
Abstract
PURPOSE:
To assess the interrater reliability, construct validity and usability of the Eating and Drinking Ability Classification System (EDACS) among Dutch children with Cerebral Palsy (CP) when used by speech and language therapists (SLTs) familiar and unfamiliar with the child’s eating and drinking performance and parents.
METHODS:
Translation was undertaken using the method of Eremenco. Agreement between SLTs and parents when using EDACS was determined by intraclass correlation coefficient (ICC) and linear weighted Kappa (
RESULTS:
Thirty-one SLTs classified 149 children (67 girls; mean 10 y, SD 4 y, range 3–21 y) with EDACS. Pairs of SLTs showed good agreement ([ICC]
CONCLUSION:
The Dutch version of EDACS is reliable and valid, and can be used easily by (familiar and unfamiliar) SLTs and parents of children with CP. Parents and professionals showed a high level of consistency when classifying eating and drinking abilities. EDACS enables uniform and efficient communication about safety and efficiency of functional eating and drinking ability in clinical and research contexts.
Keywords
Introduction
Cerebral palsy (CP) is a common neurological development disorder with a worldwide prevalence of approximately 2–2.5 per 1,000 live births [1]. People with CP suffer from a range of activity limitations arising from disorders of movement and accompanying disturbances of sensation, perception, cognition, communication and behaviour. Impairments of movement, sensation and posture can limit oral skills required for speech, eating, drinking and swallowing. Bulbar and oral movement difficulties, that may lead to problems with eating and drinking, are common in individuals with CP [2]. International prevalence estimates range from 27–99%, depending on the study population and measures of eating and drinking ability adopted [3, 4, 5].
It is often assumed that there is a significant correlation of oral motor dysfunction affecting speech, eating, drinking and swallowing with the severity of limitations to gross motor function and mobility [2, 3, 6, 7, 8]. According to the Dysphagia Disorders Survey (DDS) [9], Calis et al. [5]. found a 99% prevalence of dysphagia in a group of Dutch children with a GMFCS level IV or V and an IQ
Valid and reliable systems are available to classify specific aspects of everyday function in people with CP on the basis of their self-initiated movement (Gross Motor Function Classification System, GMFCS) [12], manual ability (Manual Ability Classification System, MACS) [13], and communication ability (Communication Function Classification System, CFCS) [14, 15]. All systems look at achievements rather than deficits and each classification system describes “performance” (people’s usual activity) in five ordinal levels, rather than “capacity” (what people can do at their best). None of these systems is a performance test or even a diagnostic tool. These systems enable clinicians to communicate with families and other professionals in a uniform way about the child’s functional abilities [15].
In their systematic review, Sellers et al. identified 15 ordinal scales used to classify eating impairments in children with CP [16]; however, none met agreed quality standards of health measurement scales [17, 18]. In response to this identified gap in knowledge, a new Eating and Drinking Ability Classification System (EDACS) was developed in the UK [19] with input from all stakeholders including expert professionals, people with CP and parents. This system consists of an extensive manual and an algorithm, both necessary for sufficient comprehension of eating and drinking abilities. It was designed analogous to other functional classification systems for people with CP (e.g. GMFCS, MACS and CFCS). EDACS can be used to classify how children and young people with CP eat and drink in everyday life using distinctions that are meaningful (Italics show the official wordings as stated in the manual itself) [20]. EDACS identifies key features of safety (choking and risk of aspiration), and efficiency (time taken and loss of food from the mouth) linked with limitations to eating and drinking ability. Five distinct levels of ability are described in an ordinal scale ranging from Level I “eats and drinks safely and efficiently” to Level V “unable to eat and drink safely” (Fig. 1, the summarized algorithm). Degree of assistance required to bring food and drink to the mouth is described in a separate three level ordinal scale: “Independent”, “Requires Assistance” and “Totally Dependent”. The interrater reliability of EDACS met recognized quality standards when used by pairs of Speech and Language Therapists (SLTs) (
Clinical algorithm EDACS.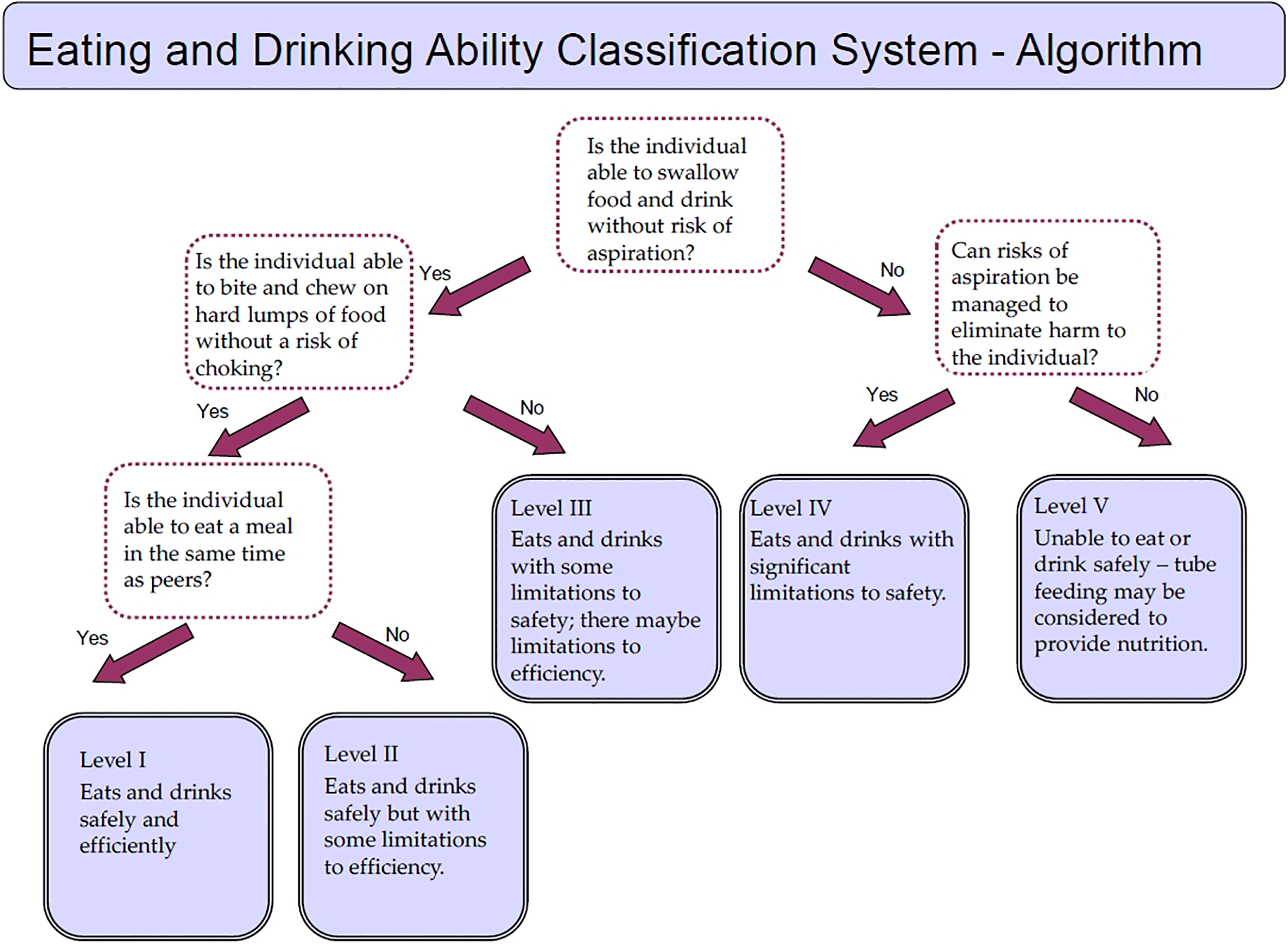
Sellers et al. also investigated the interrater reliability between parents and SLTs in order to examine the relationship between their respective viewpoints. By inviting parents to classify their children’s abilities, it is possible that parents will feel empowered and that their opinions matter [21]. Differences of opinion can form the basis of discussion about the most applicable EDACS level with the recognition that parents will have better knowledge than professionals of their child’s eating and drinking abilities across a range of situations and environments. There is evidence that parents can be reliable partners in classifying their child’s functional status [15].
The objectives of this study were (1) to translate the EDACS into Dutch by a validated translation method, (2) to examine the interrater reliability of the translated EDACS among SLTs for a cohort of Dutch children and young people with CP, (3) to investigate interrater reliability between SLTs and parents in the same cohort, (4) to assess the usability of the Dutch EDACS by SLTs and parents, and (5) to examine association between the EDACS and the Dysphagia Management Staging Scale (DMSS) [9], the GMFCS, CFCS, and MACS to determine its construct validity. A strong association was hypothesized for the DMSS in contrast to a moderate association for the other classification systems. The DMSS is a five-level ordinal scale used to classify severity of feeding and swallowing problems based on management needs and health related outcomes. It is used in conjunction with the DDS as a screening and clinical assessment of swallowing and feeding function for eating and drinking in people with developmental disability [9].
The development of the Dutch version of EDACS involved two distinct phases. The first phase consisted of translation of EDACS into Dutch. The second study phase consisted of investigating reliability, validity and usability of this Dutch version of EDACS. Written informed consent was obtained from the parents (or caregivers) and participating SLTs. This research was conducted in accordance with national and international ethics standards. The study was submitted to the Regional Hospital Human Ethics committee (registration number 2013–530).
Phase 1: Translation of the English EDACS into Dutch
First, a literature search by PUBMED on methods used to translate medical classification systems was conducted. Translation was undertaken using the method of Eremenco et al. [21] because it was considered to be thorough, practical, affordable, and used by other research groups in children’s rehabilitation. The method was applied in the following steps: (1) two forward translations were undertaken by a qualified translator with medical background and one without medical background (whose native language was Dutch), (2) one version combining both translations was agreed on by both translators, (3) one backward translation was created by a qualified translator with native English, (4) three reviewers (PJ, DSn and KvH) with expert knowledge of limitations of eating and drinking associated with CP reviewed the translation process and made adjustments, (5) the English member of the research group (DSe) reviewed and made adjustments to the backward translation, and (6) final adjustments were made by the Dutch members of the research group. The Dutch version of EDACS with a clinical algorithm can be downloaded from the website: www.EDACS.org.
Phase 2: Reliability, validity and usability study
Participants
Only participants (SLTs) of the last five curricula of the Pediatric Neurorehabilitation Cerebral Palsy course in the Netherlands, still working with children with CP were selected and invited to take part in the study. All SLTs were recruited by email. As recommended by Palisano et al. [12], the SLTs were trained in using EDACS, by attending a single 3-hour training session. The training session was provided by KvH, DSn and CE. This meeting consisted of an introduction to EDACS, an explanation of the manual, and a practice session using EDACS to classify function from video recordings of four children and young people with CP whilst eating and drinking. Parents received the EDACS user manual and a separate glossary by post and were invited to participate and classify their children’s eating and drinking abilities using EDACS.
SLTs were asked to recruit and classify three to five children who were attending special schools and rehabilitation centers. The following inclusion criteria were: age between 3 to 21 years, diagnosis of CP, and no intercurrent illness (e.g. cold or flu) at the time of rating. Two “mealtimes” (lunch and snack) were observed at the same day to observe the child’s abilities.
To include a heterogeneous group of children, it was not necessary to have established eating and drinking difficulties. Demographic information was collected from the medical record, including age, sex, CP subtype, GMFCS level, MACS level, CFCS level, and source of nutrition (tube, oral or combination). Table 1 shows the characteristics of 150 children with CP and 31 SLTs participating in this study.
Demographics of participants included in the reliability study
Demographics of participants included in the reliability study
The reliability study was designed to reflect typical practice within the Dutch healthcare system. Rehabilitation teams, in the Netherlands, usually have only one SLT engaged in the treatment of a child with CP. Typically the SLT has sole knowledge of the child’s eating and drinking abilities.
In this study, we evaluate the differences in scoring between pairs of two SLTs. For the interrater study the SLTs (
All participating SLTs and parents independently classified the usual eating and drinking performance of the children with CP on EDACS. They also determined the degree of assistance required. SLTs-2 visited the children in the rehabilitation setting or special needs school they were attending. Two mealtimes (morning snack, lunchtime) were observed on the same day and all SLTs obtained access to the children’s health histories. They observed the eating and drinking abilities ‘live’ (
SLTs’ and parents’ opinions about the usability of EDACS were assessed by four questions. Both SLTs and parents were asked to rate the clarity of level descriptions and of level distinctions using a four-point scale: ‘outstanding’, ‘good’, ‘moderate’, or ‘bad’. Also, they were asked to rate how easy it was to use EDACS using a three-point scale: ‘easy’, ‘neutral’, or ‘difficult’. Finally SLTs and parents were asked about the time needed to complete the EDACS (in minutes). All questionnaires were distributed and collected by a gatekeeper.
To determine the construct validity of EDACS, SLTs also classified children using one of the five levels of the DMSS. The DMSS consists of variables selected because they are sensitive indicators of the presence and functional adequacy of swallowing and feeding disorders in people with developmental disabilities. The level of the DMSS was determined by observation and on the basis of available medical information [9].
Statistical analysis
Interrater reliability was analyzed using Intraclass Correlation Coefficient (ICC) with a two-way random model for absolute agreement (single measure) and by linear weighted kappa (
The associations of EDACS level with degree of assistance required, as well as with DMSS, GMFCS, CFCS, and MACS, were calculated using Kendall’s tau-b. Descriptive analysis was used to report the usability of the EDACS system. Missing values were considered as missing at random. For all statistical tests, the level of significance for two-tailed
Interrater reliability measures with use of EDACS by SLTs (
31). (a) Reliability of EDACS levels I-V, SLT-1 versus SLT-2. (b) Reliability of degree of assistance needed, SLT-1 versus SLT-2
Interrater reliability measures with use of EDACS by SLTs (
SLT-1, Speech and Language Therapist familiar with the child; SLT-2, Speech and Language Therapist unfamiliar with the child. (a) ICC 0.84, 95% CI 0.79–0.88. (b) ICC 0.85, 95% CI 0.80–0.89. The grey boxes represent absolute agreement.
Interrater reliability measures with use of EDACS by SLTs (a) Reliability of EDACS levels I–V, SLT-1 (
EDACS, Eating and Drinking Ability Classification System; SLT-1, Speech and Language Therapist familiar with the child. (a) ICC 0.80, 95% CI 0.71–0.87. (b) ICC 0.77, 95% CI 0.66–0.84. The grey boxes represent absolute agreement.
Participants
An invitation to participate was sent by email to SLTs who met the inclusion criteria to participate in the initial meeting for the study (approximately 80 SLTs). Thirty-one of the 38 SLTs who attended this initial meeting agreed to participate. In 16% of the cases, the familiar SLTs knew the child’s eating and drinking abilities through group therapy; in the remaining cases, the familiar SLTs knew the child’s abilities from individual therapy in the past or present.
Reliability
The level of agreement between SLTs-1 and SLTs-2 was excellent. They agreed on EDACS level in 96 out of 149 children (ICC 0.84; 95% CI 0.79–0.88;
Eighty-one children (54%) were rated by their parents and SLTs for EDACS level, and 82 children (55%) were categorized on degree of assistance needed (see Table 3). The level of agreement was 0.80 (95% CI 0.71–0.87;
Validity
There was a significant and positive correlation between EDACS level and degree of assistance required for eating and drinking (Kendall’s tau-b 0.69,
Usability
SLTs and parents were asked to judge the usability of EDACS. The questions assessing usability of EDACS showed that 23% of the EDACS classifications made by SLTs-1 and 2 (70/300) were categorized as ‘outstanding’ regarding the understanding of the user instructions, 73% (220/300) were categorized as ‘good’ and 3% (10/300) as ‘moderate’. Of the parents, 30% (24/81) understood the instructions ‘outstanding’, 65% (53/81) ‘good’, 3% (2/81) ‘moderate’, and 3% (2/81) ‘bad’. When the SLTs classified an unfamiliar child, in 34–39% of the cases, the SLTs considered choosing between levels to be ‘easy’, in 49–51% of the cases ‘neutral’, and in 10–14% of the cases ‘difficult’. In two cases, the SLTs did not answer this question. Similar to these results, 47% percent of the parents thought choosing between levels to be ‘easy’, 43% found it ‘neutral’, and 10% found it ‘difficult’. The mean time needed to classify a child on the EDACS was 13 minutes for SLTs-1 (SD 7.9 range 1–30), 15 minutes for SLTs-2 (SD 8.9 range 2–60), and 16 minutes for parents (SD 8.1 range 1–35).
Discussion
The content of EDACS has been successfully translated into Dutch following a thorough, validated translation process. The key features of safety and efficiency of eating and drinking ability expressed in five distinct levels were considered meaningful and feasible by parents and SLTs working within the Dutch healthcare system. EDACS enables clear and efficient communication about a child’s eating and drinking skills between professionals and between professionals and parents.
There were only slight differences in interrater reliability outcomes among SLTs obtained in this study (ICC 0.84) compared to the original study by Sellers et al. (ICC 0.93). Both results are judged as statistically ‘excellent’ following the interpretation of Cicchetti [22]. Sellers et al. [19] assessed reliability of EDACS when used by pairs of SLTs who were both familiar with the child’s usual eating and drinking performance. In this study, eating and drinking abilities were classified by one SLT familiar with the child’s current feeding abilities, and one SLT who was unfamiliar with the child’s feeding abilities. Videos, live observations, and medical records were used by the latter SLTs (SLTs-2) to classify eating and drinking ability. It is possible that in some cases the ‘unfamiliar’ SLTs (SLTs-2) did not have enough background information to be able to classify all aspects of eating and drinking. This might explain the slightly lower SLT interrater reliability in the present study compared to Sellers’ study. Another explanation may be found in the larger number of subjects used in our study and greater (between subjects) variability of their eating and drinking abilities. From these findings, it can be concluded that eating and drinking ability can be classified by SLTs who are ‘familiar’ or ‘unfamiliar’ with the child from direct observation or from video recording.
The ICC value of 0.8, when EDACS is used by SLTs as well as parents, shows that this instrument can be reliably used by an informed parent. This supports the idea that parents should be considered as serious discussion partners. There is a trend for parents to classify their child on a lower EDACS level, i.e. greater abilities with eating and drinking, when compared with the opinion of the SLT. Possible explanations for this finding are that parents may be less aware of risk factors for inefficient or unsafe eating and drinking, or that parents may be more tolerant of risks to support their child to function at the edge of his/her abilities. SLTs may limit exposure to risks in a school or clinic setting for safety reasons. For the degree of assistance required during eating and drinking, parents reported their child to be in need of more help than the SLTs did. Parents may provide their child with more help when eating and drinking for practical reasons such as speeding up the time taken to finish a meal, whilst in a school setting when given enough time, a child may be able to eat and drink independently.
The moderate positive association between EDACS and GMFCS highlights that measures of gross motor function will not be sufficient to predict a child’s eating and drinking ability. The moderate positive association between a child’s ability to use his/her hands (MACS) and level of assistance needed to bring food and liquids to the mouth also highlights that MACS as a measure of hand function is insufficient to predict levels of dependency at mealtimes. The strong correlation between EDACS and DMSS reflects the construct validity of EDACS. However, the DMSS (linked to DDS assessment) can be used only by qualified clinicians in people with developmental disabilities. It is a validated scale where the level of the swallowing and feeding disorder is determined rather than the eating and drinking ability of the child with CP [9]. For scaling, the information from a parent questionnaire is used. It is not suitable for use by parents to convey their ideas about the child’s eating and drinking ability. Functional classification systems have arisen from models of healthcare based on family centered practice including collaborative teamwork with parents. The EDACS, along with the other functional classification systems for CP, enables parents, clinicians and researchers to communicate clearly with one another [23]. In this respect, our findings support the complementary use of DMSS and EDACS in clinical practice.
Overall, this study shows that EDACS is reliable and valid when used by experienced SLTs, both ‘familiar’ and ‘unfamiliar’ with the child and also when used by parents. For other healthcare professionals, the concepts of EDACS should be known thoroughly for adequate use of this classification system in partnership with parents. The usability study showed fairly good results in differentiating between levels, and also shows room for improvement, considering that 10-14% of users of the EDACS (SLTs and parents) experienced difficulties differentiating between the various levels. An E-learning module is beneficial in this respect.
Limitations
Only SLTs experienced in working with children with CP participated in the present study. In daily practice, not all SLTs will meet this standard, which is a limitation of our study. In addition, SLTs only observed lunch and snack times at school and did not observe usual mealtimes at home. They were aware of, but did not observe, all the different food texture choices made at home to ensure mealtime safety and efficiency within the context of the child’s environment away from school. This emphasizes the need for discussing a child’s eating and drinking ability with parents in routine care, and the utility of EDACS to support this. It should be noted that selection bias may have influenced the observed interrater reliability and usability. For instance, parents whose native language was not Dutch were not included in our study.
EDACS can be used to describe limitations on someone’s overall eating and drinking ability arising from CP. The gross categorical distinctions between EDACS levels can be insensitive to subtle features of someone’s eating and drinking ability. For example, some children show greater limitations in eating and drinking ability than one may expect when only considering oral motor capacities because of behavioural issues or hypersensitivity of the oral area. A child’s lack of experience or exposure to more challenging food textures or fluid consistencies may also suggest greater limitations to their eating and drinking ability.
Future perspectives
EDACS has the potential to address questions concerning the prevalence of limitations in eating and drinking abilities of children with CP at the population level. Also, the association of eating and drinking ability with other areas of functional ability (including gross motor function, speech and hand function) can be addressed as well as weight/growth data and functional prognosis. EDACS provides professionals with a means to describe observations of safety and efficiency linked to eating and drinking. EDACS highlights and points to the need to explore the difference between the eating and drinking ‘performance’ (usual activity) and ‘capacity’ (what a child can do at his/her best). As with the GMFCS, it is possible for eating and drinking difficulties to be identified and linked to different EDACS levels with the aim to support clinical management.
There is limited data concerning time related changes in eating and drinking abilities in people with CP. It is therefore uncertain how frequently children’s eating and drinking abilities should be reclassified using EDACS. Prospective longitudinal studies to examine the stability of EDACS levels over time are yet to be conducted. Longitudinal studies using the GMFCS and MACS demonstrate that individuals with CP usually remain stable over time and that, when there is change, it is no more than one level [24, 25]. Yet, uncertainties remain with regard to the natural course of eating and drinking difficulties in CP. Some clinicians expect that, over the years, a child may gradually be able to eat more challenging textures, use more types of utensils, and become more independent whilst eating and drinking [9]. However, as children with CP reach puberty, risk of aspiration may increase; not only by changes in nutritional needs or increase in scoliosis, but also due to anatomical and physiological changes of the oropharynx [7]. Consequently, oral motor growth and changes in posture might lead to a different EDACS level which would warrant repeated assessments. There is also clinical utility in investigating the correlation between nutritional status and EDACS level with the potential for EDACS to identify an increased risk of malnutrition due to limitations in eating and drinking abilities.
Conclusion
In conclusion, the Dutch EDACS is the first reliable, valid, and easily applicable tool to classify functional eating and drinking abilities in children with CP when used by experienced SLTs or parents. It will enhance the communication concerning eating and drinking abilities of these children among professionals and parents. It is analogous to other functional classification systems (GMFCS, MACS and CFCS). Use of EDACS may increase the awareness of safety and efficiency of eating and drinking ability in children with CP amongst different stakeholders. It has the potential to form the basis for discussions with parents and other caregivers about the safety and efficiency of children’s eating and drinking abilities.
Footnotes
Acknowledgments
The authors gratefully acknowledge all children and their parents for participating in this study. We would also like to thank all participating rehabilitation centers and special schools and their affiliated SLTs.
Conflict of interest
The authors declare there are no financial or non-financial conflicts of interest.