
Abstract
PURPOSE:
This study aimed to investigate the stability of the Gross Motor Function Classification System (GMFCS) in children with cerebral palsy (CP) in the two to four year age band, the frequency at which children were reclassified, and trends of reclassification to higher or lower ability.
METHODS:
This retrospective study included 164 children with CP between 24 to 48 months old with two or more GMFCS ratings at least 12 months apart between their second and fourth birthdays. GMFCS ratings were captured closest to 24, 36, and 48 months. Stability and reclassification trends were analyzed using inferential statistics. Frequency of reclassification, age at ratings, duration between ratings, and corresponding change rate were analyzed using descriptive statistics.
RESULTS:
When comparing ratings closest to second and fourth birthdays, a linear weighted kappa of 0.726 was found. Of the total population, 46.95% changed GMFCS levels at any time between two to four years of age, the majority of which were reclassified to a higher level of ability.
CONCLUSION:
Findings suggest the GMFCS is less stable in the two to four year age band compared to older age bands. Due to the importance of providing accurate guidance for caregivers and high rate of reclassification, it is recommended GMFCS levels be reassessed every six months during this period of time.
Introduction
Cerebral palsy (CP) describes a group of disorders attributed to non-progressive disturbances in the brain that occur in utero or during infancy and affect the development of movement and posture [1]. CP is the most common pediatric motor disability, impacting approximately one out of every 345 children in the United States [2]. A CP diagnosis is assigned based on clinical history, neuroimaging, and standardized assessments (i.e., Prechtl’s qualitative assessment of general movements, Developmental Assessment of Young Children, and Hammersmith Infant Neurological Examination) and can be established before six months corrected age [3]. The etiology and presentation of CP is heterogeneous, encompassing a wide range of neuromotor function and long-term outcomes, thus limiting accuracy in predicting future function based on diagnosis alone.
The Gross Motor Function Classification System-Expanded and Revised, which will be referred to as GMFCS, is a tool used to classify children with CP into one of five levels (I-V) according to their gross motor function, with a focus on sitting, transfers, and mobility [4, 5]. The less gross motor function a child has, the higher their GMFCS level will be. The GMFCS is a universally accepted classification tool as past studies have found it to be a stable, valid, and reliable measure of gross motor function in children with CP [6–9]. Stability is defined as a child maintaining the same level of function as classified by the GMFCS over time [10].
Due to the reported stability of the tool, the GMFCS is widely used by clinicians to predict a child’s future mobility needs and equipment use [5, 11]. The classification tool can thus assist clinicians in determining the appropriate treatment plan for a child with CP [12, 13]. Additionally, GMFCS levels can be used to guide surgical intervention [14–17]. However, GMFCS level alone cannot be used to drive decision making in determining the best candidate for these interventions [15].
The GMFCS is constructed into separate descriptions of gross motor function across five age groups, referred to as age bands. The age bands are: less than two years, two to four years, four to six years, six to 12 years, and 12 to 18 years. As a result, clinicians assign GMFCS levels according to the respective age band of the child [4, 5]. In 2008, Gorter et al. studied the stability of the GMFCS in children under two years of age and found it to be ‘less precise,’ with 42% of children changing GMFCS levels [18]. As a result, clinical practice has veered away from classifying children less than two years, typically waiting until the child is two before assigning a GMFCS level.
A major concern for clinical decision making and caregiver guidance is whether children with CP will remain at the same level of ability or be reclassified. Given that standard practice is to begin GMFCS classification in children at two years, it is imperative to understand the stability of the subsequent two to four year age band to provide evidence-based information about a child’s likelihood to maintain their current GMFCS level. After the initial classification, the first conversation a caregiver has with the clinician regarding their child’s GMFCS level is a pivotal moment in understanding and acceptance for the caregivers. By increasing knowledge about the rate of reclassification in this age band, clinicians can more accurately guide caregivers’ concerns and provide realistic expectations for their child’s expected gross motor function. Additionally, understanding the possibilities for secondary complications commonly associated with each GMFCS level can more accurately guide the clinician in their choice of interventions.
While current literature has examined the stability of the GMFCS in children at younger ages, no study to date has examined the two to four age band to a substantial degree (Table 1). In a 2006 study conducted by Palisano et al., stability of the GMFCS in children under six years was compared to those six years or older. They found classification of children younger than six years of age to have less stability than their older counterparts, with 75.7% agreement between ratings (0.84 weighted kappa) compared to children six years of age or older with 82.9% agreement (0.89 weighted kappa) [8]. Moreover, in a study of stability comparing classification of children under four to those older than four, Palisano et al. found those younger than four years of age to have a 64.5% agreement (0.76 linear weighted kappa); in contrast, they found children older than four years of age to have 80.3% agreement (0.88 linear weighted kappa) at last rating [10]. These studies generally indicate decreased stability of the GMFCS classification in children under six and four respectively. However, based on the findings of Gorter et al., showing ‘less precise’ stability in the zero to two year age band, it might be anticipated that these studies spanning multiple age bands could be misleading by the inclusion of children under two years of age.
Studies including the 2 to 4 year age band
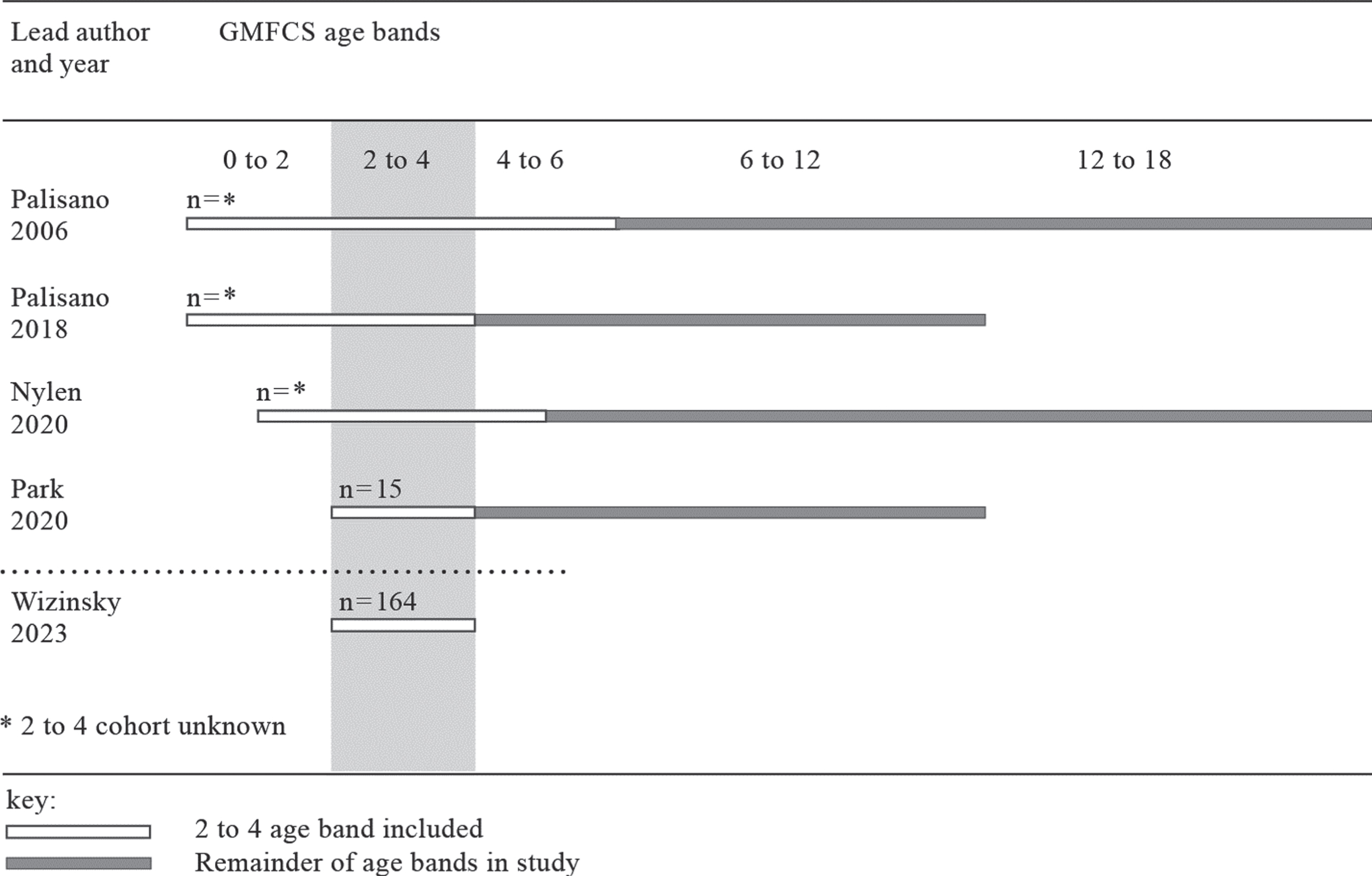
Studies including the 2 to 4 year age band
More recently, literature has begun to call into question the stability of the GMFCS in the two to four year age band. Nylen and Grooten retrospectively studied stability of the GMFCS in children under two years to 18 years of age. When looking at the total population, they found the proportion of change occurred most from two to four years, as follows: 12.9% at two years, 19.4% at three years, and 15.7% at four years [19]. However, many participants were outside of the two to four year age band, as the authors did not exclude children outside of the 24 to 48 month range when calculating percent range. It is also unclear how many participants in the study were within the two to four year age band. Lastly, Park conducted a study on change in GMFCS levels over two years for the two to 12 year population and found the two to four year age band to have the least amount of stability (kappa of 0.557) [20]. However, there were only 15 participants within this age band, making clinical implications difficult toascertain.
To date, the stability of the two to four year age band, which is interpreted to be≥24 months to≤48 months, zero days, has not been substantially studied. As clinicians assign GMFCS levels according to the age band, a thorough understanding of potential change within the two to four year age band is needed to best guide clinical practice. Prior studies have indicated difficulties with classifying children under four years of age, including a higher likelihood of change [8, 19]. Many factors including broad descriptors of the GMFCS and rapid motor skill development may contribute to a higher frequency of reclassification. The purpose of this retrospective study was to assess the stability of the GMFCS in children with CP in the two to four year age band using the ratings closest to the second and fourth birthdays. Additionally, this study sought to determine the frequency of children reclassified at any time within this age band and whether the trend of reclassification was to a higher or lower level of ability.
Design
This was a retrospective cohort study in which participants were identified from the CP Registry, a database within the electronic medical record (EMR), through Cincinnati Children’s Hospital Medical Center (CCHMC) in Cincinnati, Ohio. Exempt status was obtained from Institutional Review Boards of both CCHMC and Xavier University.
Participants
Initial eligibility criteria required that children were born between the target dates of January 1, 2009, to August 21, 2017. This date range was selected to obtain a larger sample size with minimal missing data points for children with CP within the two to four year age band as the EMR utilized at CCHMC was not primarily accessed by most departments in the institution to track GMFCS levels until 2011. Additionally, inclusion criteria required participants be between the ages of 24 to 48 months old, have two or more documented GMFCS ratings within the target date range, and have at least 12 months between the GMFCS ratings closest to their 24-month (Time 1) and 48-month (Time 3) birthdays. Furthermore, participants must have a diagnosis of CP listed in their EMR or clinical presentation consistent with CP, including periventricular leukomalacia, cerebral hemorrhage, or spasticity.
Preliminary investigation revealed 1,673 individuals in the CP Registry; 1,042 were automatically excluded as their birthdays were outside of the target date range or they were deceased. The remaining 631 individuals were meticulously screened using a standardized data collection form resulting in the exclusion of an additional 467 individuals. Ultimately, a convenience sample of 164 participants was reached.
Procedure
Standardized data collection forms and a procedural manual were created to gather GMFCS ratings closest to 24 months old (Time 1), closest to 36 months old (Time 2) and closest to 48 months old (Time 3). These GMFCS ratings were assigned by either a physical therapist or a pediatric rehabilitation physician. Given the excellent interrater reliability of the GMFCS, [9] ratings were extracted at each age regardless of which medical professional assigned the GMFCS level. A cutoff of two months between Time 1 and Time 2 as well as between Time 2 and Time 3 was established in order to maximize time between ratings, while still allowing for each data point to be obtained. The data collection forms were also used to acquire the following additional data: age at each GMFCS rating (months), time between ratings (months), whether change was present and in what direction, as well as clinical characteristics occurring between 24 and 48 months of age.
The primary investigators on this study were employed by the same institution using the CP Registry; therefore, data abstractors from an outside institution were recruited to complete data collection in order to decrease bias. Training was completed over the course of two days in order to obtain accurate and consistent data collection. Primary investigators instructed data abstractors on the important variables to be collected and how to locate these in the EMR. In order to accomplish interrater reliability of data collection, abstractors and primary investigators collectively coded four randomly selected participants. Discrepancies were reviewed and discussed until uniformity and consensus were achieved. Competency was determined when all abstractors collected the same information. Once final data was collected, the primary investigators reviewed and verified all information related to GMFCS ratings and ages to ensure optimal data quality.
Statistical analysis
Descriptive statistics were used to analyze population characteristics. All data were entered into IBM SPSS Statistics version 24.0 for analysis. Missing Time 2 data for eight participants were coded in SPSS software, and calculations took missing data into account.
Stability of the GMFCS at Time 1 and Time 3 was measured using linear weighted kappa and its 95% confidence interval via the interpretation of Fleiss, which designates a linear weighted kappa of values < 0.40 representing poor agreement beyond chance, values between 0.40 and 0.75 representing fair-to-good agreement beyond chance, and values > 0.75 representing excellent agreement beyond chance [21]. This interpretation of kappa was chosen to set a high threshold for stability as well as maintain consistency with prior studies of stability [5, 8]. To determine frequency of reclassification, simple percent agreement was calculated for all GMFCS ratings. McNemar’s chi-square test for symmetry was used to determine whether a trend was favorable toward a higher or lower functional level in the participants that exhibited change in GMFCS level. A p-value of less than 0.05 was determined to be statistically significant.
Results
Detailed characteristics of all participants are illustrated in Table 2. These specific patient characteristics were included as they are common comorbidities and interventions seen in children with CP in this age band. The majority of children in this study had spastic quadriplegia and had received botulinum toxin A injections in their lower extremities. The median number of physical therapy (PT) visits for the study population over a two-year period was 39.50 (75.0).
Characteristics of Participants (n = 164)
Characteristics of Participants (n = 164)
*spastic quadriplegia is terminology used in EMR. CP = cerebral palsy.
Distribution of GMFCS levels for Time 1 and Time 3 is illustrated in Table 3. The linear weighted kappa was 0.726, and the strength of agreement was classified as fair-to-good. When comparing ratings closest to second and fourth birthdays, 38.41% (63) of these children were reclassified. However, when looking at change at any time, 46.95% (77) of the total population changed. When examining all three ratings, 13.41% of participants were reclassified to a lower level of ability, 25.00% were reclassified to a higher level of ability, and 8.54% were reclassified to their original rating (Table 4). The p-value for McNemar’s chi-square test for symmetry was found to be 0.001. Of those who were reclassified, 67 participants changed one level, nine participants changed two levels, and only one participant changed three levels. Additionally, children who were originally classified at levels III and IV closest to their second birthday were most likely to be reclassified by their fourth birthday, whereas children who were originally classified at levels I and V were least likely to be reclassified.
Stability of the Gross Motor Function Classification System (GMFCS) comparing furthest margins of 2 to 4 age band
Linear weighted kappa = 0.726, 95% confidence interval 0.664–0.789. Percentage agreement = 61.6%.
Reclassification trends across all ratings
McNemar’s chi-square, p = 0.001.
For further analysis of the stability within this age band, a closer examination of the level of agreement and percent change between the second, third, and fourth birthdays was conducted (Table 5). GMFCS recordings were able to be extracted at each targeted time point with the exception of eight participants who lacked a documented GMFCS level for Time 2 (closest to 36 months old). Therefore, there were eight participants with missing data for the intervals between Time 1 and Time 2 and between Time 2 and Time 3. Frequency of change was higher between the child’s second and third birthdays when compared to their third and fourth birthdays. Ultimately, most change between ages occurred when comparing their GMFCS level at their second birthday to that of their fourth birthday (Table 5).
Age, duration between ratings, and corresponding change rate
*Mean age in months. SD = standard deviation.
When further examining extraneous variables, it was found that participants with spastic quadriplegia who changed to a higher level of ability received more PT visits, with a median of 78.00 (68.25), compared to those who changed to a lower level of ability or had no change (Table 6). Comorbidities and the medical interventions were also examined in relation to GMFCS trends. A statistically significant p-value of 0.02 was found for cortical visual impairment (CVI) in those who returned to their original classification at age two (Table 7). Other findings of comorbidities and medical interventions were not considered statistically significant.
Physical therapy visits for participants with spastic quadriplegia
GMFCS: Gross Motor Function Classification System; IQR = interquartile range; SD = standard deviation.
Prevalence of comorbidities and medical interventions in relation to Gross Motor Function Classification System (GMFCS) trends
The purpose of this study was to determine the stability of the GMFCS in the two to four year age band, establish the frequency of reclassification, and identify whether the trend of reclassification was to a higher or lower level of ability. The results from this study showed the stability of this age band to be fair-to-good (linear weighted kappa = 0.726), suggesting the GMFCS in this age group is less stable than that reported in previous studies of older children [8, 23]. When compared to studies of adjacent age bands, this study illustrated higher stability than the 0.70 kappa in children in the 0–2 age band [18] and lower stability than the 0.84 weighted kappa in a study looking at children under six years [8]. Although relating kappas between studies is an imperfect comparison, this study contributes to the existing literature in that it illustrated a trend of decreasing stability at successively younger ages [8, 18].
Prior research into the stability of the GMFCS has typically spanned across multiple age bands [8–10, 24]. While this has provided general insight on the stability of the GMFCS across time, the rate of change within each age band has not been thoroughly studied. When the stability of this tool is studied across age bands, the risk of confounding the results is high as this assumes equal probability of change within each age band studied. The findings of Gorter et al. on the zero to two year age band along with the findings of this study on the two to four year age band conclude that there is less stability in these younger age bands. This conclusion can be made based on the focused study of each age band independently.
When examining frequency of reclassification at any time throughout this age band, 46.95% changed levels. This is consistent with other studies that examined the stability in children under four with similar sample sizes [9, 18]. This study sought to further determine why only 38% of participants changed from their second to fourth birthdays, while 46.95% changed at any time. This discrepancy appears to be due to a small percentage of participants changing classification multiple times, yet always returning to the original GMFCS level taken closest to their second birthday. This suggests a clinical recommendation to coach caregivers on the tendency for lasting change around 38% of the time in the two to four age band.
While delivery of a child’s GMFCS rating can be difficult for the caregiver [25], it is important to provide anticipatory guidance on future gross motor function. This guidance is crucial for a complete understanding of potential equipment needs, financial planning, and medical treatment [26]. The findings from this study showed that a high percentage (38%) of children changed levels between two to four years of age; therefore, clinicians are advised to keep this variability in mind when coaching caregivers on the implications of their child’s GMFCS level. This is particularly relevant for those initially classified at levels III or IV near two years ofage.
Regarding the optimal approach and timing of the delivery of the GMFCS by the clinician, a few best practice standards emerge. The latest evidence in CP-specific intervention has illuminated the need for a family-centered focus for goal setting [27]. Utilization of the GMFCS Family Report Questionnaire has been shown to have excellent reliability between parents and providers [28]. In addition to serving as a collaborative platform for unifying joint decisions about the child’s current level of function, the GMFCS Family Report Questionnaire may also assist with the development of shared and realistic goal setting. Lastly, reassessment of the GMFCS every six months is ideal as there is a high rate of gross motor skill change in children under seven years[6, 29].
The retrospective nature of this study was an inherent limitation as it reduced the degree of control over the motor type and topographic distribution, reporting of variables related to frequency and type of interventions, and ability to gather all data points for each participant. The majority of participants in this study who changed levels did so to a higher level of ability (Table 4). This contrasts previous studies that included children within this age band [9, 10]. Those previous studies did not indicate the frequency nor type of therapeutic interventions, leaving many unstudied variables.
The findings of this study related to characteristics and comorbidities were not statistically significant, with the exception of CVI in those who returned to their original classification at age two. However, this sample size of participants with CVI was low, which limits the generalizability of the results. Additionally, the variables related to therapy were not controlled; however, the high percentage of participants with spastic quadriplegia prompted further review of the frequency of PT visits in the EMR. It was found that participants with spastic quadriplegia who changed to a higher level of ability received more PT visits within a two-year span compared to participants who changed to a lower level of ability or had no change. However, only PT visits within this institution were recorded; therefore, this study was not able to have an appreciation of other therapy services participants may have received.
The high rate of participants presenting with spastic quadriplegia in this study may reflect a somewhat anomalous population, given that the studying institution draws patients from around the country for specialized services. In this study, 56.7% of participants presented with spastic quadriplegia, compared to an average of 23% in the general population [2, 30]. Children with spastic quadriplegia experience a high rate of comorbidities along with a tight correlation to level IV classification [31, 32]. This might lead to the assumption that this demographic is not likely to change classification levels. However, the findings from this study showed otherwise. While the absence of Time 2 GMFCS levels for eight participants did not affect the overall results between Time1 and Time 3, it might skew results for determining trends of change within the age band.
These findings call for a prospective investigation into how stability of children in this age band may be affected by the therapeutic and medical approach to their care, original GMFCS rating, as well as distribution of topographic impairment. Given the growing movement to identify CP at earlier ages, future research might focus on these and other specific variables in order to provide better evidence-based guidance.
Conclusion
While this study was not a population-based study given the high percentage of participants with spastic quadriplegia, these results nevertheless illustrate that the GMFCS classification is less stable within the two to four year age band compared to older ages. There is a need for frequent reassessment of classification in children under the age of four in order to drive accurate delivery of therapeutic interventions and guide caregiver planning. This study further refines the landscape of knowledge regarding the stability of GMFCS, which is invaluable for providing accurate anticipatory guidance tocaregivers.
Footnotes
Acknowledgments
We would like to thank Cincinnati Children’s Perlman Center for clinical support. Special thanks to Claire Morress, PhD, OTR/L, ATP, for study design, review of data to ensure accuracy, and data analysis and to Max Buot, BS, MSE, PhD, for data analysis and review of data representation in text and graphical depictions. Additional thanks to Maria Cardarelli, OTR/L, Gaby Ulanowski, OTR/L, Amanda Winner, OTR/L, and Claire Zernich, OTR/L, for assistance in gathering data.
Conflict of interest
The authors have no conflict of interest to report.
Ethical considerations
CCHMC IRB ID: 2019-1028. Date: 09.24.2019. This study, as a retrospective chart review, is exempt from Institutional Review Board approval.
Xavier IRB: Protocol #19-041. Date: 10.02.2019. This study, as a retrospective chart review, is exempt from Institutional Review Board approval.
Funding
No funding was received to assist this research.