
Abstract
PURPOSE
: The purpose of this study is twofold: 1) to determine the age when a child with spina bifida (SB) will most likely transition from caregiver clean intermittent catheterization (CIC) to self-CIC, and 2) to identify factors associated with self-CIC in children older than that age.
METHODS
: This is a retrospective, single-institution cohort study of individuals with SB. Data were collected prospectively as part of the National Spina Bifida Patient Registry. For Aim 1, we identified all individuals who perform self-CIC and who had a documented transition from caregiver-CIC. We then determined the age of transition to self-CIC. For Aim 2, we compared individuals over age 10 years (age cutoff determined by Aim 1) who use self-CIC to those who use caregiver-CIC to determine what variables were associated with self-CIC.
RESULTS
: From our SB population, 206 individuals used self-CIC. Of these, 64 patients had
documented ages of transition from caregiver- to self-CIC. 46 (71.9%) and 56 (87.5%)
patients had transitioned to self-CIC by 10 and 14 years, respectively. For Aim 2, we
used age 10 as a cutoff, based on the findings from Aim 1, and found that 287/696
patients were
CONCLUSIONS
: The ages at self-CIC transition vary, although most patients transition by age 10. Thoracic-level spinal lesions and Medicaid insurance are associated with lower odds of self-CIC.
Introduction
Spina bifida (SB) is the most common non-chromosomal birth defect, with a prevalence of 30 per 100,000 live births [1]. There are an estimated 166,000 individuals with SB currently living in the United States [2, 3]. SB is associated with multi-organ disability, including Chiari II malformation, paraplegia, and neuropathic bowel and bladder [4, 5].
Effective bladder management is critical to prevent renal damage and promote social dryness [6, 7, 8, 9, 10, 11, 12]. While 90% of individuals with SB are born with normal renal function, 50% will deteriorate without treatment [6]. The deranged bladder dynamics may result in recurrent upper urinary tract infections (UTI) and/or renal scarring leading to end stage renal disease (ESRD) if untreated [12, 13, 14, 15, 16]. These sequelae can be reduced significantly with adequate bladder management [4, 9, 10, 11, 15, 16].
Since its introduction by Lapides, clean intermittent catheterization (CIC) remains an important part of management for many in this population [17]. CIC is a method of urinary elimination by which a sterile catheter is inserted into either a native or surgically-created urethra to drain the bladder. This process is repeated at scheduled intervals throughout the day by caregivers or patients in lieu of spontaneous voiding or chronic indwelling catheterization. Previous studies have found that urinary continence significantly improves self-concept in children compared to incontinence [18]. Urinary incontinence has also been cited as a major cause of lower psychological well-being, but has not been found to consistently reduce health-related quality of life (HR-QOL) scores among SB populations [19]. Urinary-related QOL (UR-QOL) may be significantly related to HR-QOL although no single factor that improves UR-QOL has been consistently identified [20]. Both social dependence and lack of compliance may impair effective bladder management in individuals with SB [21, 22]. We hypothesize that these individuals are more likely to perform self-CIC as they approach adolescence and those who are still dependent on caregiver-CIC in adolescence are likely to have higher spinal lesion levels, lower ambulation status, and male sex (due to anatomical differences).
We also hypothesized that after 10 years old, age would not play a significant role in CIC independence. This study has two distinct aims to address these hypotheses. Aim 1 is to determine the age at which individuals using CIC are likely to transition from caregiver- to self-CIC. Aim 2 is to identify factors that are associated with and contribute to CIC independence.
Materials and methods
Research setting
All patients with SB, including both open myelomeningocele (MMC) and other closed spinal dysraphisms (meningocele, spinal lipoma, split cord malformation, etc.) are seen at the authors’ multidisciplinary SB clinics. Those individuals under 21 years are seen in the pediatric SB clinic, and those over 21 years are seen in the adult SB clinic. All urologic management is performed by two pediatric and two adult urologists. Patients followed in either clinic are enrolled in the Centers for Disease Control (CDC) National Spina Bifida Patient Registry (NSBPR). A standardized questionnaire is used at the patient’s enrollment into the NSBPR to gather baseline demographic, diagnostic, and selected procedural information. An annual visit form is completed at enrollment and at each subsequent clinic visit; this form gathers updated clinical and demographic data to be entered into the NSBPR. Data entry involves a web-based electronic medical record (EMR) which provides a standardized method for data collection and management for all participating institutions. A subset of the data is de-identified, provided to the CDC, and available for query to researchers from all participating institutions (following an established protocol for data access). In addition, all data remain available locally through the institution’s research EMR. For the present study, only NSBPR data from the authors’ institution were collected and analyzed. For data points that may change with time (specifically self-versus caregiver-catheterization), the status at the most recent clinic follow up visit was recorded. The authors’ pediatric and adult clinics enroll more than 99% of all SB patients into the NSBPR, providing a robust research cohort with minimal missing data.
Patient selection for Aim 1 (left; age at transition to self-CIC; 64 patients) and
Aim 2 (right; factors associated with CIC independence; 287 patients).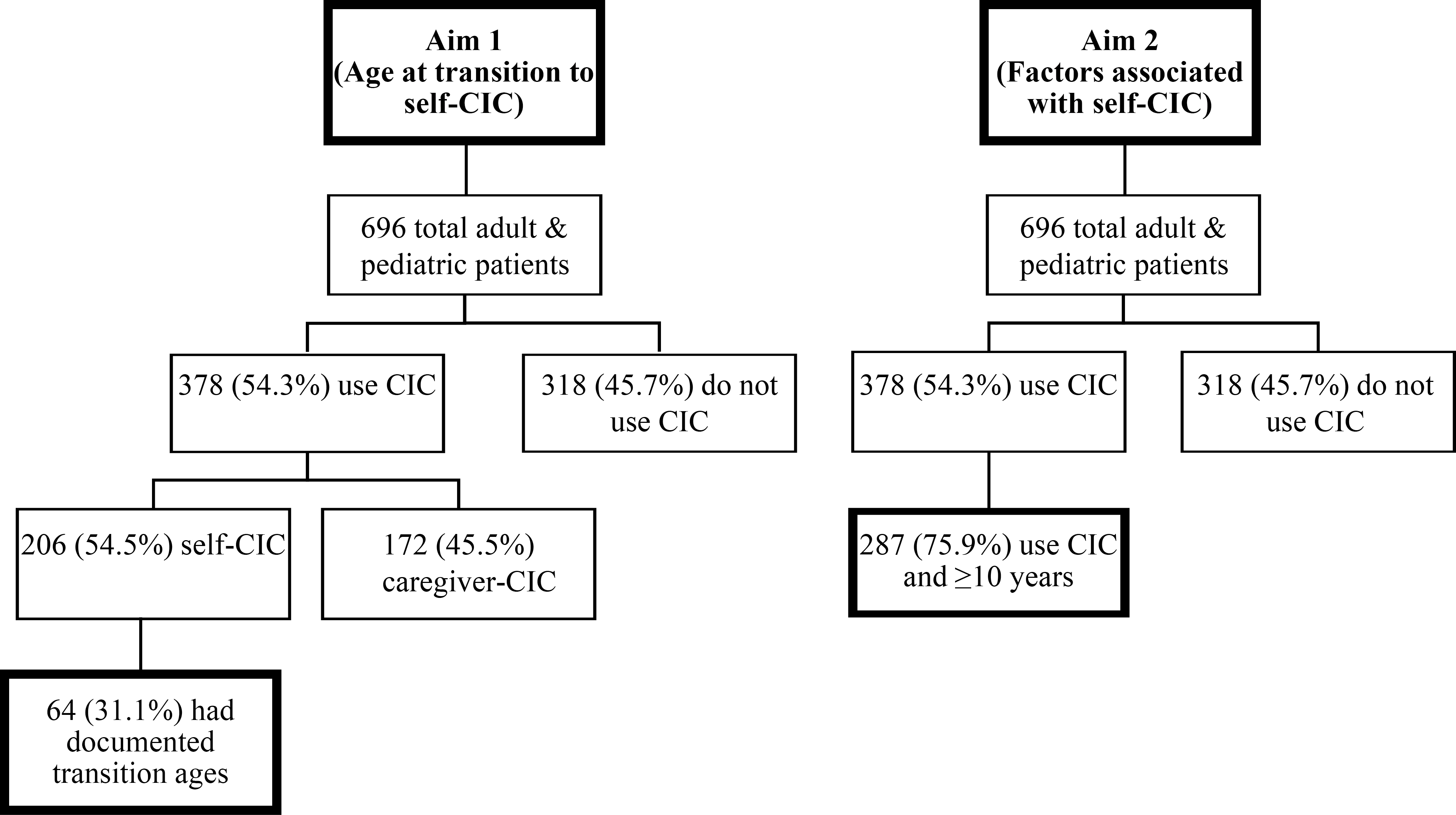
At each clinic visit, the patients and caregivers meet with the clinic coordinator who has reviewed the patient’s chart for any medical or surgical interventions since their last appointment. All information is reviewed with the patient and family to ensure accuracy and completeness of the record. Additionally, all urologic management medications and interventions are reviewed and updated in the NSBPR. When available, the age at CIC initiation and age at transition to self-CIC, if applicable, are recorded. Information about CIC dependence was collected at the last follow-up.
At all visits, patients meet with their urology provider and clinic care support staff to ensure compliance with CIC. All patients are screened for UTIs and undergo a renal ultrasound to assess for hydronephrosis, urinary tract stones, and other urinary abnormalities which suggest non-adherence to the CIC regimen. Prior to initiating CIC, all caregivers and patients are educated about the importance of the regimen and must adequately demonstrate the functional and mechanical capacity to perform CIC. At all visits, patients and caregivers on CIC are counseled on the importance of transition to independence. The concept of self-CIC is introduced to all patients of toilet-training age and emphasized at all subsequent clinic visits. Patients originally caregiver-dependent for CIC must successfully demonstrate self-CIC in the clinic to be considered “independent”.
After University of Alabama at Birmingham Institutional Review Board approval (protocol X090218005), the authors conducted a retrospective review of the records for all pediatric and adult patients at their institutions included in the NSBPR from 2009 until 2016. All patients performing CIC at any age were included in this study. Aim 1 of our study was to determine the age at which the majority of individuals with SB can be expected to transition to self-CIC. Figure 1 details the patient selection and population for determining the age at transition to self-CIC. For Aim 1, patients were excluded if they did not use CIC, did not have a documented age when beginning self-CIC, or began CIC independently without ever being caregiver-dependent. Sixty-four individuals met these inclusion criteria. Because these 64 patients represent only a fraction of total patients who use self-CIC (64/206), we compared the clinical and demographic characteristics between the 64 patients with documented transition ages and the remaining 142 patients who self-CIC but do not have recorded transition ages. The only significant difference between the groups via Pearson Chi-square analysis was community ambulation status. In the 64 patients with known ages at transition, 49/64 (76.5%) were community ambulators compared to 91/142 (64.1%) in the patients without documented ages of transition.
Aim 2 was to determine the social and disease-specific factors associated
with self-CIC in patients
Number of patients transitioning to self-CIC per year (columns) and total percent
of 64 patients having transitioned (line).
For both Aim 1 and Aim 2, the authors collected the following demographic information: gender, race, ethnicity, primary diagnosis, and Medicaid status. In addition to demographics, the authors collected the following variables for patients included for Aim 2: level of spinal lesion, ambulation status, wheelchair use, anti-muscarinic use, age at last follow-up, body mass index (BMI), history and number of ventriculoperitoneal (VP) shunts, and history and number of bladder augmentations.
Statistical analyses of the data were performed via IBM SPSS Version 25
software [25]. For Aim 2, univariate logistic
regression analysis was performed for all variables with the primary outcome of caregiver-
or self-CIC. To better assess independent predictors, those factors with univariate
significance of
Results
Age at transition (Aim 1)
Of a total 696 patients included in the NSBPR, 493 (70.8%) and 203 (29.2%) are followed in the pediatric and adult clinics, respectively. Of 696 patients, 378 (54.3%) use CIC for bladder management. Of these 378 patients, 206 (54.5%) were included in the self-CIC group. A total of 64 out of 206 (31.1%) patients had documented ages at transition from caregiver- to self-CIC and are the focus of Aim 1. The general data and clinical characteristics of the selected patients for Aim 1 are detailed in Table 1.
Demographic distribution and clinical characteristics of patients in Aim 1
Demographic distribution and clinical characteristics of patients in Aim 1
The median age at the last follow-up for the 64 included patients was 18.3
years (interquartile range (IQR) 14.5–20.9 years). The median follow-up after attaining
CIC independence was 7.0 years (IQR 5.3–10.6 years). The ages at transition to self-CIC
were collected, and the frequencies of transition by ages are depicted in Fig. 2. Based on these data, 8/64 (12.5%)
patients transitioned to self-CIC at or before 5 years of age. By 10 and 14 years, 46/64
(71.9%) and 56/64 (87.5%) patients were independent in CIC, respectively. The median and
mean ages of transition were 9 and 9.7 years, respectively. The greatest frequency of
transition occurred at 9 years with 11/64 (17.2%) patients beginning self-CIC. Visual
inspection of the data (Fig. 2)
shows a marked decline in self-CIC transition after age 10 years. Therefore, we defined
From Aim 1, 71.9% of the patients who use CIC transitioned to self-CIC by
age 10 years. For Aim 2, the authors used 10 years as a threshold beyond which the
majority of patients might be expected to self-CIC. From Fig. 2, the number of patients becoming independent in CIC
after age 10 years decreases in frequency. Of 696 total patients included in the NSBPR,
287 (41.2%) void via CIC and were
Demographic distribution and clinical characteristics of patients in Aim 2
Demographic distribution and clinical characteristics of patients in Aim 2
For Aim 2, the median age at the last follow-up for the 287 patients included in the analysis was 20.1 years (IQR 15.8–26.6 years). In this group, 123 (42.9%) were male, and 178 (62.0%) had Medicaid insurance. The number of patients that self-CIC and the number that are caregiver-dependent are 175 (61.0%) and 112 (39.0%), respectively. Univariate logistic regression and subsequent forced entry multivariable regression analyses are shown in Table 3.
By univariate analysis, gender, Medicaid insurance, thoracic level spinal
lesions, wheelchair use, history of VP shunt, and number of VP shunts were significantly
associated with self-CIC (
Factors associated with self-CIC: Univariate and forced entry multivariable regression
CIC remains the gold standard for bladder management in patients with spina bifida and spinal dysraphisms [17]. The authors’ multidisciplinary pediatric and adult SB clinics follow a proactive approach for the bladder management. Similar to other clinics, the authors emphasize the importance of caregiver-CIC initiation and daily anticholinergic prophylaxis starting at a young age when necessary. Caregivers initially perform CIC until the patients become physically and intellectually able to execute it independently [23, 24]. To our knowledge, no studies have yet been performed to evaluate the transition from caregiver- to self-CIC. Previous studies have documented the importance of transitioning to self-CIC and preserving continence for both the promotion of quality of life and independence [26, 27].
In a series of 44 patients, Seth et al. determined that the majority (73%) of patients experienced at least one barrier to self-CIC adherence. While lack of public toilet access was cited as the most common barrier (34%), difficulty positioning for catheter insertion and problems with dexterity were present in 25% and 21% of patients, respectively. Eighteen percent of patients cited supply cost as an additional obstacle for CIC adherence [22]. This study demonstrated the wide range of potential barriers to maintaining self-CIC which may also contribute to the initial transition to CIC independence. The data available in the present study do not allow for analysis of these social and cultural barriers.
Recently, Castillo et al. described their experience with 110 patients
transitioning to independent-CIC [28]. They found
that patients were capable of self-CIC between 2–17 years with a mean age of 9.45 years at
independence. Castillo et al. determined that male gender was associated with a higher rate
of CIC independence, and thoracic-level spinal lesions were associated with a lower rate of
independence. In patients
The present study identified a slightly broader range of ages at transition from 2–24 years and found that almost 13% of the patient population was capable of independent CIC by five years. Our study found that the majority of individuals achieve independent CIC between the ages of 9–14, which may correspond to increasing manual dexterity and desire to become more autonomous. Transition during the peri-pubertal years of 9–14 may also be linked to burgeoning social independence. In addition to establishing the average age of self-CIC, we determined which factors are associated with self-CIC. Patients with thoracic level spinal lesions had lower odds of self-CIC, which is consistent with Castillo et al. [28].
In another study, which reviewed the association of mobility and level of lesion, Schoenmakers et al. determined that individuals with lesions below L3 had greater functional independence with self-care and mobility. This study also found that mobility independence (OR 5.3, 95% CI 1.6–17.4) was the most important determinant of health-related quality of life [21]. It is known that individuals with higher-level spinal lesions tend to have greater functional and ambulatory impairment [29]. However, in the current study cohort, the authors found that neither ambulation status nor wheelchair use was an independent predictor of CIC independence.
Individuals with Medicaid insurance had lower odds of self-CIC, but the exact association between insurance status and CIC independence is difficult to identify. As a surrogate for socioeconomic status, families with Medicaid may represent disparities in resource availability or social support. However, given that Medicaid insurance provides the same monthly allocation of CIC supplies as private insurers at the authors’ institution, factors other than financial limitations may play a role in transition to CIC independence. Medicaid insurance status may also highlight disparities in health literacy and educational levels of caregivers which may contribute to CIC dependence. A 2015 multi-institutional study of SB outcomes found non-Hispanic black patients were least likely to have urinary and bowel continence and patients with private insurance were more likely to attain continence than those without private insurance [30]. While our study did not find race or ethnicity to be associated with CIC independence, this may be in part to the relatively small number of non-white subjects (15.6%) in our study. The disparity between CIC independence in patients with and without private insurance most likely represents an inequality among employment, income, and/or community resources between the two groups. Further studies are needed to delineate the roles that patients and their caregivers on Medicaid insurance have in CIC independence.
Interestingly, this study did not find any modifiable risk factors independently associated with self-CIC. BMI and anti-muscarinic use were not associated with self-CIC. This suggests that urinary independence among SB patients is most influenced by socioeconomic and anatomic factors. Primary diagnosis was not significantly associated with the self-CIC transition, which suggests that disease etiology does not contribute to independence, as may be expected [21]. However, only 25 (8.7%) non-MMC patients were included in the analysis, which may be too small of a sample to accurately evaluate the contribution that primary diagnosis has to CIC independence. These results will help the multidisciplinary spina bifida clinic better understand the limitations to self-CIC and to provide more focused patient education to those patients who are approaching an age of potential independence. Furthermore, this study will help recognize individuals with lower odds of self-CIC, and will enable clinics to allocate more resources to these patients and ultimately facilitate their functional independence.
The lack of association between age at the last follow-up and self-CIC shown in this study is key for the promotion of CIC independence. Once patients cross the “threshold” of age 10 years, it becomes increasingly important to address the socioeconomic factors which may limit self-CIC instead of assuming that individuals will become independent if given more time.
Limitations
The authors acknowledge the limitations of this study. This is a retrospective study at a single institution, subject to its inherent design deficiencies. Data regarding the age of transition from caregiver to self-CIC were not collected prospectively, and since the analysis the authors have added this subject as an additional field to our NSBPR data collection form. Recollection bias is possible, since the information on age of transition was based on caregiver response. Regional and cultural differences could influence the results, and single center studies are prone to treatment/management biases compared to other centers. The relationships between bowel and urinary management and outcomes were not studied, all of which are interrelated on many domains of independence and social continence. Data regarding CIC through a surgical or native urethra were not consistently reported in the NSBPR. While a surgical urethra may indeed facilitate self-CIC, we are currently unable to reliably include this in our analysis. A future study could investigate the role that a catheterizable channel has in self-CIC. Several other unincluded family, caregiver or even patient related factors could influence the results. A source of bias in this study may be the small number of patients (64/206, 31%) with a known age at transition to self-CIC. These data were not initially entered into the NSBPR at our institution. It was queried separately from the annual clinic questionnaire; therefore, the data were not consistently collected for all patients who self-CIC. Given the small sample of available data, the 64 patients may not represent a completely accurate sample of the 206 patients who use self-CIC. However, in comparing the characteristics of included patients with those who did not have a documented time of transition, only community ambulation was significantly different. This may limit the generalizability of the findings, but given that all other differences were insignificant, the authors believe that the findings are a reasonable representation of the population. Another potential confounder related to CIC independence may be the cognitive abilities of the patient. Data regarding cognitive function of patients and their current grade level are not currently included in the NSBPR. Additionally, the NSBPR does not contain data concerning parental education level, health literacy, or occupation, so we used insurance status as a proxy for socioeconomic status.
In spite of the limitations, this study addresses some critical aspects of understanding this patient population in more depth regarding functional independence for bladder management. To the authors’ knowledge, this is the first study that attempts to identify the age at transition as well as the factors associated with functional independence in bladder management. The future goal is to combine the CDC data from all the participating institutions to assess both the age and factors associated with self-CIC across other high-volume centers. This future study will include a wider geographic distribution, a larger sample size with different practice patterns, and will help to understand the complex nature of the disease and many interrelated variables.
Conclusion
Based on these results, individuals with spina bifida achieve functional independence with bladder management anytime between toddlerhood and adulthood (2 to 24 years of age). The majority of patients transition to self-CIC during the peri-pubertal period of 9–14 years (Fig. 2). Non-modifiable factors such as gender, MMC diagnosis, wheelchair use, history and number of VP shunts were associated with lack of CIC independence by univariate analysis. Thoracic-level spinal lesions and Medicaid insurances status were independent factors associated with lower odds of self-CIC by multivariable analysis. Age at the last follow-up was not significantly associated with self-CIC for patients greater than age 10. Further studies are needed at a multi-institutional level to better determine other factors that are associated with CIC independence.
Footnotes
Acknowledgments
This project was supported in part by NIH grant 1KL2TR001419, and by the KPRI of Children’s of Alabama.
Conflict of interest
One author (TSW) of this publication is the principal investigator for Ipsen
Innovation