
Abstract
Background:
Women with disabilities have a similar desire for pregnancy as their non-disabled peers but experience more ambivalence and doubt about their intention to have a child. While many have healthy pregnancies, they face higher risks and trade-offs in health, function, and independence.
Objectives:
To review the literature on pregnancy in women with physical disabilities to guide interventions and clinical care guidelines.
Eligibility criteria:
Abstracts were reviewed if they were original research on pregnancy involving adult women with physical disabilities. Both qualitative and quantitative studies were included, with no restrictions on language or publication year.
Sources of evidence:
PubMed, Scopus, and CINAHL Complete and reference lists of eligible articles.
Charting methods:
Abstracts were eligible for full-text review if they were (1) original research, (2) in humans, (3) about pregnancy, and (4) involved adult women with physical disabilities. Data were extracted by independent reviewers using Covidence software and assessed with a customized critical appraisal guide.
Results:
Five major topics characterized 171 reviewed articles: (1) rates of pregnancy, fertility, and termination or loss; (2) pregnancy complications and infant outcomes; (3) effects of pregnancy on physical function disease activity; (4) maternal care; and (5) social and interpersonal dimensions of pregnancy. Most studies were conducted in the Americas and Europe, and high-income countries used a quantitative design and were assessed to have a moderate risk of bias.
Conclusions:
This review highlights the need for future research to (1) build a stronger evidence base for tailored maternal care, (2) examine disability discrimination’s impact on pregnancy outcomes, (3) develop interventions to reduce disability-related inequities, and (4) improve disability competence among maternal care providers.
Plain Language Summary
Introduction
Approximately 1.3 billion people, or 16% of the world’s population, have a disability. 1 “Disability” is a broad term that encompasses impairments (i.e., absence of or significant difference in a person’s body structure or function or mental functioning), activity limitations (i.e., execution of a task or action by an individual), and participation restrictions (i.e., a person’s involvement in a life situation). 2 Disability is considered integral to the human experience and dynamic over time, reflecting the interaction of an individual’s body with the society in which they live. 1
Nearly 20% of women worldwide have a disability, and of these, 8.9% are of childbearing age (18–49 years). 3 In both low- and high-income countries, girls and women with disabilities face greater discrimination, limited access to healthcare, and vulnerability to violence.1,4 Disability discrimination is also associated with poorer well-being and psychological distress, 5 and internalization of stigma,6,7 and can amplify health disparities. 8 Reproductive freedom for women with disabilities is especially vulnerable to negative disability stereotypes, particularly regarding pregnancy.9 –16
While women with disabilities have a desire for pregnancy similar to their non-disabled peers, they also have higher levels of ambivalence, uncertainty, and doubt about their intention to have a child.17,18 They are almost twice as likely to be uncertain about realizing their intention to have biological children compared to their non-disabled peers. 19 Although many can and do have healthy pregnancies, pregnancy is not without elevated risks and significant trade-offs in health, function, and independence. Women with disabilities are twice as likely to start prenatal care after the first trimester and receive inadequate care compared to their non-disabled peers. 20 Routine prenatal care is also limited by environmental barriers such as inaccessible examination tables and inaccessible weight scales. 21 Moreover, these women are less likely to have support after giving birth and visit their physician for postpartum checkups. 20
Barriers to healthcare affect not only patients but also healthcare providers who face their own ambivalence and limited knowledge of disability22,23 and the impacts of this on providing necessary care. 24 They also struggle with limited knowledge and a lack of clinical care guidelines 25 to guide them. Inadequate knowledge can lead to inaccurate or inappropriate guidance on risks and potential complications, resulting in poor decision-making about a future pregnancy. 11 Despite these challenges, rates of pregnancy in women with disabilities have tripled in the last two decades. 26
Many of these challenges are due to or are amplified by a lack of systematic evidence for informed care at the intersection of pregnancy and disability. 27 To date, there have been a handful of systematic reviews on pregnancy and disability. This includes reviews on perinatal outcomes, 28 maternal care experiences, 29 healthcare interventions to improve pregnancy outcomes, 30 maternal complications and infant outcomes, 31 and access to and utilization of maternity care and domestic abuse. 32 By design, these reviews have focused on narrow questions and include more than one broad category (e.g., physical, sensory, or intellectual/cognitive) of disability. Focusing on a single type of disability – as we do here – allows for a more in-depth and comprehensive understanding of the specific challenges, needs, and experiences of that population. The goal of this scoping review was to characterize, synthesize, and evaluate the literature on pregnancy in women with physical disabilities characterized by an impairment of mobility to identify gaps in knowledge and make recommendations for future research to address these gaps.
Methods
Protocol
We used a scoping review methodological framework that allows for the inclusion of a diversity of literature and study designs, enabling a broader range of inquiry.33,34 Scoping reviews are a type of knowledge synthesis that uses a systematic approach to map evidence on a specific topic, identifying main concepts, theories, sources, and gaps in knowledge to guide future research. 35 Rather than answering a single question, these reviews can be particularly valuable for investigating available evidence, how the research has been conducted, and identifying gaps in the knowledge base. 36 We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-Scr) 35 to guide the search strategy, study selection, data collection, and reporting in this review.
Eligibility criteria
Eligibility assessment of each abstract was performed by a single reviewer using a standardized form. Inclusion criteria were: (1) original research studies, (2) in humans, (3) about pregnancy, and (4) involved adult women with physical disabilities. Pregnancy was broadly defined to include studies addressing fertility, labor, and delivery, pregnancy complications and infant outcomes, and maternal care and access. For studies that included pregnancy in addition to other reproductive health topics, there had to be a substantive inclusion of data on pregnancy. Physical disability was defined broadly by some degree of impaired mobility, irrespective of cause, such as injury or health condition. When impairment was not explicitly assessed, we were overly inclusive based on the condition or injury. For studies that involved multiple types of disabilities, for example, cognitive, sensory, or physical, at least 50% of the sample had to include a physical disability or an analysis had to be performed for the sub-sample with a physical disability. Studies that focused only on the perspective of caregivers or healthcare providers were excluded. Both qualitative and quantitative study designs were included; we excluded systematic reviews, narrative literature reviews, case studies, editorials, and abstracts. No limits were placed on year of publication or language. Articles meeting inclusion criteria that were not published in English were translated using Google Translate.
Information sources and search strategy
The search was applied to PubMed (1966–present), Scopus (1960–present), and CINAHL Complete (1981 – present); the final search was performed on July 2, 2022. We used the following search terms to search all databases: pregnancy, pregnant, disability, disabilities, and mobility impairment. We also hand-searched reference lists of articles that underwent full-text review for additional articles not identified in the database searches (see Table 1 for search syntax).
Search syntax and database. a

Final search performed on July 7, 2022.
Eligibility review and data extraction
A single reviewer (LM) conducted the initial step of title and abstract review; we were overly inclusive at this stage to mitigate any risk of missing a relevant article. Working in pairs, four reviewers (LM, SM, JK, RP) then independently reviewed each article for eligibility using Covidence, an online platform for systematic reviews and meta-analyses. Discrepancies were resolved through consensus with a third reviewer (CK). Blinded double-extraction was performed by eight reviewers (LM, SM, JK, RP, SC, MB, SP, CK). The following data were extracted from each article: sponsorship source; study country; year published; study design; guiding framework/theory (for qualitative studies); study purpose; inclusion and exclusion criteria; sampling method; sample size; source of sample; cause of disability or disabling condition; and study outcomes and results. Discrepancies in the data extractions were resolved through consensus between the paired reviewers and a third reviewer (CK) whenever needed.
Critical appraisal
While scoping reviews do not always include a critical appraisal of bias 37 nor is this required by the PRISMA-ScR guidelines, 35 we chose to evaluate the risk of bias in the reviewed studies. We developed a customized critical appraisal guide to assess six study designs (i.e., cohort, cross-sectional, case series, qualitative, case–control, and randomized controlled trials) that were eligible for this review. We drew on four established critical appraisal tools: the Scottish Intercollegiate Guidelines Network, 38 the Evaluation Tool for Qualitative Studies, 39 the Institute of Health Economics, 40 and the Appraisal tool for Cross-Sectional Studies. 41 Each eligible article was evaluated using a rating system that aligned with its study design. A common metric was used to rate studies as having a low, moderate, or high risk of bias. In cases where mixed methods were used, the dominant design determined the selection of the rating system. One reviewer (LM) developed and pilot-tested the guide and trained the other reviewers. Criteria were rated independently, and discrepancies were resolved by consensus. See Supplemental Materials for the Critical Appraisal Guide.
Synthesis of results
We synthesized the extracted information, both descriptively and thematically. As suggested by Arksey and O’Malley 34 and Levac, 33 scoping reviews are not simply a summary of many articles but a more in-depth examination of a body of literature. After all the data were extracted, we created an initial organization of major topics and iteratively developed the structure. We aggregated article characteristics (e.g., study design type, risk of bias, cause of disability) to create an overall picture of the body of literature. We also examined factors that drove risk of bias for any distinct patterns across study designs or topic areas.
Results
From the search, 2757 records were identified in the electronic databases, and another 3389 records were identified through hand-searching references. After duplicates were removed, 5847 citations were moved on to title and abstract review. Of these, 5595 were excluded, and 205 full-text articles were retrieved and reviewed for eligibility. A final set of 171 studies were included in the review (see Figure 1).
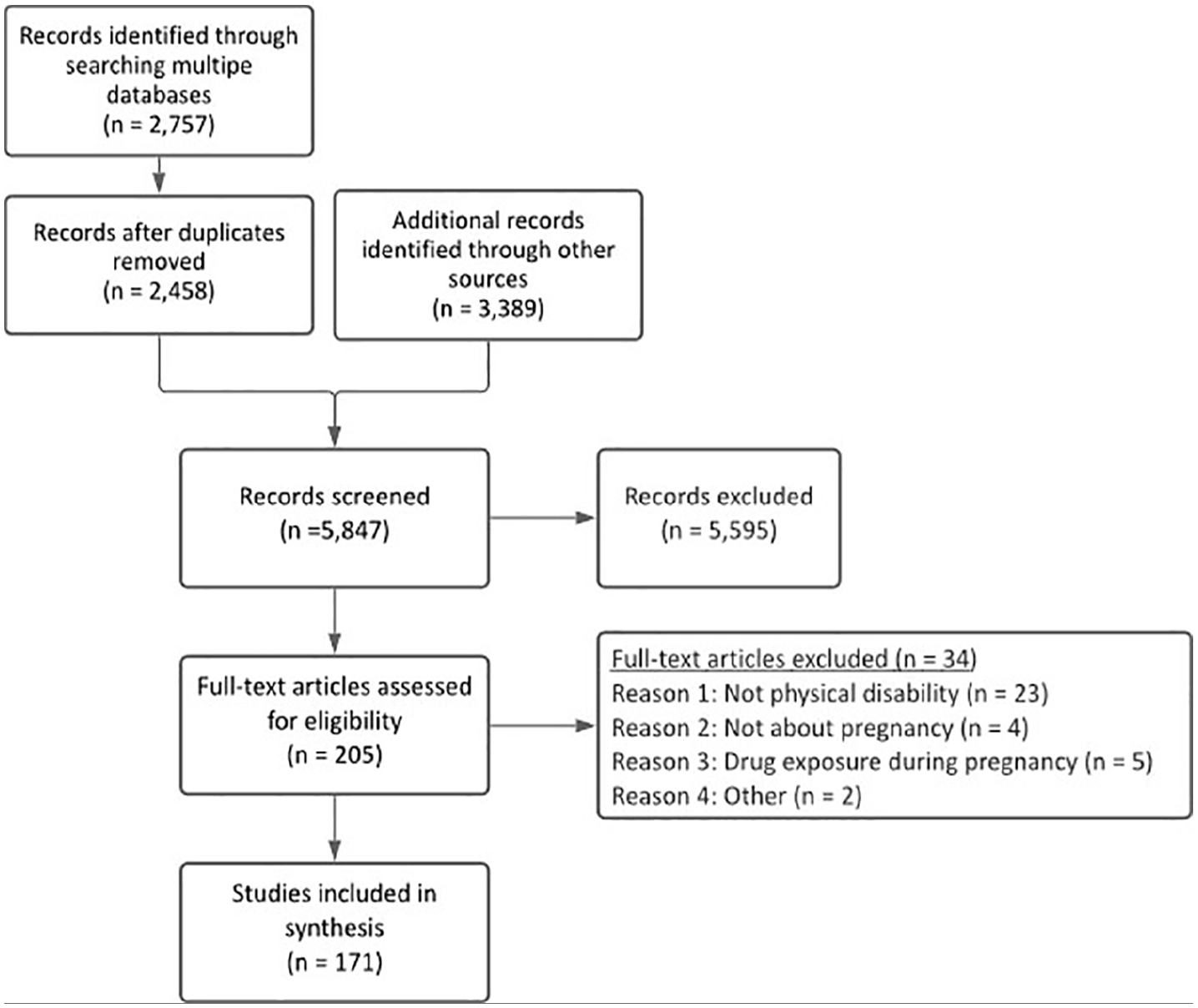
PRISMA diagram.
Characteristics of reviewed studies
A span of nearly 70 years was covered in our review, beginning in 1953 with only one study published every decade or so until a gradual rise in the early 2000s (see Figure 2). The 35 countries represented in the included articles were categorized using the World Health Organization (WHO) world regions and the World Bank Income Classification. Most studies were conducted in the Americas or Europe and high-income countries (Figure 3). Many used a quantitative study design and had a moderate risk of bias (see Figure 4). For an overview of studies included in the review, see Supplemental Table 1.

Years of publication.

Representation of studies by WHO Region and World Bank Income Classification.

Risk of bias by study design.
The most frequent cause of disability among studies was multiple sclerosis (MS; n = 71), followed by physical disabilities due to mixed causes (n = 53), rheumatoid arthritis (RA; n = 22), and spinal cord injury (SCI; n = 17). A mix of other specific conditions (cerebral palsy, myotonic dystrophy, spina bifida, chondrodystrophy, juvenile idiopathic arthritis) was represented in a handful of studies (n = 9).
Major topic areas
The 171 reviewed articles were characterized by five major topics and 17 subtopics, which are summarized in Table 2. Table 3 summarizes the distribution of study design, risk of bias, WHO region, and World Bank income classifications by major topics. Sample sizes varied widely between and within study designs; median sample sizes by study design are reported in Table 3 footnotes. In general, quantitative designs were primarily distributed across topics, while qualitative designs concentrated on studies about maternal care and social and interpersonal aspects of care. Risk of bias ratings were generally distributed across topics and study designs.
Major topic and sub-topic descriptions. a

Topics are not mutually exclusive.

Categories are not mutually exclusive; % refers to proportion within each topic area.
Median sample size (min, max) by study design
• Case control – 107 (49, 674)
• Case series – 20.5 (5, 47)
• Cross-sectional – 410.5 (50, 18,810,055)
• Prospective cohort – 61.5 (15, 1872)
• Qualitative – 22 (5, 70)
• Retrospective cohort – 1169 (6, 5,432,524)
The cause of disability was not equally represented across all major topics and sub-topics. For example, MS or RA were primarily represented in studies addressing the effects of pregnancy on disease activity, complications, and fertility. Very few studies in these populations addressed the social aspects of pregnancy, and none addressed maternal care. In contrast, physical disability from mixed causes was predominantly represented in studies about maternal care and the social dimensions of pregnancy but less so in fertility, complications, and effects on function. The distribution of disability causes among sub-topics is shown in Figure 5.

Disability representation in major themes and sub-topics.
Rates of pregnancy, fertility, and termination or loss
Forty-one articles addressed pregnancy rates, fertility, and loss or elective termination. These studies used a mix of study designs that generally had a moderate risk of bias and were conducted mainly in Europe or the Americas (see Table 3). Studies on rates of pregnancy (n = 13) addressed trends in pregnancy over time, factors related to unintended pregnancy, and the impact of injury or diagnosis onset and impairment severity on pregnancy rates. In statistical comparison to their non-disabled peers, women with physical disabilities typically had significantly fewer pregnancies,42 –45 but not in all studies reviewed. 46 Despite lower overall rates, in the United States their pregnancy rates rose from 0.27% in 2000 to 0.80% in 2010. 47 Higher rates of unintended pregnancy were associated with having a physical disability 48 or a lack of information from providers about pregnancy planning with MS. 49 The severity or complexity of disability related to cerebral palsy was inversely related to the likelihood of pregnancy. 50 Rates of pregnancy before and after SCI were comparable 51 with higher rates occurring some years after injury. 52 Duration of transient post-SCI amenorrhea was not significantly associated with successful pregnancies. 53 A younger age at the time of SCI was significantly associated with higher rates of pregnancy, 53 in contrast to fewer pregnancies associated with younger age of RA diagnosis (see Table 4). 54
Fertility and pregnancy loss and termination.

Abbreviations: 95% CI: 95% confidence interval; AOR: adjusted odds ratios; MS: multiple sclerosis; OR: odds ratios; RA: rheumatoid arthritis; RR: risk ratio SCI: spinal cord injury.
For group comparisons, statistics (e.g., AOR, OR, RR, and p-values) are reported when available. In cases where no comparisons are made, descriptives are reported.
N. S. = not statistically significant when p-values are reported < 0.05.
Five studies examining fertility focused on the use of assisted reproductive technology or fecundity, primarily in women with MS and RA. In one of the earliest studies in the review from 1965, fertility appeared to be both lower before and after disease onset among women with RA. 77 Higher relapse rates of MS were associated with in vitro fertilization treatments versus prior to treatment 79 and with a greater need for artificial insemination versus women without MS. 80 Greater MS disease activity was also associated with using assisted reproductive technologies. 81 Fecundity among women with physical disabilities after unprotected sex was found to be similar to their non-disabled peers. 82
Twenty-nine studies on pregnancy loss (nonviable intrauterine pregnancy up to 20 weeks of gestation) and/or elective termination (abortion), focused on rates within specified groups, with relatively few statistical comparisons to controls. In the few direct comparisons, significantly higher rates of pregnancy loss occurred among women with MS,55,61 RA, 46 and mixed physical disabilities, 45 but not in all studies. 44 Seventeen studies reported only descriptives of pregnancy loss within cohorts of women with SCI53,64 –66 (and combined loss and elective termination 63 ), MS,56 –60 chondrodystrophies, 71 cerebral palsy,72,73 myotonic dystrophy, 69 spina bifida, 74 and physical disabilities.18,70 Women with juvenile RA had slightly lower rates of loss than controls (though no statistics were provided). 68 Finally, studies examining factors associated with pregnancy loss suggested exposure to Natalizumab (an immunosuppressive drug) in women with MS increased likelihood of pregnancy loss 62 and for women with SCI, pregnancy loss was higher before injury than after. 51 Among women with myotonic dystrophies who had infants with the carrier gene, pregnancy loss was higher than those without the carrier gene. 78
The 17 studies of elective terminations included only two direct comparisons with controls among women with MS (no differences 61 ) and RA (higher rates 46 ). The remaining studies only reported frequencies within their respective samples of women with SCI,53,65,66 MS,56 –60,75,76 myotonic dystrophy, 69 mixed physical disabilities,18,70 cerebral palsy,72,73 spina bifida, 74 and chondrodystrophies (see Table 4 for details). 71
Pregnancy complications and infant outcomes
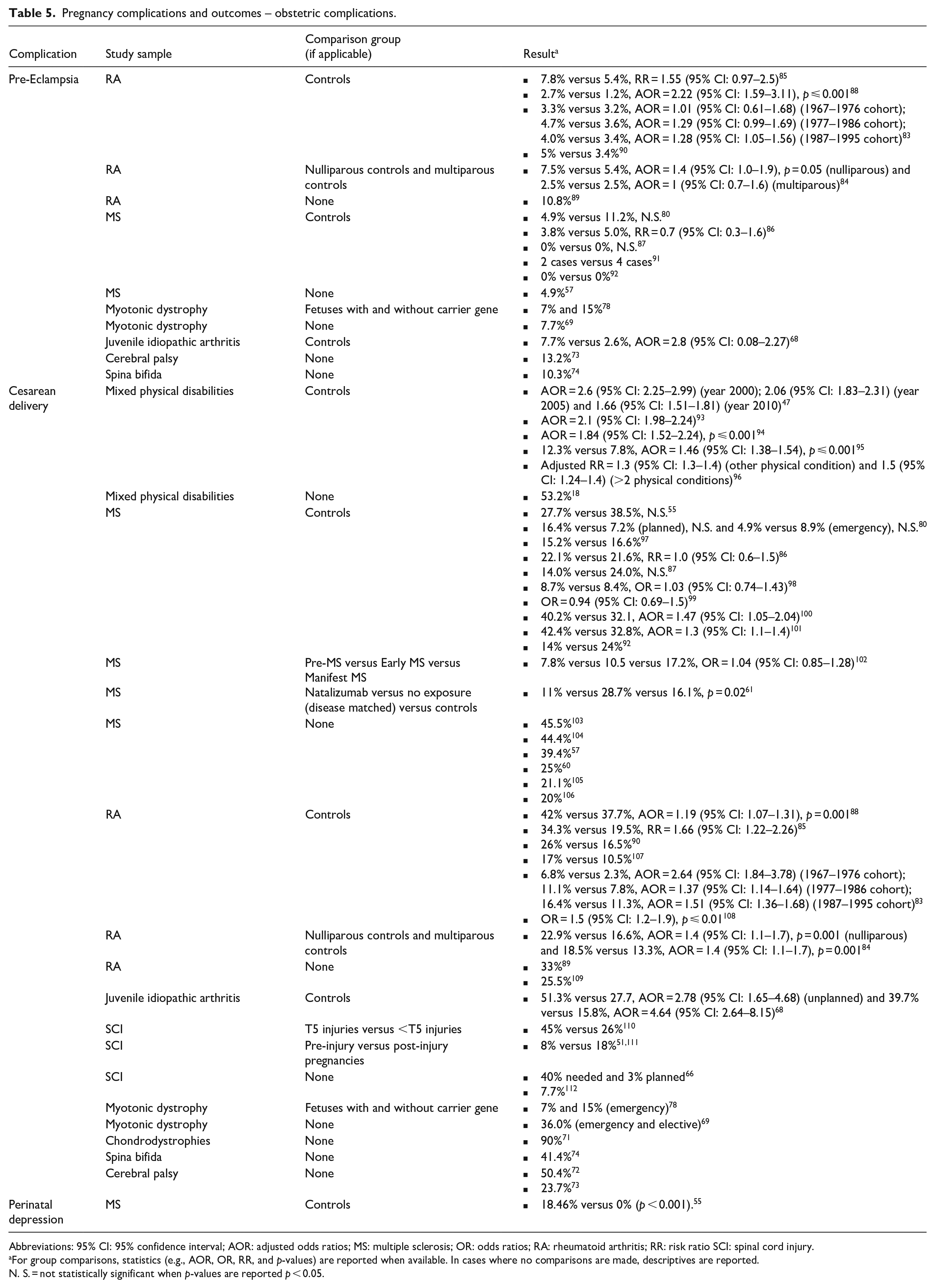
Seventy-two articles addressed pregnancy complications and infant outcomes using a variety of study designs, primarily quantitative, many of which had a moderate risk of bias. These were conducted mainly in Europe or the Americas and high-income countries (see Table 3). Studies on obstetric complications (n = 33) focused on complications that may be exacerbated by the presence of physical disability or where pregnancy may exacerbate disability-related factors. In statistical comparisons to controls, incidence of pre-eclampsia was generally similar among women with RA,83 –85 MS,57,86,87 and juvenile idiopathic arthritis, 68 but some studies found a higher rate among women with RA.83,88 The remaining studies only reported rates of pre-eclampsia in the study samples among women with RA89,90 MS,57,91,92 cerebral palsy, 73 spina bifida, 74 and myotonic dystrophy (see Table 5). 78
Pregnancy complications and outcomes – obstetric complications.
Abbreviations: 95% CI: 95% confidence interval; AOR: adjusted odds ratios; MS: multiple sclerosis; OR: odds ratios; RA: rheumatoid arthritis; RR: risk ratio SCI: spinal cord injury.
For group comparisons, statistics (e.g., AOR, OR, RR, and p-values) are reported when available. In cases where no comparisons are made, descriptives are reported.
N. S. = not statistically significant when p-values are reported p < 0.05.
Other complications during pregnancy varied by the cause of disability. For women with SCI, there could be increased frequency or severity of autonomic dysreflexia,51,65,63,110,113,114 spasticity,51,63 or pressure injuries. 51 Urinary tract infections or neurogenic bladder were also common in both SCI63 –65,67,111,113,114 and spina bifida. 74 Other complications less frequently cited included anemia and gestational diabetes in MS, 86 placenta previa in myotonic dystrophy69,78 and MS, 86 postpartum hemorrhage in juvenile RA, 68 pyelonephritis in SCI, 64 and gestational hypertension in mixed physical disabilities, 73 spina bifida, 74 and MS. 115 In one study, there were no differences in complications during pregnancy in women with MS compared to the general population. 80
Pregnant women with mixed physical disabilities had a higher risk of severe maternal morbidity or mortality than their peers, including postpartum hemorrhage, ICU admission, and puerperal sepsis. 116 They were also more likely to report fair or poor health, 50 mental health problems, 117 or have one or more other health conditions during pregnancy.96,118 In a qualitative exploration of pregnancy complications related to functional impairments, women expressed concerns about falls, urinary tract and bladder problems, wheelchair fit, and stability, safety, and mobility, requiring respiratory support, increased spasticity, bowel management problems, and skin integrity. 119
Articles reporting on labor and delivery (n = 49) addressed rates of cesarean birth, the use of induction, instrumentation, and the experience of labor and delivery. A majority of these (n = 43) addressed rates of cesarean births. In statistical comparisons to controls, women with mixed disabilities,47,93 –96 RA,83 –85,88,108 and juvenile idiopathic arthritis 68 had consistently and significantly higher rates of cesarean deliveries. In contrast, among women with MS, rates were consistently comparable to their peers.55,80,86,87,98 –101 The remaining reviewed studies only reported rates of cesarean deliveries among women with mixed disabilities, 18 chondrodystrophies, 71 spina bifida, 74 SCI,51,66,110 –112 cerebral palsy,72,73 MS,57,60,92,97,103 –106 RA,89,90,107,109 and myotonic dystrophy (see Table 5).69,78
A handful of studies examined disability or disease characteristics and their relationship to cesarean births. Women with SCI with cervical-level injuries were more likely to have a cesarean delivery than those with paraplegia. 110 Among women with MS, later stages of the disease were associated with a higher likelihood of cesarean births versus earlier disease stages. 102 Instrumentation during delivery or induction was also needed among women with juvenile idiopathic arthritis, 68 MS,75,92,98,106,120,121 and myotonic dystrophy. 78 Higher levels of impairment due to MS were associated with a greater likelihood of instrumentation use, 122 although not in all studies. 99
Studies that included hospitalizations during pregnancy or after delivery (n = 9) typically reported longer stays after delivery55,85,96,108,114,123 or higher rates of re-hospitalization 86 among women with physical disabilities versus their non-disabled peers, although this was not always the case. 115 Women with MS were also more likely versus controls to have more emergency room visits and hospitalizations during their pregnancy. 99
Three qualitative articles explored the lived experience of labor and delivery, anesthesia, and pain management planning among women with mixed physical disabilities. In these studies, participants emphasized the importance of having choices, planning, and collaborating with knowledgeable healthcare providers and expressed fears that their wishes would not be honored or possible.23,124,125 Despite such challenges, they reported labor and delivery to be an overall positive experience. A fourth qualitative study exploring the influence of healthcare providers, family, and friends on decisions about childbirth found provider recommendations for a cesarean birth to be a “directive” and supported by their peers as the “rule” for women with physical disability. 126
Perinatal depression or overall psychological well-being (n = 4) was rarely addressed in reviewed studies. In direct comparison to peers, women with MS also had statistically significantly higher rates of perinatal depression than their peers (see Table 5). 55 Women with mixed physical disabilities reported that midwives were statistically significantly less likely to inquire about how they were feeling emotionally prenatally and postnatally compared to their non-disabled peers. 123 Perinatal depression was among the most common complications of postpartum for women with SCI 63 with higher levels of depression (per self-report and clinical diagnosis) more likely among those with lower-level injuries. 127
Studies reporting infant outcomes (n = 41) concentrated on rates of pre-term birth, low birth weight, and infant death, with comparisons typically made either to controls or within group characteristics. In statistical comparisons to controls, rates of pre-term birth were somewhat mixed, though generally similar to peers. For women with MS, most comparisons were not statistically significant,55,61,80,87,98,97,102 with one exception. 100 In contrast, rates of pre-term births in women with RA were more often higher versus controls in reviewed studies,84,85,90 with some variability by number of weeks 90 and cohort year. 83 Rates of pre-term birth were also significantly higher among women with juvenile idiopathic arthritis, 68 and mixed physical disabilities. 96 Rates (without statistical testing) of pre-term birth also varied by disease characteristics such as severity of disease in RA 109 or exposure to treatment of MS with Natalizumab.62,76 The rates (no comparisons) of pre-term births were reported for women with MS,92,106 SCI,63,65 –67 spina bifida, 74 cerebral palsy,72,73 myotonic dystrophy, 69 and RA 89 in the reviewed studies (see Table 6).
Pregnancy complications and outcomes – outcomes of fetus or infant.

Abbreviations: 95% CI: 95% confidence interval; AOR: adjusted odds ratios; MS: multiple sclerosis; OR: odds ratios; RA: rheumatoid arthritis; RR: risk ratio SCI: spinal cord injury.
For group comparisons, statistics (e.g., AOR, OR, RR, and p-values) are reported when available. In cases where no comparisons are made, descriptives are reported.
N. S. = not statistically significant when p-values are reported < 0.05.
Findings across studies examining birth weight also varied by study and population. In statistical comparisons to controls, most studies among women with MS found comparable rates of low birth weights55,80,86,99,100 with an average lower weight in one study. 98 Comparable rates were also found within MS cohorts by the duration of MS 102 and exposure to Natalizumab. 61 Among women with RA, rates of low birth weight were mixed with significantly higher 88 and non-significant differences overall 85 and by parous status 84 and remission status. 128 Among women with mixed physical disabilities, low birth weight was significantly greater than controls. 96 Among women with SCI, low birth weight among post-injury births was higher versus pre-injury births (no significance testing).51,111 The remaining studies only reported rates of low birth weight among women with cerebral palsy, 72 RA,107,109 spina bifida, 74 cerebral palsy, 72 SCI,63,65 and cerebral palsy 72 (see Table 6).
Infant deaths were reported in 17 studies. In statistical comparison to controls, rates were non-significant among women with MS,55,80,86 RA 90 and among nulliparous and multiparous women with RA. 84 The remaining studies reported counts or rates with no comparisons to controls among women with MS,57,59,75,105 RA, 77 cerebral palsy, 72 myotonic dystrophies 69 and by fetuses with the carrier gene, 78 and SCI51,65,110,112 (see Table 6).
Effects of pregnancy on physical function and disease activity
Fifty-five articles addressed the effects of pregnancy on physical function and disease activity. The majority used a prospective or retrospective cohort design, had a moderate risk of bias, and were almost exclusively conducted in Europe, the Americas, and high-income countries (see Table 4).
In terms of changes in physical function (n = 18), there appears to be some protective effects of pregnancy against functional loss in some conditions. Functional loss among women with polyarthritis was mitigated by pregnancy, but appeared to decline over time. 129 Pregnancy slowed disability progression in MS (versus a nulliparous state)56,120,130 –137 and a lack of significant association of pregnancy with functional loss in MS120,130,138 –141 or RA. 142 Although this was not uniform across all studies, 135 such as a greater likelihood of using a wheelchair later in life after pregnancy in MS. 143 Women with SCI also experience a greater risk of worsened spasticity and autonomic dysreflexia during pregnancy. 51
Studies focusing on disease activity (e.g., relapse or flares; n = 51) were dominated by studies involving women with auto-immune-related disorders. The earliest study in the review, from 1953, focused on the exacerbation of disease in women with MS. 75 On the whole, women with MS experienced a reduction in relapse rates, especially in the third trimester,144,145 with an increasing relapse rate occurring in the first 3–6 months postpartum.58,59,120,130,135,137,146 –153 Some findings have suggested a protective effect of pregnancy such that parous women may be more at risk for developing secondary progressive MS, 97 but relapse rates have also been found to lower before pregnancy versus up to six years after delivery. 154 Studies of MS disease activity during pregnancy or postpartum suggested changes in biological mechanisms such as thyroid autoimmunity, 97 gene expression, 155 immunological responses,156 –158 and physiologic protective mechanisms, such as the reduction of natural killer cells in the body. 157 Immunomodulation appears to lead to a reduction in disease activity.155,157,159,160 The use of assisted reproductive technologies resulted in a higher relapse rate79,161,162 and/or disease activity. 81 Factors such as breastfeeding,146,163,164 epidural anesthesia,104,146 and labor induction60,121 were not associated with higher relapse rates; breastfeeding was associated with a lower risk of relapse after delivery. 136 Studies involving women with RA were similarly focused on measures of disease activity165 –167 and flares.89,168 –170
Maternal care
Thirty-four articles addressed some aspects of maternal care mainly using a qualitative study design with a moderate risk of bias. For this topic, there was more diversity of world regions, with a plurality in Europe and the Americas and high-income countries (see Table 4). Articles addressing accessing and/or utilizing maternal care services (n = 23) primarily addressed barriers to care in preparation for pregnancy or the experience of maternal care among women with physical disabilities. Barriers in the built environment, such as inaccessible examination tables and weight scales 21 or other specialized equipment,171,172 a lack of accommodations, such as assistance with infant care or placement of a personal wheelchair in a hospital room, 173 confusing referral procedures, 172 or inaccessible facilities,172,174 –176 are challenges to high-quality maternal care. Moreover, such barriers were not restricted to low-resource settings.13,177 –179 In low-to-middle-income countries, the geographical location of facilities and/or skilled care, such as their distance,175,180 the ability to travel to them,175,181 and cost or inaccessibility of transportation172,175 were additional barriers to accessing care.
With respect to family planning services, women with mixed physical disabilities were less likely to receive them 182 and have their needs met. 183 Prenatal care utilization or number of visits did not always differ between women with and without physical disabilities;43,70 in some cases, care was utilized more. 94 Traditional beliefs about the transmission of disabilities could also be a barrier to seeking prenatal care. 180 Women with mixed physical disabilities were more likely than their non-disabled peers to choose a place to give birth and a comfortable position in labor. Still, they were less likely to meet medical staff before labor or feel they were always involved in decision-making about care. 94 Disability also played a role in the selection of a maternal care provider. 184 Unmet needs included guidance or support for breastfeeding,11,123 recommendations for baby care equipment, 176 reducing barriers to infant care, 185 information to support women after delivery, 11 and specialized prenatal care, such as occupational and physical therapy.72,176
Articles that addressed the knowledge about pregnancy and disability (n = 20) highlighted the challenges of the limited knowledge of providers to discuss a future pregnancy or guiding women during pregnancy.11,13,49,63,171,173,175 –178,181,184 –187 Unsurprisingly, a lack of knowledge resulted in women’s needs going unrecognized and not discussed, 188 or a poor understanding of their potential for pregnancy. 187 Women with mixed physical disabilities receiving care from midwives were significantly less likely to get advice about postnatal physical recovery or contraception from their midwives compared to their non-disabled peers. 123 Women also struggled with having limited information172,189 or understanding the information given to them, 49 while others obtained more information from lay sources 176 or their peers. 172 Women could be tasked with educating their providers about their disability, 179 but even then, their knowledge and expertise about their disability could be disregarded. 186
Fourteen articles addressed interpersonal aspects of care that were experienced in relationships with healthcare providers. The focus of these was mainly on support in the pregnancy decision-making process or maternal care planning. When positive support was received, women felt protected and cared for.185,187 However, interactions with healthcare providers could also be a source of discrimination, stigma, disrespect,123,185 and discouragement from pursuing reproductive goals. 187 When healthcare providers were perceived as feeling themselves to be “superior,” this damaged the sense of support and autonomy in that relationship. 190 Nervousness and discomfort of healthcare providers could also be palpable when receiving care. 181
Balancing autonomy and having others “take over” could be especially challenging in managing relationships with healthcare providers. 191 “Unhelpful” help could occur when assistance was given but not requested. 192 The ability to self-advocate with healthcare providers could be a powerful tool in shaping a positive experience of maternal care and getting needs met. 178 Despite having a sense of autonomy and control during childbirth, power dynamics could often tip toward healthcare providers. 191 Continuity of care could also be challenging when multiple healthcare providers are involved; 173 a lack of communication between them could place an undue burden on women. 171 In some cases, challenges around communication imperiled the life of the mother and the child. 13 Cultural biases and stigma expressed by healthcare providers often reflected the broader culture, 175 with some women offered termination of their pregnancy because of their disability status.185,193 Finally, the desire to be treated “normally” could come into conflict with their more complex needs during pregnancy. 188
Articles addressing satisfaction with maternal care and/or unmet needs (n = 9) generally found lower levels of overall satisfaction,173,176 although this was not uniform.104,191 In some cases, satisfaction was higher compared to non-disabled peers. 193 Inadequate accommodations 173 or poor coordination between healthcare providers 171 led to reduced satisfaction with maternal care. Greater unmet needs were also associated with limited knowledge of both healthcare providers and women themselves 184 or not having enough information to guide breastfeeding or to make appropriate decisions around infant care. 178 Among women with mixed physical disabilities, not receiving the anesthesia care they planned for during labor and delivery led to greater dissatisfaction with care. 125 Failure to make referrals to specialty care, such as physical or occupational therapy,176,178 were particularly problematic when help was needed to strategize practical needs like safely carrying, bathing, or feeding infants.
Social and interpersonal dimensions of pregnancy
Twenty-seven articles addressed social and interpersonal dimensions of pregnancy, with the majority using a qualitative study design with most having a moderate risk of bias. These studies were conducted across a broader range of regions and country incomes than other topics (see Table 3). Twenty-one articles addressed women’s desires for and fears around motherhood and factors influencing decision-making. While they have a similar desire for pregnancy as their non-disabled peers, greater ambivalence, uncertainty, and doubt was experienced by women with mixed physical disabilities and spina bifida.18,187,194 Factors influencing pregnancy decision-making included the importance of having a biological child, 194 length of experience with disease or its duration,49,195 the effects of the disability or disease on the course of pregnancy or functioning after delivery,10,54,187,195 –197concerns about the ability to care for a child,18,197 or burdening a partner 198 and child. 197 Societal attitudes about disability and negative perceptions about disability could also influence decision-making,9,10 although not all women felt that society’s views of family planning were negative. 199 Fears of passing on the disability to the child, warranted or not, also played a role in decision-making180,198,200 and the reactions of others to a pregnancy. 201 For women with cerebral palsy, greater impairment was associated with a lower desire to have children. 72 Women with SCI expressed fear and uncertainty around pregnancy, such as being pregnant and caring for a child. 63 Some women experienced worry and even despair when learning of their pregnancies. 18 In testing the efficacy of a pregnancy decision-making tool, women with MS had less decisional conflict and greater self-efficacy and knowledge about pregnancy and MS when using the tool compared to controls who did not use the tool. 202
Articles addressing the support and reactions of others to pregnancy or desire for a future pregnancy (n = 10) reflected a range of experiences, both positive and negative, from family, friends, and strangers. These tended to be negative or neutral compared to the experience of their non-disabled peers. 193 Family reactions often revolved around concern for the mother and the baby’s well-being, balanced by excitement and encouragement.9,18 Reactions from strangers could be similarly varied, ranging from curiosity and hostility to questioning parenting capability. 12 Reactions to a woman’s pregnancy can also be heavily influenced by cultural beliefs, 180 religion, 200 and traditions. 200
Women’s experiences of stigma and discrimination about pregnancy were not restricted to a global region or a country’s wealth or development.9,181,192 For some women, the negative reactions of others could be more limiting than the disability itself. 193 Women were generally realistic about the need for support from others to realize their desire to be mothers.18,190 While they depended on their families during pregnancy, 174 they also had to negotiate the balance of needing help and maintaining their parental role. 192
The experience of becoming and being a mother could be transformative and a positive experience (n = 5). The effect of disability on the ability to care for young children and the roles of mothers could be complex. While impediments to simple acts of caring for a child could be challenging, it also activated problem-solving and the use of strategies to take on a maternal role.203,204 For women with SCI, childbirth was a very positive experience that they would recommend to other women with SCI. 191 Being a mother also offered women a connection to other mothers in their community, creating a sense of belonging 194 and normalcy, especially in the way others have perceived them. 181 However, for some, there was a price exacted, with postpartum health problems, loss of function, and isolation. 204
Risk of bias assessment
The majority of studies (64%) in this review had a moderate risk of bias, with only 20% having a low risk of bias and the remaining (16%) having a high risk of bias. Studies in maternal care and social and interpersonal dimensions of pregnancy had the highest rates of moderate and low-risk studies. In contrast, the remaining topic areas were more distributed across risk ratings (see Table 3). In terms of study design, cross-sectional studies had the highest proportion of low risk of bias studies, and qualitative studies were well balanced between moderate and low risk of bias. In contrast, retrospective cohort studies fared the worst, with no low risk of bias studies represented in the review and a third of studies having a high risk of bias (see Table 3). In terms of factors driving bias ratings, most study designs had clear and focused objectives or study questions, clear outcomes, and justified conclusions. Deficiencies tended to aggregate around sampling issues and reporting, such as participant characteristics, the pool from which the sample was drawn, or accounting for dropouts. Other deficiencies in quantitative designs included a lack of reporting confidence intervals or accounting for confounders. For qualitative designs, the positionality of the researchers was notably absent in most studies with mixed ratings for the inclusion of theoretical frameworks. See Supplemental Table 2 for item-level details for each rating scheme.
Discussion
The goal of this scoping review was to characterize and synthesize the literature on pregnancy among women with physical disabilities, highlighting gaps in knowledge to inform recommendations for future research. The 171 studies in this review were conducted in 35 countries, predominantly in Europe and the Americas, with the vast majority in high-income countries. They were predominantly quantitative in design, using a variety of cross-sectional methodologies, mostly retrospective and prospective cohorts. These were complemented by qualitative studies that explored the experience of maternal care and the social and interpersonal dimensions of pregnancy. Most studies had a moderate risk of bias, with a minority of studies having a low risk of bias, highlighting the opportunity to improve the scientific rigor of the research. The thematic structure that emerged from our synthesis reflects key tenets of Mitra et al.’s 15 Perinatal Health Framework for women with physical disabilities by emphasizing the influence of personal, social, and structural factors on the experience and outcomes of pregnancy and the functional and physiological impacts of disabling conditions and injuries. Although more women with physical disabilities are pregnant each year, pregnancy rates remain lower than their non-disabled peers. In direct comparisons, rates of pregnancy loss were generally higher among cohorts of women with physical disabilities. For the general population, the prevalence of a single pregnancy loss is estimated to be 10.8%. 205 Our review suggests that rates of loss are quite variable across and within populations but generally above estimates for the general population. Understanding risk factors and how to mitigate the risk of pregnancy loss is important for future research to address. Rates of elective termination varied more widely by study and by sample, with most reviewed studies reporting higher rates of pregnancy termination than the most recent (2015–2019) global estimate of 3.9 terminations per 1000 pregnancies (or 0.0039%). 206
Rates of cesarean births were generally high for both women with physical disabilities and controls, with a number of non-significant comparisons to their non-disabled peers. This likely reflects the rising global rate of cesarean delivery, with an average of 21.1% and a projection of 28.5% by 2030. 207 Cesarean delivery may be medically indicated in many cases; however, the results of our review also highlight concerns of women with physical disabilities that this may be too quickly recommended by healthcare providers who may be uncomfortable or lack enough knowledge to weigh the risks and benefits of vaginal versus cesarean birth in such cases. This concern is compounded by the overmedicalization of pregnancy (e.g., unnecessary ultrasounds, non-medically indicated cesarean delivery or labor induction), particularly in developed countries. 208
Infant outcomes of pre-term birth were variable across studies and samples, although often higher among women with physical disabilities versus their peers. Similarly, rates of low-birth-weight infants varied across studies, pointing to an inconsistent relationship with physical disability. Contextual factors associated with adverse infant outcomes, such as being enrolled in public insurance, income, and employment status, are likely to amplify risks associated with disability, 209 which provides insights for understanding contextual factors that impact infant outcomes beyond disability. Our synthesis of the literature on interpersonal dimensions of maternal care and the social context of pregnancy for women with physical disabilities highlights the enduring effects of stigma and bias, both directly and indirectly, on the quality of maternal care. As our review shows, many women with physical disabilities experience being dismissed by healthcare providers, which is often compounded by a general lack of knowledge about pregnancy and disability. While negative experiences during pregnancy were not uniform for all women across reviewed studies, in general, they contended with negativity from healthcare providers, family, and strangers around pregnancy, potentially increasing the risk of mistreatment.
The social dimensions of pregnancy for women with physical disabilities are perhaps the most complex of the topics in this review. Women must consider many factors when deciding to pursue pregnancy and often do so in a setting of uncertainty with limited information to guide them. They are often confronted with hesitancy or outright rejection by healthcare providers and their families. While reactions to pregnancy could include the celebration by others, women often faced questions, skepticism, and doubt. But for many, becoming a mother was transformative and challenged them in ways that ultimately resulted in their growth as an individual.
Gaps in the current literature
Our review highlights several important gaps in the literature to guide future research. Preserving or rebuilding physical function during and after pregnancy can play an important role in decision-making about pregnancy. 210 However, studies of the effects of pregnancy on function were almost exclusively conducted in women with autoimmune disorders (i.e., MS and RA); of these, the focus was primarily on disease activity, such as relapse rates or other biomarkers. While these are critical factors that influence decision-making and maternal care practices for women with autoimmune disorders, and consistent with a 2021 systematic review and meta-analysis, 211 substantially far less attention has been paid to a broader range of disabling conditions or injuries and the impact of pregnancy on physical function. Given its critical importance to independence, infant care, and self-care, this is a significant gap warranting attention.
Perinatal depression is one of the most common and serious complications of pregnancy. 212 Women with physical disabilities may be especially vulnerable in pregnancy with an already elevated risk for depression. 213 Despite these elevated risks for mood disorders during pregnancy and the postpartum period and the serious consequences of undetected or untreated perinatal depression, our review shows that these issues were addressed and reported in only four studies.
Reasons for elective termination in reviewed studies were largely unexplored. In the general population, the reasons for seeking a termination are often complex and multi-factorial. 214 These include financial concerns, timing, and partner and other relationship-related reasons.215 –217 It is reasonable to presume these factors and others also play a role in decision-making among women with physical disabilities. For example, in the study with the highest rate of termination in this review, South Korean women with mixed physical disabilities cited similar reasons, including unplanned pregnancies, financial difficulties, poor health, and burdens of child-rearing. 18 Given the higher risks of unintended pregnancy among women with physical disabilities, 48 significantly more research is needed to understand factors that lead women with physical disabilities to seek elective termination and the outcomes of those decisions. More work is also needed to understand specific risks and mitigation strategies of pregnancy loss. Similarly, issues related to fertility, equitable access to treatment, and factors influencing decision-making were not addressed in the reviewed literature.
Recommendations for future research
The results of this comprehensive review point to opportunities to address gaps in knowledge and improve the experience and outcomes of pregnancy among women with physical disabilities. The recommendations offered here are not intended to be exhaustive but a starting point to coalesce efforts to move the field forward.
Recommendation 1 – Strengthen the evidence base to inform maternal care practices and develop interventions
One of the most important outcomes of this review is the identification of gaps in knowledge that must be addressed to inform maternal care practices and intervention development for this population of women. This includes understanding the short- and long-term impact of pregnancy and childbirth and determining effective strategies to mitigate these impacts on physical function and factors such as self-care, independence, and community living. Improving our understanding is a necessary foundation of interventions that strengthen capabilities to meet self-care and infant caregiving demands during pregnancy and in the postnatal period. There is also a need to understand the reasons women with physical disabilities seek termination of pregnancy and the role that disability plays, if any, in the decision-making process. There is an urgent need to examine the risk of perinatal and postpartum depression in women with physical disabilities and the extent to which disability plays a role in amplifying (or mitigating) risk.
Increasing the rigor of scientific studies is imperative for generating this robust evidence base. Our results suggest considerable room for improvement across study designs, with the majority of studies having a moderate or high risk of bias. The overreliance on p-values in the reviewed studies also highlights the need for increased rigor in reporting other statistical measures that reflect the magnitude of effects, as well as the meaning and relevance of results. Fortunately, many drivers of bias can be feasibly addressed by improving the reporting of sample characteristics, the reporting of confidence intervals and accounting for confounding variables, and the accounting for the positionality of researchers and theoretical frameworks in qualitative studies.
Recommendation 2 – Examine the effects of discrimination and stress on pregnancy outcomes among women with physical disabilities
The results of this review highlight the stress that women with physical disabilities often encounter during pregnancy. These are frequently related to navigating barriers to care, coping with the reactions of others, a lack of information to guide them, and not receiving evidence-informed care. However, there is limited research on understanding the impact of these experiences on the experience of pregnancy and outcomes. Literature on factors that mediate the association between race or ethnicity and maternal and infant outcomes increasingly points to the mediating role of stress associated with discrimination. 218 The potential role of allostatic load or the cumulative physiological effects of stress over the life course may help to explain disparities in pregnancy outcomes among women of color. 219 Disability discrimination is also associated with poorer well-being and psychological distress, 5 internalization of stigma,6,7 and can amplify health disparities. 8 In some world regions, identities other than race, such as caste or cultural beliefs, can drive discrimination.220 –222 Using an intersectional ecological framework that incorporates each identity, their intersections with one another, and their interaction with systems in which a woman lives 223 can help guide research to understand intersecting identities in the context of pregnancy among women with physical disabilities. The alarming lack of research at the intersection of mental health, pregnancy, and disability highlights a significant opportunity for future research to examine risk factors and treatment strategies to mitigate the risk of mental health disorders during and after pregnancy.
Recommendation 3 – Develop interventions to mitigate maternal care and pregnancy outcome inequities among women with physical disabilities
In this review, we did not identify a single intervention study that addressed the myriad challenges women with physical disabilities face in managing pregnancy, childbirth, and decrements in postpartum health and function. Despite gaps in evidence highlighted in this review, our results also point to decades of existing literature to inform the development and testing of interventions in the near future. For example, the reviewed literature highlights persistent challenges in navigating the social dimensions of pregnancy. This work can directly and immediately inform the development of interventions that support skill development, like self-advocacy, to empower women with physical disabilities to cope with these challenges effectively. Interventional research is also needed to develop strategies and clinical practices that improve maternal and fetal outcomes, enhance the quality of care, and promote equitable maternal healthcare access. In addition, this existing research can directly inform policy changes and training programs for healthcare providers.
Recommendation 4 – Increase disability competence and education of support of maternal care providers to improve access and quality of maternal care for women with physical disabilities
Accessible maternal care services are generally lacking, both in high- and low-income countries, with additional burdens in low-resource settings.184,224 Healthcare disparities among people with disabilities are increasingly recognized for their adverse effects on health and well-being, with ongoing challenges of access to care.225,226 These challenges burden both women with physical disabilities and healthcare providers. The results of our review underscore the importance of and need for improvements in the interpersonal aspects of maternal care for women with physical disabilities. Improving the cultural competence of healthcare providers is one approach to reducing health disparities. 227 Cultural competence in healthcare reflects the ability of a healthcare provider and organization to effectively deliver services that meet patients’ social, cultural, and linguistic needs. 228 While cultural competence has typically focused on racial and ethnic differences, more recently, it has expanded to include other vulnerable and marginalized groups, including people with disabilities.229,230 Studies on maternal care providers’ perspectives show that they struggle with ambivalence or discomfort, 24 limited competence in disability,24,231 and often must make decisions in a setting of uncertainty 232 without sufficient evidence 25 to guide their care. However, these healthcare providers also value an interprofessional network and collaboration24,231,232 to provide high-quality maternal care. Although not the focus of this review, healthcare providers also need support and education in providing high-quality maternal care to women with physical disabilities. As such, the development and testing of interventions to support them are also urgently needed. Moreover, improving the quality of and access to maternal healthcare that meets the needs of women with physical disabilities cannot be accomplished without the involvement of healthcare providers and healthcare systems. Understanding challenges from those perspectives is an essential next step in creating effective solutions.
Strengths and limitations
There are a number of strengths in our approach to this review, balanced by several significant limitations. We used three large databases to identify the literature, which was augmented by hand-searched reference lists. Multiple reviewers were involved in evaluating studies and were involved at all stages of the review. Independent reviewers conducted data extraction and critical appraisals, and discrepancies were rigorously reconciled. We did not limit the year or language of articles to only English, which helped mitigate the risk of missing relevant studies. We also critically appraised articles, which is not common in most scoping reviews. Using a variety of rating schemes that reflected the range of study designs and creating a common metric to compare the risk of bias across study designs and topic areas provided important information to guide future research. That said, as our protocol was developed for this review, it should be validated in future work.
While our broad search criteria necessitated considerable effort to review each potential article, casting a wide net and hand-searching reference lists of eligible articles enabled us to include a broad range of topics that may have been missed with narrower search criteria or keywords. We considered this to be an acceptable trade-off, given the ultimate purpose of the review and the complexity of the topic. However, this is not a guarantee that all relevant articles were captured, given our broad definition of “pregnancy.” Details within each article may not be represented entirely in each of the topics and sub-topics. Moreover, the breadth of the literature in this review limits the ability to draw definitive conclusions about a given topic, issue, or population. In fact, such efforts as we have undertaken here often produce more questions than answers.
Other factors that should be considered in interpreting the overall results of this review include the range of sample sizes across and within study designs. While smaller samples are typical for specific study designs, such as qualitative or case series, the wide range of sample sizes increases the likelihood of underpowered quantitative studies contributing to the interpretation of results. Another limitation relates to the predominance of p-values reported in the reviewed studies. p-values do not convey the size of an effect or the practical significance of an effect 233 ; however, many studies reported p-values as the only statistic, if any. p-values are also sensitive to sample size. Larger samples may yield small p-values for what are ultimately trivial effects, while smaller samples may not detect important effects simply due to lack of power. Ideally, p-values should be interpreted alongside other statistical measures, such as confidence intervals and effect sizes.
Despite such inherent limitations, the overarching goal of the review was to provide an overview of the current literature and sufficient information to guide readers to explore the articles more. Moreover, we offer a provisional and preliminary organizational structure of the major and subtopics of the body of literature on pregnancy and physical disability that future work can build on and improve.
With respect to generalizability, the majority of studies were conducted in Europe and the Americas, and high-income countries. While this is representative of the current literature, it is also an important caveat for generalizing findings to lower- and middle-income countries in other regions of the world. It is also a call to the field to support and promote efforts to reach women across the world to understand context-specific and both common and unique experiences in pregnancy. This is especially important given the higher rates of disability in childbearing years in lower-income countries. 3 Such efforts are also important because cultures are diverse in values and social structures, including motherhood, families, and family planning. Disability is inextricably linked to the context in which a person lives, including the culture and society as well as the physical environment. As such, a comprehensive understanding of contextual factors at the interface of disability and pregnancy – and ways in which structures can be changed to support women – can only be achieved with greater representativeness of world regions and cultures. Any review is limited by literature that is published after the final search date, and these results should be re-considered as new evidence emerges. Residual confounding, or factors that are not accounted for in statistical modeling, is a further caution considering the generalizability of results. In addition, the risk of bias should be taken into account when generalizing findings.
Our broad definition of physical disability enabled us to cast a wide net, including studies that may have been excluded with greater specificity of the cause of impairment. However, there is no universally accepted definition of “physical disability,” although reference to some impairment of mobility is generally accepted. Moreover, applying this definition to samples where physical disability was more inferred than explicitly stated leaves room for error. However, there is some precedent for including a range of disabling causes under the construct of a physical disability and discussions of pregnancy. 234 And, as with any scoping review, there is always the risk that we did not include all published articles meeting our inclusion criteria because of a broad definition of physical disability that could include a number of conditions and injuries. Our decision to include studies with a 50% threshold of stated physical disability or where there was an analysis within a sub-sample was also based on our judgment. Studies using claims data or other large datasets where definitions of disability do not distinguish types (i.e., physical, visual, hearing, cognitive) were excluded. Such a lack of distinction presumes that needs are uniform across the broad construct of “disability.” This limits the potential usefulness of these studies in informing solutions that are tailored to the nature of functional limitations associated with the type of disability. Nevertheless, our threshold of 50% may be overly strict. In contrast, conditions we included under the umbrella of physical disability may have been excessively generous or applied inconsistently despite our best efforts. As such, the efficacy of such methodological decisions should be tested and refined in future reviews.
In terms of representation of disability or disabling condition in the reviewed studies, it is not surprising that there were many articles focused on women with MS, given that it occurs predominantly in women and is diagnosed during the childbearing years. Although there is some risk of their overrepresentation in results, these articles almost exclusively focused on disease activity during and after pregnancy, with limited attention given to functional impairment and other dimensions of the pregnancy experience. This alone points to gaps in the literature addressing the needs of women with auto-immune conditions.
Conclusions
There is a rising call to action to enhance maternal care for all women and address the disparities in maternal health. Our review underscores the significant and persistent challenges that women with physical disabilities encounter on their journey to motherhood. However, there is cause for optimism. Since its inception in the mid-20th century, the body of literature on pregnancy and physical disability has grown steadily, showing no signs of slowing down. This review identifies several opportunities to build on this foundation by developing targeted interventions and clinical guidelines to support women with physical disabilities throughout pregnancy and in caring for their infants.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251338424 – Supplemental material for Pregnancy and physical disability: A scoping review
Supplemental material, sj-docx-1-whe-10.1177_17455057251338424 for Pregnancy and physical disability: A scoping review by Claire Z. Kalpakjian, Lukonde Mulenga, Shannen M. McIntosh, Jodi M. Kreschmer, Rebecca Parten, Heidi Haapala, Elizabeth S. Langen, Sara A. S. Rosenblum, Svati Pazhyanur, Susan Carlson, Maryam Berri and Susan D. Ernst in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251338424 – Supplemental material for Pregnancy and physical disability: A scoping review
Supplemental material, sj-docx-2-whe-10.1177_17455057251338424 for Pregnancy and physical disability: A scoping review by Claire Z. Kalpakjian, Lukonde Mulenga, Shannen M. McIntosh, Jodi M. Kreschmer, Rebecca Parten, Heidi Haapala, Elizabeth S. Langen, Sara A. S. Rosenblum, Svati Pazhyanur, Susan Carlson, Maryam Berri and Susan D. Ernst in Women’s Health
Supplemental Material
sj-xlsx-3-whe-10.1177_17455057251338424 – Supplemental material for Pregnancy and physical disability: A scoping review
Supplemental material, sj-xlsx-3-whe-10.1177_17455057251338424 for Pregnancy and physical disability: A scoping review by Claire Z. Kalpakjian, Lukonde Mulenga, Shannen M. McIntosh, Jodi M. Kreschmer, Rebecca Parten, Heidi Haapala, Elizabeth S. Langen, Sara A. S. Rosenblum, Svati Pazhyanur, Susan Carlson, Maryam Berri and Susan D. Ernst in Women’s Health
Footnotes
Acknowledgements
None.
Ethics approval and consent to participate
Because this is a scoping review of previously published research, no human subjects were involved in this review.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Eunice Kennedy Shriver National Institute of Child Health and Human Development (Grant no. R21 HD092526) and the Craig H. Neilsen Foundation (Grant no. 534511). The content is solely the responsibility of the authors and does not necessarily represent the views of the NIH or Craig H. Neilsen Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
All included articles in this review can be accessed online.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.