
Abstract
PURPOSE:
Assessing provider adherence to preventative sexual and reproductive healthcare guidelines in adolescents and young adults (AYA) patients with physical and intellectual disabilities (PWD).
METHODS:
Records of PWD (
RESULTS:
The mean age of both groups was 17.3 years
CONCLUSIONS:
Adherence to sexual health guidelines was suboptimal, and lower among PWD. Vaccination rates did not differ between the two groups.
Keywords
Introduction
The United Nations Convention on the Rights of Persons with Disabilities defines disability as “long-term physical, mental, intellectual or sensory impairments which in interaction with various barriers may hinder [the] full and effective participation in society on an equal basis with others” [1]. The World Health Organization notes that 10% of the world’s population has a disability [2], with estimates of approximately 6–23% of the United States having any type of disability, including mild, moderate, and severe disabilities [3, 4, 5, 6]. The reproductive healthcare needs of people with physical and intellectual disabilities are largely unmet and understudied [2, 6, 7, 8, 9, 10]. In 2006, the United Nations General Assembly adopted the Convention on the Rights of Persons with Disabilities (CRPD) which addresses the human rights of people with disabilities and strategies to ensure that those rights are upheld. Within this document, there are several provisions related to the reproductive health needs of this population, including the right to protection from sexual and gender-based violence, the right to equal access of healthcare, and the right to freedom from discrimination “in all matters of family planning, fertility, and family life” [2, 11]. The United States has not ratified this convention, making it one of few countries that is not legally bound by this document [1].
It is reflective of the United States’ non-ratification of the CRPD that Americans with disabilities receive suboptimal health care [1, 2, 6, 7, 8, 12, 13, 14, 15]. In particular, the sexual and reproductive health (SRH) of people with disabilities is largely overlooked [1, 2], despite the markedly increased risk of sexual assault and exploitation present for those with physical and intellectual disabilities [3, 9, 12] along with the increased risk of acquiring sexually transmitted infection in sexually active adolescents with intellectual disability [8, 16]. Perinatal care and prenatal counseling are also frequently inadequate for women with disabilities [7, 17] despite the fact that women with most types of disability become pregnant at the same rate as women without disability [18, 19]. There are many possible reasons for this health discrepancy: many people with physical disabilities note that their physicians’ offices lack appropriate equipment to accommodate their physical needs during genital exams [7, 15], and many people with both intellectual and physical disabilities simply are not offered comprehensive reproductive healthcare due to the incorrect belief that this population lacks sexual impulses and desires [2, 20, 21].
Current recommendations regarding SRH from the United States Preventive Services Task Force (USPSTF), American Academy of Pediatrics (AAP), American College of Obstetricians and Gynecologists (ACOG), and the Centers for Disease Control and Prevention (CDC) do not exclude individuals based on the presence or absence of disability (Table 1). These guidelines note instead that the most important risk factors are age, multiple sex partners, and inconsistent condom use [6, 22, 23, 24, 25, 26, 27]. Because people with disabilities should be free from discrimination “in all matters of family planning,” this population should ideally be in receipt of SRH in line with these recommendations as a matter of health equity, although we hypothesize that they are not.
There is a paucity of literature about the SRH of adults with multiple medical conditions and disabilities, and even less for the adolescent and young adult (AYA) population. The majority of available studies do not include males and consist of survey-based, retrospective analyses [6, 28] which are prone to recall bias and exclude patients whose disabilities preclude them from completing a survey. These studies reveal that women with disabilities report that they are less likely to receive Papanicolaou (pap) smears than those without disabilities [22]. Other research has found that women with disabilities state that they are less likely to receive contraceptive counseling, sexually transmitted infection (STI) counseling, and routine access to gynecologic care. With regard to STI screening, findings are less uniform, with some studies demonstrating decreased screening rates and others showing equivalent screening rates in the disabled as compared to populations without disability [7, 15, 16].
Research regarding healthcare provider practices concerning SRH for disabled populations is limited. Available studies do not focus on provider practices, but rather on patients’ experiences and perceptions. While these studies are valuable, they do not define what kind of care a provider intends to offer, or confirm if the care offered to people with disabilities is substantially different from that offered to those without disabilities. As such, the objective of the current study was to assess provider adherence to preventative SRH guidelines in AYA with disabilities.
Methods
This study is a matched cohort design comparing AYA with multiple medical conditions to those without these conditions, with matching based on age and sex to examine the outcome of provider adherence with reproductive health screenings [29]. We conducted a retrospective chart review of AYA receiving routine preventative care in a clinic that provides a medical home for children and adults with complex neurodevelopmental conditions (People With Disabilities, PWD) from January 1, 2011 to December 31, 2016. PWD were matched by age and sex to patients seeking routine preventative care at an internal medicine-pediatrics clinic within the same institution in the same time interval (Comparison Cohort, CC). Matching was completed using the proc-sql function of SAS Enterprise Guide version 7.1 (Cary, NC, USA). All visits in each of the two clinics conducted during the study period were eligible for inclusion. If a patient had multiple visits to the clinic during the study period, each visit was eligible for inclusion as a separate data point. Patients who are currently deceased but had visited either clinic during the study period were eligible for inclusion. For CC only, the presence of a documented intellectual or physical disability was the exclusionary criterion. Prior to data collection, the study protocol was approved by the Institutional Review Board of the participating institution.
PWD and CC were identified in the medical record (Epic, Verona, WI, USA) by CPT
Reproductive health guidelines
Reproductive health guidelines
Medical records for PWD and CC were reviewed to determine provider adherence to the following SRH guidelines as indicated (Table 1): (1) initiation and completion of human papilloma virus (HPV) vaccination series within the study period [22, 23], (2) initiation and booster for meningococcal vaccination [30], (3) screening for human immunodeficiency virus (HIV) within six months before or after the date of the preventative healthcare visit [25], and (4) sexual [24], (5) menstrual [27], and (6) pregnancy history documentation on the day of the preventative healthcare visit. Screening for N. gonorrhoeae (GC) and C. trachomatis (CT) within six months before or after the date of the preventative healthcare visit [24] and receipt of pap smear within six months before or after the date of the preventative healthcare visit with a minimum age of 21 [31] were also noted.
Six-month windows before and after the date of the primary care appointment were chosen to reflect the possibility that a patient may have had their screens performed in a non-primary care setting, such as an urgent care visit or gynecologist appointment. Such testing, if visible to the primary care provider, may result in non-screening during the index encounter that is still in compliance with the guidelines in question.
With respect to HIV screening in particular, the USPTF specifies that “The evidence is insufficient to determine optimum time intervals for HIV screening. One reasonable approach would be one-time screening of adolescent and adult patients to identify persons who are already HIV-positive, with repeated screening of those who are known to be at risk for HIV infection, those who are actively engaged in risky behaviors, and those who live or receive medical care in a high-prevalence setting.” As many providers combine STI screening in general with HIV screening, the same six month window was used for HIV screening as for STI screening.
Within menstrual history, three elements were explored: documentation of the first date of last menstrual period (LMP), recording of menstrual regularity or pattern, and notation of any menstrual history other than LMP or regularity (e.g., heaviness of flow, pain). If a screening measure was offered or ordered by the provider but declined or not completed by the patient, this was recorded as positive provider adherence. Meningococcal vaccine initiation and booster rates during the study period were included as a non-SRH control measure of physician guideline adherence [30].
Characteristics of patients with disabilities (cases) and nondisabled age- and sex-matched peers (controls)
Adherence to sexual and reproductive health (SRH) guidelines among patients with disabilities (cases) and nondisabled age- and sex-matched peers (controls)
Among PWD, history of any cognitive impairment or intellectual disability as determined by physician documentation during their index visit, use of assistive mobility device, continence status, and verbal status were collected as secondary characteristics, as was the use of a foreign language interpreter for all patients.
The primary outcome variables were receipt of each specific SRH guideline among those eligible based on age and gender. Adherence to each guideline was coded as “yes” or “no”. The number (percent) of eligible PWD and CC receiving each specific SRH recommendation was then calculated. An a prior power calculation determined that a sample size of 42 per group would provide us 80% power to detect a 25% or more difference between the group proportions at alpha equal to 0.05. To account for the matched categorical nature of the data, the Cochran-Mantel-Haenzel chi-square test was then utilized to explore whether adherence to SRH guidelines was independent of the presence of a complex medical condition and disability. Analysis was completed using SAS Enterprise Guide version 7.1 (Cary, NC, USA) and p-values were not adjusted for multiple comparisons.
There were 2350 total encounters, representing 1417 unique patients in the study period. The total number of unique patients in the PWD population was 144 (56 females, 38.9%), and the total number of unique patients in the CC population was 1273 (701 females, 55.1%). For forty-two unique patients in the PWD population, a unique CC patient of the same age and gender was available, with 17 females in each cohort (40%, Fig. 1). These 42 pairs constituted the study sample.
Schematic of identification of patients and matching strategy. PWD: Patients With Disability, CC: Comparison Cohort.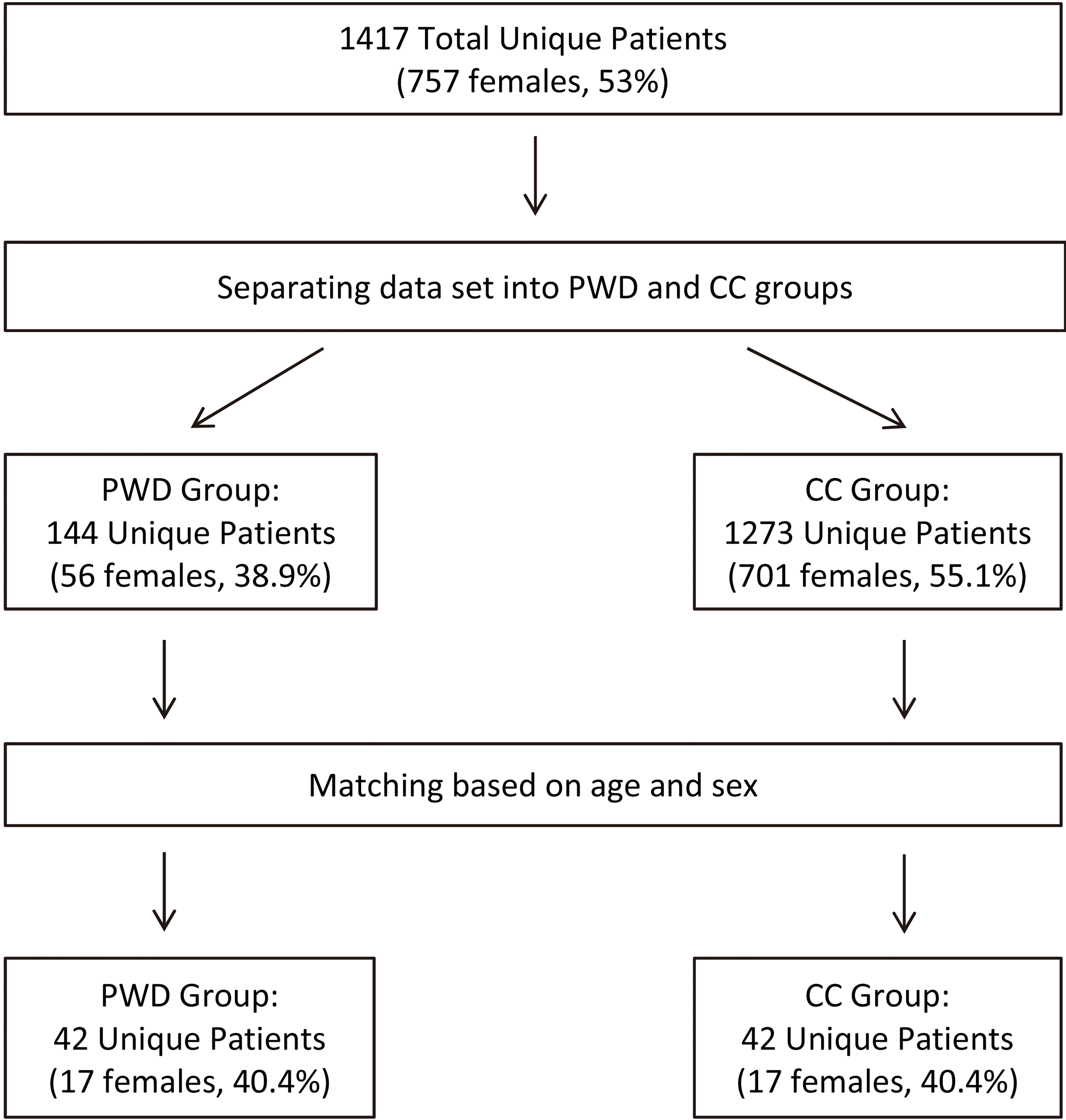
The mean age of PWD and CC was 17.3 years
All PWD were noted to have one or more disabilities: 30 (71.4%) were nonverbal, 33 (78.6%) used a device for assistance with mobility (i.e., wheelchair, crutches), 36 (85.7%) had documented intellectual disability, and 30 (71.4%) were incontinent (Table 2).
With the exception of initiation of the meningococcal vaccine series, there were no significant differences between eligible PWD and CC in adherence to immunization guidelines (Table 3). With respect to HPV vaccine completion, 11/40 (27.5%) of PWD and 19/42 (45.2%) of CC completed the series (
In contrast to vaccination, adherence to SRH history and screening recommendations was low on the whole and lower for PWD (Table 3). While the majority of individuals aged 15 years and older were not screened for HIV, screening was significantly lower among PWD as compared to CC: 2/28 (7.1%) PWD and 8/28 (28.6%) CC (
Among female patients, provider adherence to menstrual history taking was suboptimal overall, but worse for PWD. Documentation of LMP was equal between the two groups, which may be related to Epic’s auto-populate feature that pulls the most recent documented LMP. Notation of any menstrual history other than LMP was lower among PWD (17.7% vs 41.2%) but not significantly different (
Pregnancy history was documented in 0% of PWD versus 29.4% of CC (
The results of this study reveal that AYA with disabilities are less likely to receive routine reproductive healthcare in a primary-care setting as compared to those without disabilities. Medically complex and disabled patients are less likely to have appropriately documented histories for menstrual health, sexual activity, or pregnancy. In addition, they are less likely to have appropriate HIV screening. Without appropriate sexual history, it is impossible to know if AYA with disabilities are adequately screened for STIs. The higher rate of initiation of meningococcal vaccination among medically complex patients is not surprising, given the higher risk for invasive meningococcal disease among persons who have increased contact with healthcare systems and immunocompromised patients [30]. The finding that there is no significant difference between PWD and CC for initiation or completion of HPV vaccination is intriguing. This may indicate that adherence to routine reproductive healthcare is achievable when presented as a part of routine care in general.
It is interesting that provider adherence to history taking guidelines in general is lower than adherence to immunization recommendations. It can be difficult to obtain sensitive histories from patients with intellectual disability or limited verbal capacity, and it may feel too intimate to broach with a caregiver. It may also be that many other medical needs are felt to be more pressing, and many providers may feel that they have inadequate time to address this area of care. In addition, in patients who have profound intellectual disability, questions regarding sexual activity and sexual health may not be explored as providers may assume that these patients have minimal interest in sexual activity and limited ability to express this desire [13]. This is, however, not the case for people with mild-to-moderate intellectual disability or many types of physical disability [2, 3, 6, 7, 10, 12, 13, 15, 16]; additionally the increased risk of sexual exploitation in populations with disabilities [3, 9, 12]should prompt the provider to investigate sexual history regardless of a patient’s perceived capacity to experience sexual desire.
It may be that this is a type of unconscious bias among providers, or that providers simply do not consider the SRH needs of their patients with disabilities. A more concerning possibility is that the non-adherence to SRH guidelines may represent instead a form of unconscious bias, or that providers actively decide against the provision of SRH – or even asking questions – based on the incorrect belief that patients with disability are devoid of sexuality [1, 2, 7, 8, 12, 13, 15, 20, 32]. This study is not designed to determine the role of bias, unconscious or otherwise, in the provision of SRH to patients with disability, but further evaluation of bias and heuristics in the SRH care of patients with disability may reveal ways to improve this discrepancy. SRH and disability is not generally a part of medical school curricula, and it is not the specific purview of any particular medical discipline. The lack of a “home” for this topic only contributes to the potential for provider bias.
Current findings point to several future directions for improvement. As menstruation is not affected by cognitive capacity and can be a source of tremendous anxiety for both women with physical disabilities and their families and caregivers [21], adequately addressing menstrual history in disabled populations would be an excellent starting place. Women with disabilities are more likely to have comorbid conditions that may affect regular menses, such as being under- or overweight, genetic conditions, or use of certain medications. Women with epilepsy or behavioral problems may be at risk for worsening of symptoms around the time of menses [14, 32]. Since abnormal menses can also have a large impact on overall health, appropriately addressing this part of a young woman’s life is essential regardless of her abilities.
Future studies should also explore ways to improve appropriate sexual history-taking in the medically complex and disabled population. Sexual history taking is of utmost importance as it allows identification of patients appropriate for STI screening and should include documentation of histories of coercive or forced sex, which is much more common in this population [3, 4, 7, 9, 12, 33].
An additional area of improvement may be to address existing guidelines and determine if they are appropriate for patients with physical and intellectual disabilities or require adaptation. Several special populations are discussed in current recommendations – for example, people seeking healthcare at an adolescent clinic, incarcerated people, men who have sex with men, and gender minority people [22, 23, 24, 25] – however, these guidelines are silent on the topic of people with disabilities. Perhaps certain guidelines (i.e., STI screening) are not appropriate for women with profound intellectual disability due to their perceived lower rates of sexual activity, although there is always the risk of rape and sexual assault. As such, specific discussion for medically complex and disabled populations may be necessary.
There are several limitations to this study. This is a retrospective chart review, and as such, documentation in the patient chart may not reflect all conversations between the patient, the patient’s family, and the provider. The provider may have offered services to the patient and/or the patient’s caregivers, which may have been subsequently declined. Unless the provider specifically documented that the family declined services, this would be coded as the provider failing to provide appropriate SRH. The small sample size forms an additional limitation. We were underpowered to detect differences of less than 25% between the group proportions which could have been clinically relevant, but would not have been statistically significant with the current sample sizes. In addition, this was a single-site study and patients were enrolled from a clinic devoted to the primary care of medically complex and disabled patients, and as such, findings may not be generalizable to patients seeking care in other settings or other populations of patients with disabilities.
An important limitation of this and other studies about disability is the challenge of defining “disability,” as well as the difficulty of separating populations with physical disability only from populations with intellectual disability only, and again from populations with mixed disability [3, 4, 6, 9, 33]. Many studies examining disability using large databases such as Add Health (the National Longitudinal Survey of Adolescent Health) extrapolate the presence or absence of disability from responses identifying functional limitations or use of durable medical equipment [6]; others have focused purely on populations receiving care for specific disabilities [16]. In this study, we attempt to separate patients with disabilities from those without by looking at populations from two separate clinics: one devoted to the care of complex medical conditions with significant impact on the “full and effective participation in society on an equal basis with others” [1], and another devoted to the care of a general population. While this clearly is not a perfect way to study healthcare delivery to these populations – for example, even though documented disability in patients from the general medicine-pediatrics clinic is an exclusion criterion, patients with a disability that is not documented in their chart may still be present in the analysis; there are also patients with no intellectual disability at all in the clinic devoted to medical complexity – the comparison of these two clinics does reveal that in different settings, different medical care is offered to different patients.
This study is also limited by the relatively few female patients included in our analysis, which is reflective of the overall milieu of the complex healthcare clinic; most of the patients seeking primary care in that clinic are male. This limits the generalizability of this study with respect to populations with more women.
In discussing problems with access to good sexual and reproductive healthcare and education, the World Health Organization notes that “The ignorance and attitudes of society and individuals, including health-care providers, raise most of these barriers – not the disabilities themselves” [2]. Barriers to good sexual healthcare and education arise from the actions of populations without disability. Addressing these attitudes and beliefs about disability can ultimately lead to improved health for all parties, and doing so must include the voices of people with disabilities themselves [2].
Footnotes
Acknowledgments
The authors would like to recognize the editorial skills of Ms Beth Thielman for review of this manuscript.
Conflict of interest
The authors have no financial or other relationships relevant to this article to disclose.