked about their concerns that muscle weakness in their affected limb, pain, and numbness, symptoms related to their BPBI are safety concerns while caring for their baby. The impacts of these concerns infiltrated routine daily tasks such as holding their babe, feeding, and changing a diaper. As their children grew during infancy and toddlerhood, it became more difficult to pick-up their children without pain, discomfort, or worry that they could not safely carry their child. Rachel and Lily explained: “Because of either pain or something sometimes my hand would go numb if I held her [daughter] for too long or I didn't have the strength in that arm to hold her but I couldn’t hold her in my right arm and do things with my left arm cause that arm doesn't work as well, and so I had to find places for her, put her in a carrier, all of that stuff.”
“I was super scared because I was like, how I’m going to hold him, or what if he falls from my arms or something like that. But, everyone always helps me and my mom was there; teaching me how to hold him and all that, and it was really easy. I couldn't like hold him a lot when he was growing up because of the pains and that he was heavy. He is heavy. He's big, so I’m still working with that because he still wants to be carried sometime but I can't.”
The other major transition that created uncertainties surrounded career choice and entering post-secondary studies. This transition was described as a difficult time with navigating school schedules, expectations, and advocating for accommodations on their own. Being away from home, some participants had to learn to advocate for their needs because their parents were not there to do so. Katie shared, “I kind of got to school and it was a little bit of a shock if I didn't tell anyone that no one knew, because my mom wasn't calling the school and letting them know for me.” On the other hand, Sarah's parents helped advocate for her accommodations within post-secondary education; however, she had to learn to navigate a whole new system of supports: “My parents are very adamant to get me in with what my schools health and wellness and accessibility services and so yeah, I have a case worker and it's just like an accessibility consultant, and I meet with her, and each time I need to update my LOA, my letter of accommodation, and they try to find what would work to help compensate for my problems.”
After completing post-secondary education, Megan expressed feeling nervous to apply to graduate school because of insecurities that her BPBI limitations would impact her ability to fulfill program requirements. As she had an interest in working in the pharmaceutical field, she was concerned about the precision required of both her hands to perform laboratory work. Her narrative demonstrates that insecurities related to BPBI limitations can have an impact on post-secondary school programs of study and career choices. The following are Megan’s words in relation to her struggle with the decision to apply for graduate school, “So, my Co-Op was a surprising experience for me because it was in the research lab for a pharmaceutical company. So, I was always worried if I would be good with lab-related work cause it’s very like hands-on and like fine motor skills.” I was also debating if I even should apply for Master's because I was worried about if I would be able to do everything that would be required to in the lab. It's more I had doubts that would I do well, even with the Masters, I wasn't sure if I'd do well in the lab setting or would I be good enough to be to get accepted into the program.”
Navigating BPBI identity
Navigating their BPBI identity was collectively discussed among interviews in relation to how the visible versus invisible disability infiltrated their daily interactions and who they saw themselves to be. Appearance-related concerns arose from the visibility of BPBI and being recognized as being different. Yet, BPBI was also described as an invisible disability, lacking representation on disability forms or unrecognized in situations when accommodations were needed. The dilemma of the visibility/invisibility of BPBI appeared to manifest during childhood related to the development of self-image and self-esteem. As adolescents, participants shared about their struggles with the way they looked in pictures and how they tried to cover up their BPBI with the clothes. Sarah and Joel shared: “I hated how my arm looks. I would see pictures of myself like in full body pictures in a group, and I would hate the way my contracture looked, because it was like immediately the first thing I noticed. Even now, I still do make an effort if I’m going to have a picture with somebody, I will put them on my left side so I can kind of hide my arm.” “I always used to love wearing sweaters and jackets that cover up the arm difference. That was my big thing like wear bulky... always wear a sweater or jacket...at least make me feel like I was covering up the difference.”
Jamie shared that hiding their BPBI was habitual, and they had learned to hide their upper limb difference so well that their BPBI could go unnoticed: “When moving and I naturally tend to put my arms or have hands in pockets and things; I'm naturally hiding. Because I don’t intend to do that, but that's how I’ve learned to do it so,..I always find this with people sometimes I tell someone that I have a disability and they go oh I would have never noticed.”
Keeping their BPBI hidden allowed Jamie to be in control of when their BPBI was disclosed to strangers. The readiness to disclose one’s BPBI was also expressed by Sarah who spoke of how she dated her boyfriend online for 9 months before she even met him in-person. Whether it may be disclosing their BPBI diagnosis through the visibility of their limb difference or conversation, Sarah explains that navigating this process is ongoing. BPBI is part of her identity and fundamental to who she is, and a central part of being understood by her partner: “There’s a lot of complexity in there that I think people wouldn't think about. I think there’s a general that your partner is supposed to always be supportive, but he has his own biases in his own upbringing that are affecting the way he thinks and the place he’s from, and what he’s known all his life. I think it is hard when you're dating somebody able bodied, and they don't understand disability.”
Other participants had negative encounters when their BPBI was pointed out to others when their appearance or physical capacity made them stand out as being different. Katie and Kendell shared, “I don’t like to make it known that I have a disability and it’s times where it gets pointed out that I do still have certain things that I can’t do.” “Recently I when I type on a computer, I type one handed - it's a lot quicker for me; it's the best for me and someone at my workplace pointed that out. She didn't mean anything bad about it, she was just, ‘Oh, you type with one hand and things like that...' Especially growing up, if someone was to point something out like that, it made me and still makes me uncomfortable.”
These narratives described situations in which participants did not want their BPBI disability to be known; however, they also faced with situations in which they wanted their BPBI to be known to receive appropriate support. Jamie contrasted their experience from early childhood when they also had a speech impediment to their lived experience of navigating BPBI as an adult without any other visible disability: “I was more visibly disabled as a child, because the minute you add that speech impediment other people are reacting to me as if I were ... reacting to me with the idea of, I was disabled, and that was my identity label quite clearly thrust upon me. Whereas now in adulthood I’ve gone into a more invisible version of disability. It was very strange, the whole visual versus invisible disabilities, a very frustrating dichotomy, because- I’m like, where's the middle option.”
Having an overt disability was seen to be helpful when advocating for accommodations associated with education and employment settings. The narrative shared by Sarah illustrates how the need for accommodations may not always be a formal request or process; the need may spontaneously arise in public spaces. In these social situations, the invisibility of BPBI can make it difficult to navigate these social situations: “I’ve learned that in order to get the accommodations I need, or just sort of the behavior I need around me when I’m out in public sometimes; I do have to make my disability visible, and that was a hard one for me... Because sometimes I do use a sling, but I don't always use a sling. When we were in Disney World and there is the bus between the parks and the hotels, and everybody immediately gets in; taking up all the seats. So, you’re standing, you get on the bus, and then the next people get on the bus. There was no like picking your seat, and the first time I tried it, I realized, I can’t properly hold onto the straps overhead, and it was dangerous. I was going to fall on somebody, and I needed a seat. I needed a seat on the bus and I’m starting to panic, and I realized that when I had my sling on immediately, it was, ‘Oh, there’s one of the disabled seats available for me,' because people can see and they will say, ‘Oh, okay, she’s got something going on.’ Whereas if I had just gone and sat in the seat, they would have thought I was just taking it because I was lazy.”
For some participants, pain emerged in adulthood that added to the invisible disability associated with BPBI. Jamie shared “In childhood, I don’t recall having as much pain, with it, which I gather, is a common saying of the pain - gets worse during puberty and then adulthood.” Experiences of pain after strenuous physical work, stiffness, and chronic pain were represented in the narratives around participating in day-to-day activities. Kendell and Sarah explained “For me, my pain is not easily tracked like that, because right now I’m in little to no pain. On like a daily basis. I would say I’m in little to no pain unless I’m doing something that's like strenuous where I’ve done too much, and I know my limits, so I don't even allow myself to get to those points, unless I really have to, I don't strain my body... I’m also kind of at a point in my life now where I’m actually feeling more pain in my right side, which is my non brachial plexus side.” “I definitely do get pain like, more neck and back... I would say actually - I don't have loads of pain down the arm, except for those electric shock type things, or just stiffness, because of my contracture.”
Living with chronic pain associated with BPBI, Sarah’s narratives around pain stands out among the other interviews and highlights how pain is a part of their identity and everyday activities. “I have fairly bad constant pain, that is definitely a huge mark on my daily life. Especially from the moment I wake up having slept for no matter how many hours, whether it was just up to 3, whether it’s up for 12, there’s pain associated with that so as soon as I wake up.”
Discussion
Lifelong participation from childhood to adulthood after BPBI involves successful adaptions to daily activities while navigating through uncertainties during life transitions and ongoing challenges with BPBI identity. Our study contributes to a developing understanding of adaptation in individuals with BPBI as they are confronted with increasing complexity of activities of daily living and occupational roles in their transition into adulthood. Further, where mere adaptation of existing skills is insufficient to meet the occupational demands of adulthood, we describe the recruitment of new skills, namely self-advocacy skills, and remodeling of one’s identify around evolving self-concept in relation to their BPBI. Self-advocacy and reintegration of BPBI are especially needed to navigate major life transitions such as parenting and post-secondary education. The narrative process, specifically, inviting this kind of discourse directly from those with lived experience is important to the meaningful development of BPBI literature. This is especially the case with this topic of visibility, as often, the physical aspects of BPBI are visible and the psychosocial elements of self and identity are ‘invisible' in BPBI research. Narratives of both participants’ adaptability through life transitions and navigation of the visibility and invisibility of their impairments lends insight to the outcomes of this study; particularly, in reflecting upon the meaning of the participation restrictions reported in the literature by adults with BPBI.13–15
In our study, the SDT constructs of autonomy, competence, and relatedness were used to contextualize the interviews and frame our understanding of how transformations occur in lifelong participation. Within this context, our findings align with Bergman et al., who found that higher self-determination behaviours were found in adolescents with BPBI at home compared to school and community environments. 26 Reflecting back, our participants expressed how their parents were instrumental in providing opportunities that fostered their willingness to try different activities. However, adopting a ‘you can do anything' approach without acknowledging physical differences may have created more difficulties with learning to advocate for their needs outside the home. This may be reflective of the underlying development of occupational awareness, the alignment between upper limb capacity and demands, as an influential factor in the child’s performance and adaptability.
Despite competency in navigating everyday activities, the narratives from the qualitative data generated insights regarding the challenges of transitioning to post-secondary education, making career choices, dating, and parenting. In a practical manner, these narratives can inform transitional care programming for children with BPBI and their families. At present, health services for individuals with BPBI are primarily delivered in tertiary care pediatric centres. These children and families are followed for medical and rehabilitation care until 18 years of age with specialized care related to reconstructive surgery and rehabilitation. 27 Ultimately, the goal of care in childhood is to foster meaningful participation within each child and family’s life context. 28 Yet, little is known about how pediatric care relates to lifelong participation after graduating from such programs. The narratives of this research begins to illuminate and identify key transitional areas that need to be addressed in transitional programming for these families.
Lastly, the visibility/invisibility dilemma that arose from these interview data suggests that upper limb impairment after BPBI may be experienced paradoxically. Described in these qualitative data is the desire to belong among friends, co-workers, and society without being seen or set apart as being different. Yet, in times of need, the lack of visibility of BPBI was seen as a hinderance to receiving needed support. These experiences relate to the SDT concept of relatedness and developing one’s own BPBI identity. The ability to live in both worlds where BPBI was seen and unseen seemed to create two identities that lived in conflict of each other. An in-depth exploration of this paradox is needed to better understand the intersection of BPBI identity and the social factors contributing to participation. Further, as children and adolescents may not readily express awareness of their sense of belonging in different social situations, learning from the narratives of adults with BPBI is important. These lived experiences can help families recognize and navigate the visible/invisible aspects of BPBI and its meaning in their life context and stage.
Our study presented strengths around being able to engage in in-depth semi-structured interviews that allowed for a rich, narrative story of each participant and their lived experiences in relation to lifelong participation with their BPBI. We gathered participants and recruited from diverse geographic locations to gain a greater holistic approach of BPBI and how it can look different depending on resources and location. Through engaging in these interviews, it allowed for a comprehensive understanding of the participants’ lives in a variety of different areas (childhood, youth, adulthood). Our study also encompassed a broad age range of participants, in different life stages and occupations, that highlighted different aspects of their narratives creating insights into different areas.
Potential limitations of this research study are that despite having a predetermined interview guide, there was variation in the interview style between participants and how different topics were explored deeper with some participants. This study also had a limited number of male participants, with only two out of the nine being male. It is possible that having more male representation could have added further depth to our results.
Conclusion
This qualitative study builds on the emerging literature on outcomes of adults with BPBI in elucidating the lived experiences and perspectives of lifelong participation. The findings from interview narratives indicate that adaptation to BPBI impairments are developed in childhood that continue into adulthood; however, there is a need to develop self-advocacy skills and reintegrate BPBI during major life transitions. The insights gained from this study can help inform children with BPBI and their families about the uncertainties faced when transitioning to post-secondary education, employment, and parenthood. These transitions also journey with ongoing process of working through physical insecurities, learning to self-advocate, and developing one’s own BPBI identity. This research generated rich narratives regarding the lived experiences of adults with BPBI and highlights that more research is needed to understand the lifelong impacts of BPBI to inform transitional care programming for children with BPBI and their families.
Footnotes
Ethical approval
This study was approved by the Hospital for Sick Children Research Ethics Board (Approval #79834) and Administrative approval through the University of Toronto Research Ethics Board as a graduate student project (Approval #42161).
Author Contributions
Shelby Rabb: conceptualization, methodology, formal analysis, writing – original draft, reviewing and editing; Laura Ireland: conceptualization, methodology, formal analysis, writing – original draft, reviewing and editing; Lexi Davidson: conceptualization, methodology; Emily S. Ho: project administration, conceptualization, methodology, formal analysis, resources, supervision, writing – original draft, review and editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from the American Hand Therapy Foundation, Burkhalter New Investigator Grant and the University of Toronto Connaught New Researcher Award.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.