
Abstract
A 12 year-old female presented to the emergency department with a right hemiparesis, headache, and neck pain. Initial neural imaging studies were unremarkable. However, a repeat MRI of the cervical spine during her acute hospitalization showed an acute spinal infarct. Neurological workup was consistent with fibrocartilaginous embolism (FCE) as the etiology. After several weeks of intensive inpatient rehabilitation, the patient demonstrated remarkable functional progress. This case report reviews the comprehensive pediatric literature on FCE with focus on the mechanism of injury, role of imaging studies, treatment options and prognosis. Awareness of the typical clinical history, as well as the signs and symptoms characteristic of FCE will improve the identification of this rare cause of abrupt weakness and potentially facilitate functional recovery.
Introduction
Fibrocartilaginous embolism is a very rare form of spinal cord injury that affects both children and adults. According to Davis and Klug [1], the distribution of patients with FCE is bimodal with an increased incidence in both the young adult population, with an average age around 22 years old, and in the adult population, with an average age around 60 years old. In addition, there seems to be higher rates of FCE in the female population [2, 3, 4]. Due to the paucity of literature on this topic, the exact prevalence of pediatric FCE remains unknown. Based on review of the literature by the authors of this case report, there have been only 16 other documented cases of FCE in patients under the age of 18 years old to date [5].
Neurological signs and symptoms may include but are not limited to back pain, sensory and motor deficits below the level of the lesion, and possible neurogenic bladder and bowel. The injury can affect any level of the spinal cord but 66–70% of cases affect the cervical region [2, 3, 6]. Because of the associated functional deficits, it is important that physical and occupational therapy be implemented early in the treatment plan to enhance the potential for improved functional outcomes. This case will focus on the diagnostic features of this disorder and the impact of rehabilitation therapies in facilitating the functional progress made by the patient.
Case presentation
Patient is a 12-year-old female with an unremarkable premorbid history who had an abrupt onset of right-sided weakness, right-sided paresthesias, head-ache, and neck pain. She did not have loss of consciousness, seizure-like activity, change in mental status, impaired vision, or loss of bowel or bladder function. She also had no recent travel or preceding history of trauma. The patient did have a preceding bout of otitis media that was treated with amoxicillin two weeks prior to admission.
Presenting vital signs were stable other than tachypnea with respiratory rate in the 30s. Oxygen saturations were maintained within normal limits on room air. Physical exam revealed a well-developed, well-nourished female who appeared in no acute distress. Cardiac and respiratory exams were unremarkable. On cranial nerve exam, patient’s pupils were equal and reactive to light, extraocular movements were intact without nystagmus, facial expression was symmetric, and hearing was intact. Initial motor exam was significant for 3/5 strength in the right lower extremity, 0/5 strength in the right upper extremity, and 5/5 strength in the left upper and lower extremities. In addition, the patient’s sensation to light touch was diminished in the right forearm and upper arm regions. Deep tendon reflexes were initially 2+ and symmetric upon presentation. CBC and BMP were unremarkable. A lumbar puncture was performed and a CSF culture showed no organisms after 72 hours of incubation. In addition, all viral studies from CSF were negative. CSF WBC count was 1, RBC count was 1, the appearance of the CSF was clear and glucose level was within normal range. Finally, there were no oligoclonal bands and CSF IgG was within normal limits. Initial MRI and non-contrast CT of the cervical spine were both unremarkable.
Patient’s hospital course was complicated by respiratory distress requiring aggressive pulmonary treatment. On day two of hospitalization, the patient began to experience progression of symptoms, which included decreased head and trunk control, and loss of reflexes with ascending sensory level (initially at C4). The neurology team’s initial differential diagnosis included acute flaccid myelitis, transverse myelitis, acute disseminated encephalomyelitis, neuromyelitis optica, or less likely stroke. There was also concern for a right hemicord lesion at C4 but this was lower on the differential since the C-spine CT and MRI were initially normal without any signs of cord compression, inflammation, ischemia, or hemorrhage.
The patient was initially treated with fluoxetine, aspirin, and IVIG for presumed transverse myelitis. However, repeat MRI of the cervical and thoracic spine showed a T2 hyperintensity within the C2–C3 intervertebral disc posteriorly with a small focal protrusion (Fig. 1). Radiology suggested that these image findings favored an early subacute cord infarct due to FCE as opposed to transverse myelitis. Therefore, the patient was only given 2 days of IVIG but did receive 5 days of IV methylprednisolone.
MRI of the cervical and thoracic spine showing T2 hyperintensity within the C2–C3
intervertebral disc.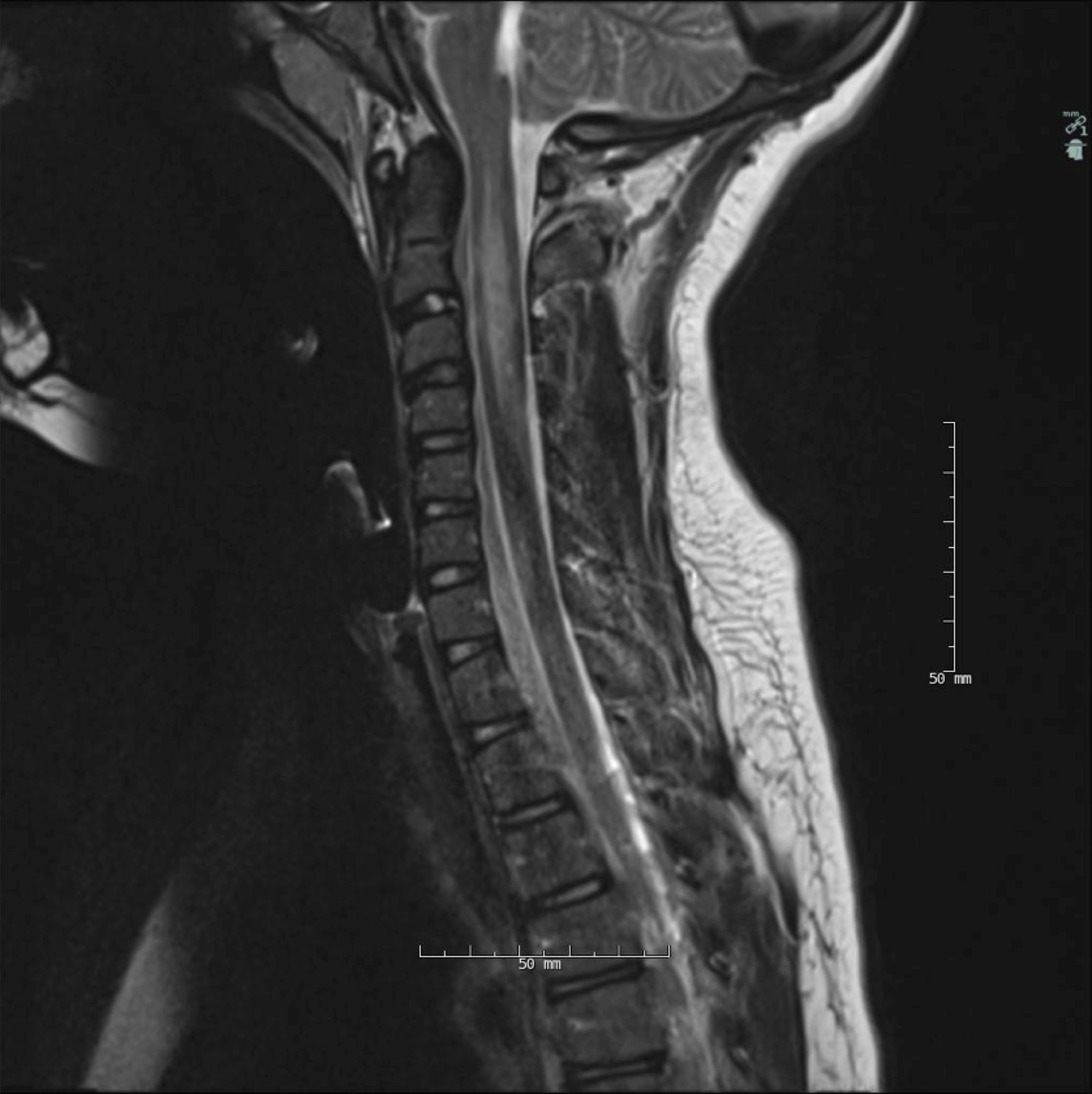
After medical stability was attained, the patient was transferred to the pediatric acute inpatient rehabilitation unit where she received comprehensive rehabilitation therapies 6 days a week, which included speech therapy, occupational therapy, and physical therapy. Other services included child life services, educational classes, and support from social work and psychology teams.
During her hospitalization, the patient made remarkable functional gains. Functional Independence Measure for Children (WeeFIM) scores were assessed at admission and discharge. On admission, the patient was modified independent for eating, supervision for grooming, total assistance for bathing, maximal assistance for upper and lower body dressing, and minimal assistance for toileting. Upon discharge, the patient was modified independent in all activities of daily living other than lower body dressing for which she needed minimal assistance (Table 1). On admission, the patient was unable to ambulate. On discharge, the patient was able to ambulate 500 feet, including ascending and descending a flight of stairs with supervision. To assist with ambulation, a carbon fiber ankle foot orthotic was prescribed for the right lower extremity. Patient continued to receive outpatient therapy after her discharge from the acute rehab facility.
Functional independence measure for children (WeeFIM)
The exact mechanism of injury of FCE is unknown although there have been multiple proposed theories throughout the literature. One proposed theory is that contents of the nucleus pulposus shift into a radicular artery or its segments after an injury. The injury is thought to be caused by increased pressure on the intervertebral disks that causes a tear in the annulus fibrosis and allows extrusion of material into the arteries [2]. This is thought to be more common in younger patients since spinal structures are highly vascularized in this population. Autopsies have supported this theory as nucleus pulposus fragments have been identified in the spinal cord of postmortem patients [4]. Another theory is that there are vertebral abnormalities in some individuals that predispose them to FCE. This theory is less convincing since these abnormalities have been found in a large number of the population who did not experience a spinal cord injury attributed to FCE [6].
There have been several studies about FCE published throughout veterinary literature. The majority of cases have been identified in dogs; however, there have been cases of FCE in cats, horses, swine, and turkeys. In a review from 1973 to 2013 conducted in canines, researchers found that the etiology of FCE was thought to be similar to that in adult humans. In terms of prognosis, approximately 85% had the ability to ambulate completely independently [12]. When reviewing literature in cats, FCE was less often identified. In a case study of fourteen cats that were diagnosed with FCE, they presented similarly to human subjects with signs of hemiparesis or paraplegia. Five cats of the fourteen had favorable outcomes with minimal to no residual deficits [13]. There has been continued research throughout the animal population with the increased use of advanced imaging, such as MRIs.
As in this case study, FCE is often initially diagnosed as transverse myelitis. The major clinical features distinguishing FCE from transverse myelitis include the absence of prodromal illness, trauma, onset, time of progression, CSF findings, and imaging studies. In FCE, there usually is no prodromal illness but there is typically an associated trauma in contrast to transverse myelitis, which is often preceded by a prodromal illness [2]. In pediatric FCE literature, there have been several precipitating factors that have been identified. These include falls, weightlifting, and injuries incurred in activities such as basketball, ballet, and roller coaster riding [5]. However, in cases where no definite history of trauma is identified, it is possible that FCE can be caused by a relatively minor injury, which is not recognized as the precipitating event. Another distinguishing feature of FCE is its time of progression, which typically is less than 48 hours in contrast to transverse myelitis, where signs and symptoms may take up to one week to peak. CSF studies also help differentiate these two diseases. In transverse myelitis, CSF analysis reveals oligoclonal bands or an elevated IgG index, whereas CSF studies are typically normal in FCE [2].
From an imaging perspective, MRI remains the gold standard for diagnosing FCE. MRI shows hyperintensity mainly of the gray matter on T2-weighted images and cord enlargement [7]. The areas of the spinal cord supplied by the anterior spinal artery are often the most impacted from FCE [8]. Unfortunately in the initial stages of disease, MRI may be normal, as demonstrated in this case. Diffusion weighted imaging (DWI) has the potential to help clinicians differentiate spinal cord infarctions from other inflammatory etiologies. Additionally, DWI has the potential to identify spinal cord ischemia within hours of presentation, which may help practitioners identify the diagnosis earlier [7].
Maintaining hemodynamic stability in an FCE patient is critically important. Previous studies have suggested a non-surgical approach without biopsy or cord decompression [2]. There is no current standard treatment for FCE. Although there has been some literature discussing the potential benefits of steroids, their effect on recovery remains uncertain. Steroids are often still used in current day practice for FCE treatment [2, 9]. Treatments such as hyperbaric oxygen, mannitol, thyrotropin releasing hormone, dimethyl sulfoxide naloxone, IV immunoglobulin, plasma exchange, and IV heparin have been proposed but the effectiveness of these treatments remains uncertain [9, 10]. Rehabilitation therapies, however, have been established to improve functional outcomes in these patients [6]. Hopefully future research will help establish a more effective clinical and functional treatment regimen for FCE.
Review of the literature indicates that FCE typically has a poor prognosis. However, there have been more recent cases with favorable neurological outcomes [2, 3]. Since there have only been a limited number of cases, especially in the pediatric population, FCE has only recently been recognized in the differential diagnosis of patients experiencing a spinal cord infarct. Similar to this case, there have been other recent cases in which patients have had significant functional recovery. Variables such as extent and level of the infarction, unilateral versus bilateral involvement, and age of the patient when injured, all impact prognosis [6, 11].
Conclusion
FCE is a rare cause of spinal cord injury. This study is the first to specifically focus on the rehabilitation goals and functional progress in a patient with FCE. After approximately 3 weeks of intensive inpatient rehabilitation, this patient made substantial progress in functional mobility and activities of daily living. FCE should be included in the differential diagnosis of abrupt onset of weakness in both adults and children. Early initiation of comprehensive rehabilitation therapies may lead to favorable functional outcomes.
Footnotes
Conflict of interest
The authors have no conflicts of interest to report.