
Abstract
PURPOSE:
To identify key determinants of the quality of life of caregivers of infants and toddlers (
METHODS:
We conducted focus groups with providers for children who are DHH as well as interviews with hearing parents of infants and toddlers who are DHH. A multi-step qualitative analysis on interview data using grounded theory was performed, and an iterative analysis to investigate codes to characterize specific topics in caring for deaf infants and toddlers was conducted.
RESULTS:
Four focus groups (
CONCLUSIONS:
For hearing parents, the diagnosis of hearing loss requires changes in multiple domains of parenting. Support in each of these areas is critical for parents to restore a sense of equilibrium that is central to their quality of life. This framework provides a way to categorize parent experiences and may act as a template for focused interventions in the three identified domains.
Background
Hearing loss is among the most common birth conditions, with at least 1 in 500 newborns born deaf or hard-of-hearing [1]. The diagnosis of hearing loss in the already difficult post-partum period can be immensely challenging for the families of infants/toddlers who are deaf/hard-of-hearing (DHH). Approximately 90% of infants who are DHH are born to hearing parents [2], who have limited exposure to deafness and its management. Pressingly, in numerous studies parent stress is associated with poorer linguistic progress in the deaf or hard-of-hearing child [3, 4, 5], increased child behavior problems [6], and lower quality of the child’s self-esteem [7]. The early childhood period is a formative time for parental attachment and intimacy. Notably, there is evidence to suggest that early support and improved parental coping strategies during this time can ameliorate these negative outcomes [6]. Additionally, successful parent coping can improve the child’s emotional development [8, 9].
Multiple studies have focused on stress amongst the parents of children who are hard-of-hearing. Prior studies have used questionnaires like the Parenting Events/Daily Hassles scale and the Parental Stress Index to assess increased levels of stress in parents of children who are DHH compared to those of typically hearing children [6, 10, 11, 12]. Despite the a priori hypotheses predicting an increase in overall stress, the results have been decidedly mixed. Burger et al. [13] and Quittner et al. [14] found increased levels of parenting stress amongst the hearing parents of children who are DHH, while Lederberg and Goldbach [12] and Meadow-Orlans [11] did not find a difference in general parenting stress. In contrast, there was an increase in context-specific stress related to hearing loss observed [11, 12]. There has also been extensive research in the specific context of Early Hearing Detection and Intervention on the impact of age of DHH identification on parental stress. Despite early concern that universal newborn hearing screening might lead to increased parental stress and issues with bonding, the study conducted by Pipp-Siegel et al. [6] of all families in Colorado’s program suggests that there was no increase in parental stress associated with earlier age of identification of deafness or changes in maternal bonding and attachment [15].
Although prior studies have identified specific stressors facing caregivers of infants and toddlers who are DHH such as time pressure related to deadlines and decision-making difficulties, these results do not provide a comprehensive framework for explaining the parent experience [11, 12]. Other studies have identified variables such as personality [16], sense of coherence [17], acceptance [5], and self-efficacy [18] as having a role on reported levels of stress both in parents in general, parents of children with other special needs, and in parents of the deaf and hard-of-hearing. These studies all point to the importance of considering a multitude of factors beyond parental stress when evaluating an individual parent’s experience of raising a child.
Quality of life (QOL) is a multidimensional construct that includes both positive factors such as a sense of achievement and negative factors such as stress [19]. The World Health Organization defines QOL as “individuals’ perceptions of their position in life in the context of culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.” [20]. By addressing QOL in caregivers of children who are DHH, providers can maximize the appropriate treatment and developmental trajectory of their children. Two studies have examined the concept of family QOL which is “the overall degree to which family members’ needs are met, the extent to which family members enjoy their time together, and the extent to which they are able to do things that are important to them.” [21]. The naturalistic study by Jackson et al. [22] used interviews with 8 families to identify a wide range of themes that describe the impact of having a child who is DHH on the family. A questionnaire-based study examined family QOL using the Beach Center Family Quality of Life scale [21]. Both of these studies focused on the general childhood age range of less than 18 years; however, studies of older children may fail to capture the specific challenges of early development such as language acquisition. There has been little investigation of the factors influencing QOL specifically with parents of infants and toddlers who are DHH [23]. Only one study has focused on parents of infants and toddlers who are DHH [24] and this was in the specific context of Early Hearing Detection and Intervention (EHDI). Additionally, general studies of children with chronic diseases often do not frame QOL in terms of issues like language acquisition that are unique to infants and toddler children who are DHH [25].
In order to devise effective interventions to improve QOL in parents of children with deafness, a more nuanced understanding of both the positive and negative contributors to QOL must be obtained. Given the paucity of information on parent QOL in this critical period and the absence of a framework explaining their experiences, our objectives were to use a qualitative methodology to identify the key factors affecting the QOL of hearing parents of infants and toddlers (0–3 years) who are DHH. We sought to develop a theoretical framework for QOL for these parents. Our framework can then be used by pediatric health care providers and researchers to formulate early interventions and tools that can positively impact QOL for infants and toddlers who are DHH and their families.
Methods
Study design
We performed a qualitative study in the grounded theory tradition [26], using four focus groups with providers and six individual semi-structured interviews with parents (one interview was conducted with both parents present). Individual interviews were performed to attain greater detail into areas discussed in the focus group. Two researchers (D.C., N.V.) conducted focus groups and semi-structured interviews. Focus groups with providers were conducted because providers could draw upon their experiences working with many different parents. Focus groups lasted approximately 2 hours and individual semi-structured interviews lasted approximately 1 hour. All focus groups and interviews were conducted in office or hospital conference rooms. All sessions were audio recorded, transcribed by a professional service, and checked by the investigators for accuracy.
We provided a $25 gift card and parking validation to each parent who completed an interview. The study was approved by the University of California, San Francisco Institutional Review Board.
Participants and recruitment
Providers from our institution’s pediatric otolaryngology clinic, providers from an affiliated otolaryngology practice at another children’s hospital, and teachers and workers at a school for toddlers who are DHH were invited by email to a participate in focus groups held at these respective sites. Meeting dates were set and any available and interested providers were invited to attend.
Prospective patient families were identified by asking providers at a single University-based pediatric otolaryngology practice to review and identify patients who would meet study criteria. We included English-speaking, hearing parents of children up to the age of 36 months who had a permanent hearing loss (unilateral or bilateral). We excluded children with additional disabilities or global developmental delay. Parents were then contacted through the patient list by phone and email over a 4-month period and asked to participate in the study. All parents willing to participate in the study were included.
Interview guide
Both the focus groups and individual interviews used semi-structured interview guides to gain an understanding of the experiences of parents in caring for infants who are DHH and to assess the ways in which the diagnosis impacted the families. The initial focus group guide was developed by the study authors and iteratively modified after each session. The guide used for interviews was further developed based on information acquired from the focus groups with clinicians and educators. Interviews for the study included questions and probes to provide an understanding of (1) the initial diagnosis of hearing impairment and parental reactions to the diagnosis, (2) parenting experiences, (3) interactions with extended family and general public afterwards, and (4) the ways in which parents communicated with their children.
Focus group composition
Focus group composition
Parent and child demographics
*Bone anchored hearing aid
De-identified transcripts were entered into Dedoose, a qualitative coding software [27]. Data was analyzed in an iterative process beginning with open-coding of the initial transcripts by four investigators (N.V., S.G., M.O., D.C.) to develop the initial codes and categories. Two investigators (N.V. and S.G.) then performed focused coding of all data to further develop these categories. During focused coding, we added new codes, combined categories, and adjusted category definitions as transcripts were analyzed. Data collection continued until the categories were fully developed and demonstrated conceptual coherence around the notion of quality of life of parents of children who are DHH. Through team meetings of the entire study team and shared analytic memos, the research team reached a consensus on the construction of the major analytic categories and the development of the conceptual model. Finally, in the two subsequent focus groups – the first with a subset of providers from the initial focus group and the second with a new group of providers from an affiliated audiology and speech practice – we performed member checking of data [28]. Finally, the participants assisted with the development of the framework and affirmed the investigators’ interpretation of the developed framework. The two final focus groups did not reveal any new codes.
Exemplary quotes supporting major categories and subcategories
Exemplary quotes supporting major categories and subcategories
Demographics
Two initial focus groups were convened with participants from a range of care providers for children who are DHH (Table 1). We also interviewed 7 parents of young children from our clinical otolaryngology practice (Table 2). There were 18 participants in our two initial focus groups (Table 1). We interviewed 7 parents – 6 mothers and 1 father – across 6 families. All parents were typically hearing (Table 2). Children’s ages varied from 4 months to 24 months and included those with unilateral and bilateral losses along with a range of severities (Table 2).
Categories and theoretical code development
We identified three major categories that encompass the caregiver experience and constitute the three main roles that caregivers play: (1) being a parent (2) being a mediator (3) being a navigator (Fig. 1). Combined, these codes represent a construct “Search for Equilibrium”, whereby parents come to terms with their changed role in each of the three major codes discussed below. QOL is determined by the ability of the parents to achieve this personal sense of normalcy in their lives.
Theoretical framework diagram.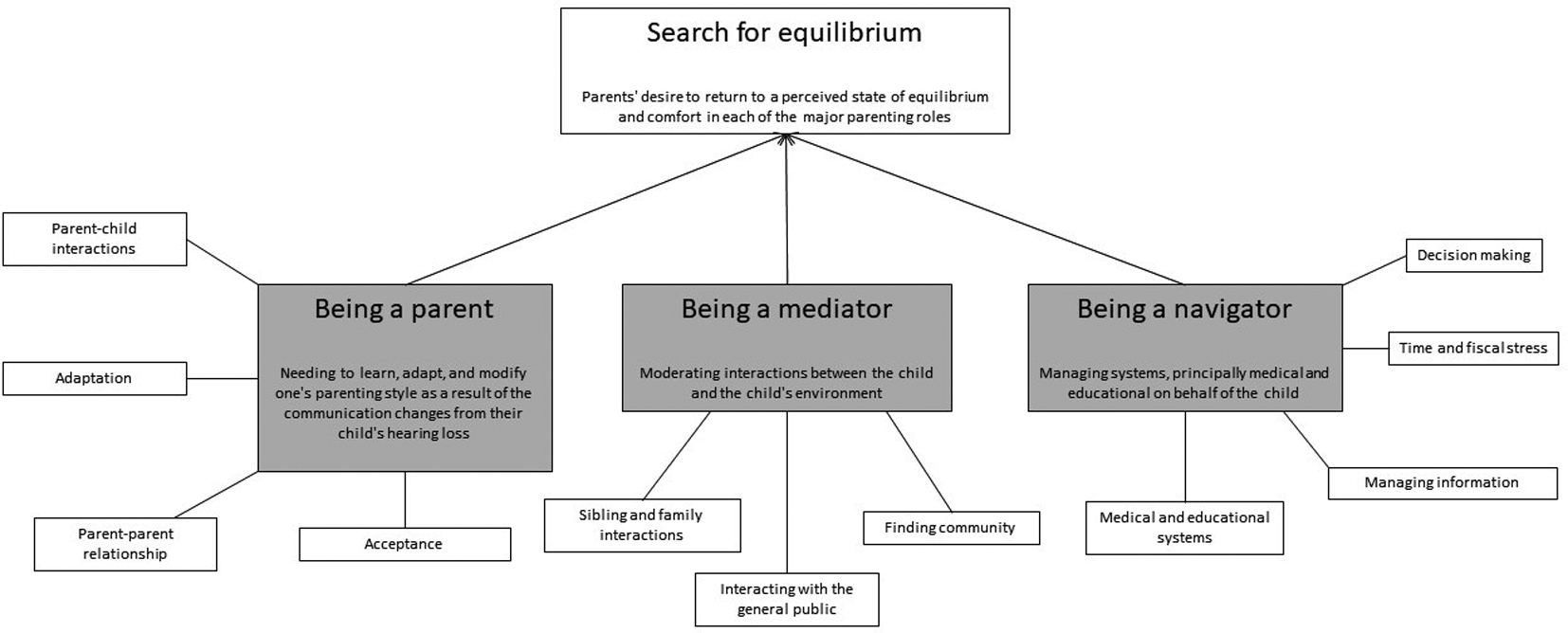
The area of most immediate concern for caregivers was their ability to be a parent (Table 3). The diagnosis of their child’s hearing loss often left parents second-guessing even the very basic elements of parenting. One early intervention home visit provider provided an example, “I used to go to see this mom. It was her first baby, first child. And, you know, as [program coordinator’s name] was saying, she just was overwhelmed and almost, you know – she told me years later that, “I had no idea what to do with this baby. I had no idea”
Providers expressed that parents often do not feel like they have any skill in the area of hearing loss, which can result in strained communication and decreased feelings of bonding between the parent and child. Parents expressed having to relearn, adapt, and modify their parenting style as a result of their child’s hearing loss. One parent explained, “I have to make a very conscious effort to talk out loud to her about the day and what’s going on and all these like different learning things. Like I would drive home and if I didn’t have to consciously remind myself, I won’t say anything to her the whole ride home. But I try and talk out loud.”
These adaptations often required extra attentiveness to ensure that the child received a rich exposure to language and interaction. Parents described having difficulty including their infant in social activities when compared to a hearing child. Furthermore, the degree of attentiveness such as talking out loud or ensuring that the child could see the parent’s face to provide additional sensory input often differs between the child’s two parents, resulting in stress in the parent-parent relationship. A teacher of infants and toddlers who are DHH related, “We’ve had a lot of that where the mom is the interpreter and she’s the only one who’s signing, or the dad, and then so there’s no direct communication between the one parent and the child. And then also feeling isolated because one parent is really competent and the other one isn’t that competent so there’s a disparity there.”
Eventually, many parents were able to adapt their own individual lifestyle and learned to interact with their child, though in a modified way from their pre-diagnosis conception. Developing a system of communication and learning skills for managing the child, whether with the help of early education experts or independently, was essential for arriving at a sense of routine in the parent-child relationship. Despite the challenges, many parents expressed positive experiences stemming from their parenting experience and a feeling of deep connectedness to their child. In describing this, one parent said, “I mean, it’s a little more difficult than having him not hearing and stuff but then it’s, you know, it’s a little more rewarding in a way. I mean, it’s just like you’re kind of learning a different thing and you’re, you know, you still learn your whole entire life, you know, and this is just something different that we have to learn and go through and figure it out.”
Being a mediator
The next realm of interaction was between the child, their environment, and the parent (Table 3). All parents serve as a “mediator” for their child regardless of disability or chronic condition. Parents acted as intermediaries between their child and the world their child encountered. The two broad classes of interactions were 1. Those between the child and family and 2. Those with the general public and strangers. Each of these situations had to be adapted to a child who is DHH, providing its own set of challenges.
Parents were often anxious to share the hearing loss diagnosis with their own parents (the child’s grandparents) out of fear for negative reactions. In some instances, family members reacted dismissively or with insensitive comments. One mother said, “Oh, it was like –it was a very touchy subject […] when I told my dad he said, “It’s not that bad. She has one ear.” And I kind of felt like “f*** you”’cause, you know, it’s just –I feel like my dad doesn’t know” In others, extended family members acted positively and supportively.
Families needed to ensure inclusion of their child in family interactions. Parents experienced anxiety as they tried to ensure that other family members were responsive to their child’s disability (e.g., turning down the TV, speaking one at a time). A provider in one focus group said, “[B]efore the holidays, you know, Thanksgiving or the winter holidays, families will talk to us about how hard it is to go to the family meal or the family get-togethers because people don’t know how to interact with their child or play with their child.” Both parents and family members who might provide childcare felt uncomfortable about being able to meet the communication needs of the child.
Similar stressors were found when interacting with the general public. Participants related having to field inappropriate and rude questions. Just as parents had to advocate for their child at family gatherings, so too did parents find they had to intervene when their child interacted with the public by explaining their child’s lack of response (Table 3). A parent described this situation, “I have to let people know that he does not hear well, you know, [you] need to talk louder. It’s different. You know, you have to be – I don’t know what the exact word would be. You just have to speak your voice, you know, to people to let them know that they might need to be doing something a little different.”
Not all interactions with the general public were negative; strangers could also be helpful and act as role models. Parents described feeling encouraged when they saw what they perceived as positive role models such as an adult wearing hearing aids or signing in public. Some parents felt more comfortable reaching out to adults who are DHH whom they had only known peripherally before. Through connecting to others in similar situations, parents sought to find a community for themselves and their child. Most parents derived a great deal of satisfaction from these interactions.
Being a navigator
The final role parents found themselves playing was as a navigator of a variety of unfamiliar systems (e.g., medical, insurance and educational services) (Table 3). Unlike in the previous domains, this role did not directly involve the child, although it had potentially major implications for the child’s development. As in other domains, parents faced a steep learning curve in understanding their child’s diagnosis and learning about all the services and items they had to address. Broadly speaking, these fell into two areas –educational and medical.
On the medical side, caregivers had to balance multiple appointments and tests, negotiate with insurance companies, and interact with health care providers. On the education side, parents similarly had to learn about the services offered and how to most effectively access these. Parents noted that both systems left little room for error and that mistakes in forms or meeting deadlines could lead to considerable delays in their child receiving crucial services. One parent described her challenges with school enrollment saying, “They [the school district] provide free preschool. And then at 3 years old they determine whether you are qualified for their pre-K. But if you don’t qualify then you’re off to your own devices but they only tell you this a month before your child turns 3. Meanwhile you missed all the application opportunities to any private schools’cause preschool’s all private here. I think that’s wrong too. Luckily I know the system so we’re already – I actually just turned in all the application to schools yesterday. But if I didn’t know, I’d be up a creek because you assume as a parent, [that] education, you know, equals everybody has a spot, right? But that’s not the case.”
Each of these areas could cause both time pressure and financial stress.
Providers also emphasized the stress brought on by making potentially life-altering decisions about hearing aids, surgical therapies (cochlear implant), and communication modalities, including sign language, with limited input from the child. One clinical provider explained, “[T]he families are pressured that they have to make the choice, it’s not like they can ask the child and say what do you think about a BAHA [bone anchored hearing aid], how are you hearing today. You know they’re always looking for these subtle cues whether its for an implant or a BAHA or what not. And I think that’s the hardest thing that they’re making a choice for this other individual and that they want to feel that they are making educated decisions.” Participants described a steep learning curve that accompanied the diagnosis which was exacerbated by the plethora of options for parents to choose from in areas ranging from the assistive hearing device to the modality of communication. As in previously described categories, parents were able to find support from early start teachers, clinical providers, and other parents who had been through similar situations. Parents gained skills in navigating these logistics over time.
Theoretical framework
Each of the major categories described above reflects a different set of interactions: “Being a parent” describes the interaction between the parent and child; “Being a mediator” describes how the parent, the child, and the child’s environment interact; finally, “Being a navigator” describes the parents’ interactions with the systems their child needs. Each of these roles is affected by the hearing loss diagnosis and in turn affects the QOL of the parents. Parents seek to restore balance to these areas of responsibility. Therefore, we generated the theoretical construct “Search for Equilibrium.” This concept represents the notion that having a child with hearing loss tends to take the parent away from their own preconceived notions of parenting and leads them to search for a new balance in their roles. This relativistic construction should be adapted to different cultural constructs, where “equilibrium” can be culturally specific and the parameters of the search in the three domains – being a parent, mediator, and navigator – are readjusted based on those cultural norms (Fig. 1).
As one social worker explained, “They need to learn how to navigate everything and that is way bigger than hearing loss. That’s why they say that eventually hearing loss becomes a normal part of their life but it’s learning to navigate this world that causes that emotional [stress] so you know identifying the stressors and helping them reduce the stressors would create that quality of life that we hope to achieve for these families.”
Discussion
Parents must adapt their perceptions and actions to achieve a feeling of balance. Each parent emphasized major categories differently, with some talking in depth about difficulties related to “being a navigator” while others focused on communication difficulties related to “being a parent” during the interview. The “Search for Equilibrium” is a process that varies over time as parents confront different obstacles as the child grows older. We anticipate being able to adapt our general framework and devise culturally specific modifications in the future.
This is one of the first studies to qualitatively explore the issue of QOL experienced by parents of infants and toddlers who are deaf or hard of hearing. Deafness is often considered a disability with one key characteristic being its invisibility [29]. Unlike many other disabilities, a child who is DHH is physiologically healthy but without support will be unable to fully interact with their surrounding world. Participant experiences coalesced into three key roles that were each affected by having an infant/toddler who is DHH. These roles represented the interactions between parent and child, between the parent, the child, and their environment, and between the parent (on behalf of the child) and other systems – principally medical and educational.
A great deal of literature has focused on specific stressors without looking at other factors that may influence QOL. Previous studies have identified the impact of deafness on a broad set of family-related areas including “emotional well-being, family interaction, parenting, physical well-being, and support for special needs” [30]. In addition to “parental stress, decision making, family interactions, and social networks” [22]. This paper’s model describes specific factors that underly concepts like “emotional well-being” and relates them to the major parenting experiences.
The major categories parallel findings from other qualitative inquiries such as the 2008 study published by Jackson et al. [22]. They identified themes of “decision making” and “support services” which correspond to the navigator role described by participants. Additionally, categories of parent-reported experiences of “increased bonding” and “parents as teachers” to describe the interactions between the parent and child are consistent with experiences noted by participants in this study. Reflecting this study’s focus on very young children (
The theoretical code “Search for Equilibrium” manifests itself in previous observations of diminished stress in mothers of children who are deaf or hard-of-hearing over time. Lederberg and Goldbach, in a longitudinal study using the Parenting Stress Index, found higher levels of stress at 22 months in mothers of children who are DHH compared to mothers of typically hearing children. However, this stress difference between the mothers of children who are DHH and children who are typically hearing disappeared by the time the children were 3 or 4 years old [12]. Although stress is just one component of QOL, these data indicate adaptation to the initial diagnosis which eventually results in decreased stress levels. Our theoretical framework potentially supports an approach that could address this difference and improve QOL through earlier intervention.
This framework, although devised in the context of hearing loss, also can be applied to other disorders of communication and to chronic conditions in general in this age group. Studies involving parents of children with a variety of disabilities have identified some overlapping themes and experiences. Resch et al. conducted focus groups with parents of children with disabilities ranging from muscular dystrophy to autism and identified 4 main barriers to parent well-being – access to information and services, financial barriers, school and community inclusion, and family support [31]. Similarly, in a broad literature review, Sullivan-Bolyai, et al. identified four main caregiving responsibilities: “managing the illness,” “coordinating resources”, “maintaining the family unit”, and “maintaining self.” [25]. These themes are similar to our categories of “being a navigator” and “being a parent.” Other studies on parents of children with autism spectrum disorder and children with cerebral palsy have found that these parents also face silent judgment and rude comments when out in public, similar to those reported by participants in our study [32, 33]. However, the domain of “being a mediator” contains unique elements to the role that have not previously been addressed in the literature. Specifically, this study identifies the unique challenge parents face of being interpreters for their children when interfacing with family and the general public. This finding is particularly relevant to disorders of communication such as hearing loss and other conditions such as autism. Although the focus is often on treating the medical condition, disabilities and diseases affect many other aspects of the family unit, including social, emotional, and psychological function. This framework can be used to compare hearing loss to other chronic diseases of childhood so broader lessons on chronic care management can be adapted and incorporated to assist families.
In addition, this approach takes an ecological framework towards hearing loss. Focusing on improving parents’ capacities in the mediation role has the potential to improve QOL and to decrease potential parent stressors. Further investigation using our framework may help guide tools and interventions that help parents improve their communication with their child, integrate in the community, and navigate medical and educational systems. Since parents have mentioned the importance of learning about other parents’ experiences [34], this framework provides one way for providers to organize their discussions with families. Providers who work with parents of children who are DHH should ask about the challenges of guiding interactions between the child and others. They should also provide support and strategies on how to handle these situations to support the role of “being a mediator.” As mentioned by one of our participants, parent support groups can also serve as a space for these discussions. Future research could identify strategies for supporting the child’s interactions with others. These changes could be of considerable benefit to both parent and child. Despite numerous programs designed to provide services for infants and toddlers who are DHH, parents are still often unaware of the services available or how to access them which suggests additional areas for improvement in care delivery.
Limitations
Interviews were limited to parents of children receiving care from a single medical center in the San Francisco Bay Area and may not represent experiences of families in other parts of the United States with differing socio-economic backgrounds. The sampling frame was based on a purposive sample of hearing parents and thus may not be generalizable to all DHH children, especially those raised by parents who are DHH. Providers told us that culture often impacts how the hearing loss is perceived, how family members react to the diagnosis, and how willing the caregivers are to accept and ask for resources [35]. Thus, future studies investigating the perspective of raising a child who is DHH with Deaf families/parents, ethnic minorities, and non-English speaking families will be performed to further evaluate the impact of cultural context with our findings. Information presented is based on self-reported experiences of participants, and thus interviews may not have captured all relevant categories or theoretical codes.
Conclusions
With early identification, parents are increasingly confronted with a hearing loss diagnosis early on in their parenting journey. The diagnosis affects every major area of the parent experience as it pushes parents away from their notions of normal in three main relational domains – as a parent, mediator, and navigator. Successfully navigating these challenges is critical for parents to achieve good QOL. Simply learning sign language or generating adaptive technologies does not fully address QOL for parents of infant and toddlers who are DHH. Our study provides an initial framework by which providers for infants and toddlers who are deaf/hard-of-hearing can understand these parents’ experiences and help them on their search for equilibrium for their families and their child.
Footnotes
Acknowledgments
The authors would like to thank Cimeran Kapur for her administrative support. This project was funded by the “Children’s Communication Center” grant by the Claire Giannini fund. The sponsor was not involved in the design, conduct, or reporting of the study.
Conflict of interest
The authors have no conflict of interest to report.