
Abstract
BACKGROUND:
Chronic obstructive pulmonary disease (COPD) is a preventable and treatable disease. Mucus accumulation, a common impairment in COPD affects lung function, exacerbations and quality of life. Physiotherapy measures including positive expiratory pressure devices like lung flute form the non-pharmacologic treatment options for the same. Although not a primary airway clearance device, inspiratory muscle trainer (IMT) plays a role in it. The aim of this study was to compare the effectiveness of lung flute and IMT as methods for sputum clearance in COPD.
METHOD:
Participants with COPD were recruited from the Department of Pulmonology and screened for eligibility. Block randomization was used to divide the participants into three groups: Inspiratory muscle training (IMT), lung flute (LF), and routine physiotherapy (RP). Supervised 30 minutes of in-patient intervention was delivered to all the groups for 6 days, once a day. Total sputum volume analysis (TSV) was conducted before and after 6 days of intervention. Descriptive statistics were presented as median and quartiles. Kruskal Wallis H test and Wilcoxon signed rank test were applied.
RESULTS:
60 participants aged 55 to 65 years with mild to moderate COPD were included in the study. Median TSV for RP, LF and IMT were 8.50, 20.50 and 25.75 ml respectively. Pair-wised comparisons for TSV revealed significant differences for the means of the rank scores between RP and LF (LF dominant) (p < 0.001), RP and IMT (IMT dominant) (p < 0.001) and LF and IMT (IMT dominant) (p = 0.002).
CONCLUSION:
IMT performed superiorly in terms of sputum clearance in patients with COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, preventable and treatable disease. COPD is characterized by persistent respiratory symptoms and airflow limitation due to airway and/or alveolar abnormalities mainly caused by significant exposure to noxious particles or gases [1]. With inclusion of the low middle income countries, COPD is worldwide one of the top three causes of death [2]. With 64 deaths per 100,000 populations, COPD stands as the second most common cause of death in India (9.7%) and it accounts for 3% loss of disability-adjusted life years [3–5].
Common impairments observed in COPD include airflow limitation, chronic productive cough, mucus hypersecretion and gaseous exchange abnormalities. These may be the consequence of cigarette smoke exposure, activation of mucin gene transcription or acute and chronic viral or bacterial infection [1, 6]. The primary mechanisms inducing excessive mucus are overproduction and hypersecretion by goblet cells, increased degranulation, decreased mucus elimination owing to poor ciliary function, distal airway obstruction, and ineffective cough secondary to respiratory muscle weakness and reduced peak expiratory flow [7]. Mucus accumulation in COPD patients affects pulmonary function, exacerbations, hospitalizations, and mortality [7]. Management of COPD is aimed at alleviating the symptoms, and reducing the risk of future exacerbations [8]. Physical therapy measures including positive expiratory pressure devices form the non-pharmacologic options for the treatment of mucus accumulation [9–12].
Lung flute (LF), an oscillatory positive expiratory pressure device, is a reusable, plastic device that is non-invasive, easy to use and drug free [13, 14]. It consists of a mouthpiece and a reed inside a 36 to 38-cm rectangular plastic tube and it generates audio waves (18–22 Hz) [15, 16]. With vigorous exhalation, its output is 110–115 db by using 2.5 cmH2O of pressure [16]. The lung flute generates sound waves which travel down the tracheobronchial tree and vibrate secretions, thus enhancing the mucociliary clearance, especially of lower airways [14, 17].
Cough is one of the most effective ways of sputum clearance. The first stage of cough requires inspiring enough air to provide the volume necessary for a forceful cough. Inspiratory Muscle Training (IMT) targets to increase strength and endurance of the inspiratory muscles by increasing the load to inspiration [18] Improving strength of inspiratory muscles could be evaluated as an approach to enhance the inhalation phase of cough and improve sputum clearance [19]. Although not a primary airway clearance device, inspiratory muscle training (IMT) has been shown to contribute to sputum clearance in previous studies [20, 21].
Studies comparing the effects of threshold IMT and lung flute in facilitating sputum clearance in patients with COPD have not been conducted. Therefore, the purpose of the study was to compare the effectiveness of lung flute and IMT as methods for airway clearance in patients with COPD.
Materials and methods
Participants, randomization and allocation
Participants with COPD were included in the study when older than 40 years of age, with <50% of post-bronchodilator airflow obstruction measured by spirometry (GOLD stage 3–4). They were excluded if they were hemodynamically unstable (systolic pressure <100 mmHg, diastolic pressure <60 mmHg and mean arterial pressure <80 mmHg), had cognitive impairments or had a history of any other pulmonary conditions, severe cardiac conditions, abdominal or thoracic surgeries in the past three months.
Computer generated random numbers were assigned to the participants. A sealed opaque envelope was used to conceal group information. Block randomization was used to divide the participants into three groups: Inspiratory muscle training (IMT group), lung flute group (LF group), and routine physiotherapy group (RP group). CONSORT guidelines were followed in this study [22]. Consort flow diagram is depicted in Fig. 1.
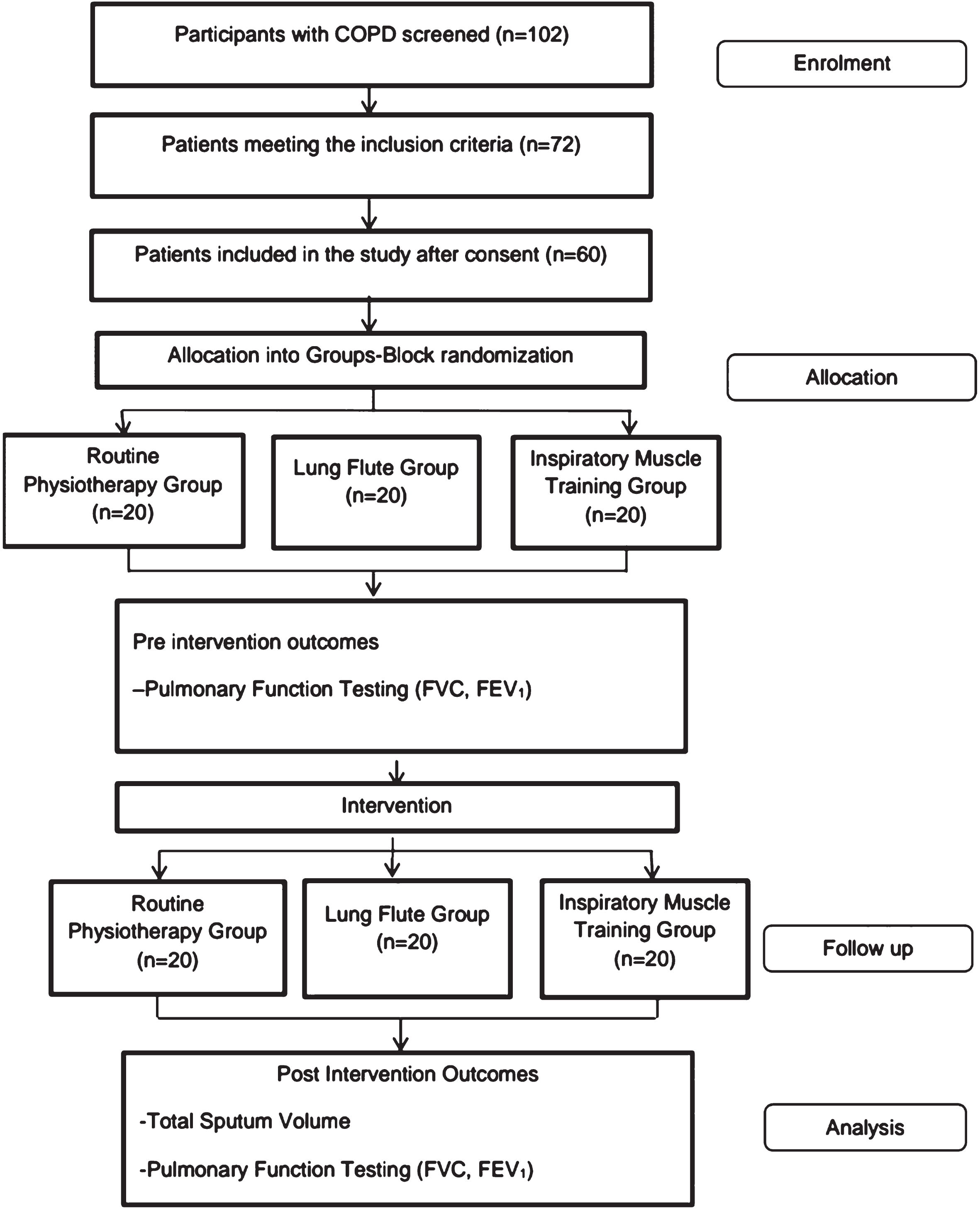
Consort Flow Diagram for the study. Legend: FVC- Forced vital capacity; FEV1-Forced expiratory volume in 1 second.
After the group allocation, demographic data-including age, weight, height, body mass index, comorbidities-were collected. Supervised 30 minutes duration of in-patient physiotherapy intervention was delivered to all the three groups for 6 days, once a day. Participants were taught exercises related to their allocation groups (IMT, LF, RP). Before the treatment, a dose of mucolytic was administered to all the patients via nebulization. The treatment along with the dosage and duration was documented in the patient records after each session.
Procedure for RP group
Participants were positioned in a half lying position and performed active cycle breathing technique [23]. They were mobilized from half lying to short sitting followed by standing and walking according to their tolerance levels (fatigue, level of dyspnea and changes in vital signs).
Procedure for LF group
Participants were positioned in a half lying position. They were instructed to blow twice into the long flute vigorously enough to make the reed oscillate, followed by 5 normal breaths. Each session encompassed 2 sets of 10 repetitions, followed by 3 huff coughs [24]. This was furthered by routine physiotherapy.
Procedure for IMT group
Participants were positioned in a half lying position. A nose clip was worn by them to avoid any additional air flow. They were then instructed for expiration to residual volume followed by maximal inhalation with a tight seal around the mouth-piece of the threshold IMT. The participants were instructed to take 10 breaths through the device making a maximal inspiratory effort. This was followed by 2- to 3-second breath hold, and an active exhalation to functional residual capacity residual capacity. After every 5 breaths, they had to cough or huff [25]. This was followed by routine physiotherapy.
Outcome measures
Outcome measures were assessed before initiating the treatment and after completing 6 days by an investigator who was blinded to the group allocation. Volumetric assessment of sputum was the primary outcome measure. Pulmonary function test (PFT) was the secondary outcome measure.
Volumetric assessment of sputum
Sputum quantity was assessed using a volumetric jar (Technico® TC 27°C). Sputum volume expectorated by each participant was measured after each session and recorded in milliliters (ml). Total sputum volume (TSV) was calculated after completing 6 days of treatment.
Descriptive statistics of the participants included in the study
Descriptive statistics of the participants included in the study
RP = Routine physiotherapy, LF = Lung flute, Inspiratory muscle training (IMT), K-S = one sample Kolomogorov-Smirnov test, Q = Quartile.
Forced vital capacity (FVC) and Forced expiratory flow rate (FEV1) was assessed using EasyOne Plus Diagnostic Spirometer Machine. The procedures were performed according to European Respiratory Society guidelines [26]. PFT was assessed on the first and the sixth day of intervention.
Data analysis
Data was analyzed using IBM SPSS package (version 28.0 Armonk, NY: IBM corp). Normal distribution was checked by means of formal testing using Kolmogorov-Smirnov with Lilliefors significance correction, Q-Q plotting and visual check of the histograms. The output variables dispersed over the different levels of the within subjects ‘’PRE-POST’ factor and the levels of the between groups presented mainly with non-normal distributions. The descriptive statistics encompassed presentation of minimum, maximum, median, quartile 1(Q1), and quartile 2 (Q2). The 95% confidence intervals (CI95%) were obtained with bootstrapping (1000 samples). Non parametric mixed ANOVA design does not exist. Therefore, the non parametric pathway for analysis followed the following steps: check of equality of the PRE level distributions between the different therapies using the Kruskal Wallis H test, analysis of the differences between PRE and POST scores for each of the therapies using a Wilcoxon signed rank test, calculation of the paired differences between PRE and POST for each of the group for differences between the different groups using the Kruskal Wallis test, with post hoc pair-wised comparisons based on the Mann-Whitney U test. For post hoc pairwise comparisons, the Benjamini-Hochberg procedure was used to cope with the False Discovery Rate. To claim a statement concerning a pair-wised difference between medians, the assumption of similarity between two distributions in shape was checked by means of a Kolmogorov-Smirnov Z test, whereas the similarity of variability was checked using a non parametric Levene’s test. If one of these assumptions was violated, the statement of a significant Mann Whitney U test was that the distributions differed. Effect sizes for the Mann-Whitney U test and the Wilcoxon signed rank test was calculated by dividing the Z-score of the test score with the root of the sample size. A p value of less than 0.05 was considered statistically significant.
Results
60 participants with COPD were included in the study and were divided into three groups i.e. RP, LF and IMT. Each group comprised of 20 participants. None of them experienced any serious adverse events that required major medical or surgical interventions. The characteristics of the participants are depicted in Table 1. One-way ANOVA presented the participants to be comparable for age (p = .460) and BMI (p = 0.934) between the levels of the ‘therapy’ factor. Baseline comparison showed no significant difference between the groups.
Total sputum volume
For therapy RP, LF and IMT, TSV presented with a median of respectively 8.50 (CI95% 6.51 11.50), 20.50 (CI95% 19.25 22.75) and 25.75 (CI95% 22.00 27.00). The non parametric analysis of the TSV variable is presented in Table 2. Kruskal-Wallis on the different levels of the ‘therapy’ factor was significant (p < .001) Pair-wised comparisons for TSV revealed significant differences for the means of the rank scores between RP and LF (LF dominant), RP and IMT (IMT dominant) and LF and IMT (IMT dominant).
Non parametric analysis output of Total sputum volume (TSV)
Non parametric analysis output of Total sputum volume (TSV)
K-S = 2 samples Kolmogorov-Smirnov z-test, RP = Routine physiotherapy, LF = Lung flute, Inspiratory muscle training = IMT.
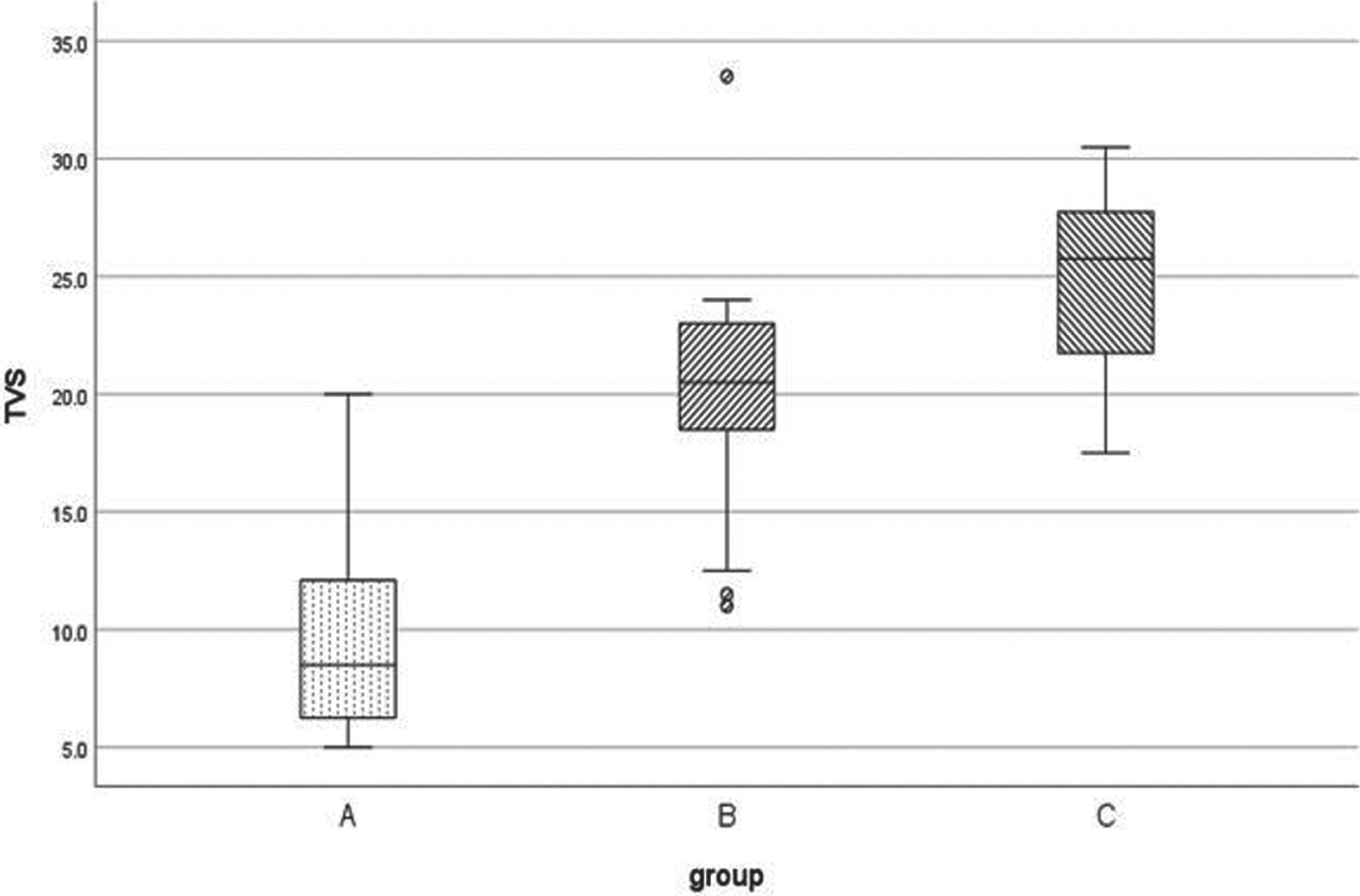
Boxplot for Total sputum volume in ml (TVS). Legend: Group A = Routine Physiotherapy, Group B = Lung Flute, Group C = Inspiratory Muscle Trainer; * = extreme outlier. = moderate outlier.
For therapy RP, LF and IMT, FVC –PRE (L) presented with a median of respectively 1.56 (CI95% 1.44 1.92), 1.34 (CI95% 1.11 1.65) and 1.24 (CI95% 1.05 1.69), for FVC-POST 1.73 (CI95% 1.60 2.04), 1.78 (CI95% 161 1.86) and 2.666 (CI95% 2.14 2.83). Significant differences were found in LF and IMT as compared to RP.
For therapy RP, LF and IMT, FEV1-PRE (L) presented with a median of respectively 1.02 (CI95%.78 1.45),.92 (CI95%.64 1.15) and.66 (CI95%.55.73), for FEV1-POST 1.09 (CI95%.89 1.88), 1.94 (CI95% 1.45 1.98) and 1.55 (CI95% 1.12 1.85). Significant differences were found in LF and IMT as compared to RP.
Discussion
The aim of this study was to compare the effective ness of LF and IMT for sputum clearance in patients with COPD along with its effects on pulmonary function. In this study, LF and IMT presented a large effect on TSV as compared to RP. Moreover, IMT was significantly more effective than LF. IMT had a larger improving effect on FVC than LF. According to the results of this study, adding IMT to the treatment protocol for COPD could prove beneficial.
In this study, significant differences in total sputum volume were found among the groups, with IMT being the most effective. This could be because strengthening the inspiratory muscles increases the lung volume prolonging the inspiration and expiration phase of cough and the mucus movement [27]. Furthermore, the increased stretch in the expiratory muscles due to the increased lung volume augments a more effective cough [19]. This result seems to be in contrast with the pilot study done by Naraparajju et al where they found acapella to be more effective than IMT in patients with bronchiectasis [21]. However, the effects of IMT and acapella on sputum volume were limited to one session. According to McConnel, IMT should be provided for at least 5–6days for to be effective enough for sputum clearance [25].
With the increase in lung volumes in COPD, the chest configuration is altered, shortening the inspiratory muscles and leaving them at a mechanical disadvantageous position. This reduces the force generated by the inspiratory muscles. However, the improvement in strength of the inspiratory muscles resulting from the IMT may significantly improve the inspiration phase of cough ultimately improving the cough production [19]. These elements may partly explain the differences in results between the study of in Naraparajju et al. and the study presented here.
Airflow limitation and lung hyperinflation is one of the main impairments in COPD which results in a decreased volume of expiration and consequent gas trapping, causing lung hyperinflation. Hyperinflation alters the mechanics of breathing, placing the diaphragm in a flattened position which reduces its contribution to ventilation affecting the pulmonary function. Increase in diaphragm strength could also increase maximal expiratory pressures according to a review conducted by de Medeiros et. al. [28]. They suggested that stronger inspiratory muscles are able to expand the thorax generating larger elastic recoil of the lungs and chest wall, which may have enhanced PFT data in the IMT group. However, considering the short duration of 6 days of intervention the improvements in the PFT values could be attributed to learning effect rather than a physiological effect.
Hitherto, IMT has demonstrated to improve inspiratory muscle strength and pulmonary function. This study also demonstrated IMT to be an effective modality for airway clearance in patients with COPD. Therefore, IMT can be considered to achieve two goals with a single treatment modality. This might be beneficial as it may reduce the requirement of additional airway clearance techniques and also reduce the treatment duration. Further studies are needed to prove this hypothesis.
This study was done for a short-term duration. The use and dosage of pharmacological agents such as nebulizers, which could have influenced the intervention, was not recorded. Moreover, the total sputum volume comprised of sputum expectorated only during the treatment and immediately after. The volume expectorated throughout the day, which could have provided vital data for understanding the results, was not recorded. Further studies could be conducted to assess the effects of IMT on airway clearance in other pulmonary conditions.
Conclusion
Inspiratory muscle training was found to perform superiorly in terms of sputum clearance in patients with COPD.
Footnotes
Acknowledgments
The authors would like the participants of the study for their co-operation and Rajiv Gandhi University of Health Sciences for funding the study.
Conflict of interest
The authors have no conflict of interest to report.
Ethical considerations
This study was conducted in Father Muller Medical College, Mangalore from March 2019 to December 2022 after approval from the Institutional Ethics Committee (FMMIEC/CCM/602/2017). The study was registered under Clinical Trial Registry, India (CTRI/2017/07/009100). Participants were recruited from the inpatient admissions in Father Muller Medical College Hospital. The consulting pulmonologist and the primary investigator performed a detailed history taking and examination and screened the participants for eligibility based on the inclusion and exclusion criteria. Study procedure was explained to the eligible participants and written informed consent was taken.
Funding statement
This study was funded by Rajiv Gandhi University of Health Sciences.