
Abstract
COVID-19 pandemic did not impact all countries in the same way, and in Spain, the percentage of intensive care unit (ICU) and the mortality rate patients has been very high. The present work aims to present the first case of the new Coronavirus-2019 (COVID-19) on March 23, 2020, in Tenerife, Canary Islands, Spain, of a patient on Invasive Mechanical Ventilation (IMV) affected by acute pneumonia which was treated by airway clearance techniques (ACT) thinking that she was not infected with COVID-19, since the first polymerase chain reaction (PCR) test was negative. The subject presented septic shock, hypoxemic encephalopathy, and seizures. Right lung base consolidation and pleural effusion were visible in the echography. The thorax x-ray presented subcutaneous emphysema and pleural effusion in the right base and an alveolar-interstitial opacity pattern in the left. Bilateral crackles and rhonchus were evident in the right lung during the lung auscultation. The airway clearance protocol comprises Cough Assist (CA) and chest compressions. The variables collected were the ventilatory parameters, blood gas analysis, and thorax x-ray description. ACT protocol improves gas exchange and expands consolidated lung areas in this atypical clinical case presented. At that time, this type of treatment was not performed on patients affected by COVID-19, and the next day we found that the patient had improved, coinciding with the second PCR test, which was positive.
Introduction
March 11, 2022, marked the second anniversary since the World Health Organization declared COVID-19 a health emergency of international concern. While global health spending will continue to grow, it is expected to be unevenly distributed among countries. 1
In December 2019, severe pneumonia cases occurred in Wuhan, China, which we now know were due to the COVID-19 virus. The development of the new COVID-19 disease in northern Italy started at the end of February 2020, although it occurred earlier as a silent spread. 2 Although it was reported to be a mild or uncomplicated illness for most affected subjects, a small percentage of patients require hospitalization and oxygen therapy, and about 5% of subjects need to be treated with Invasive Mechanical Ventilation (IMV) at intensive care unit (ICU). 1 However, the pandemic did not impact all countries in the same way, and in Spain, the percentage of ICU and the mortality rate patients has been very high. 1
Between March and May 2020, severe acute pneumonia and acute respiratory distress syndrome (ARDS) caused by COVID-19 infection had a particular impact on older adults and those with comorbidities. 2 It was verified that for this clinical presentation, COVID-19 patients, once stabilized, should follow a rehabilitation program similar to those used to recover patients affected by pneumonia and acute disease.3,4
Pulmonary rehabilitation (PR) is essential during the different phases of ventilatory care. PR in the ICU played an important role. Whether patients received invasive or non-invasive mechanical ventilation, insufflation techniques to increase pressure support enhanced lung compliance and gas exchange by recruiting collapsed lung regions.5,6
In tracheotomised patients, the cough assistant improves lung volumes and accelerates the recovery of critically ill patients. They do not require IMV, including those with severe loss of breathing muscle force. 7 It became evident that using an ICU rehabilitation protocol in mechanically ventilated patients increased the success rate by improving oxygenation and expulsion of secretions, particularly at weaning from IMV. 8
ICU-acquired weakness (ICUW) impaired peripheral skeletal and respiratory muscles of affected critically ill patients. It was one of the most severe consequences of long-term immobilization, resulting in delayed weaning from MV and prolonged hospital stay. 9 In this context, rehabilitation should be initiated immediately after the acute phase to avoid the progression of hospital-acquired weakness and to achieve rapid functional recovery. 10
Since 2020, all human and technological health resources have cared for severe COVID-19 patients. 1 Implementation of early PR programs, among which ACT were highlighted, was considered an essential part of the treatment to improve the health of COVID-19 patients and avoid hospital collapse and patient complications resulting from a prolonged hospital stay. Different acute and subacute hospital care units specializing in the recovery of critically ill patients required early research and implementation of this topic. In this sense, the work of physiotherapists may be beneficial in the respiratory treatment and physical rehabilitation of COVID-19 patients. 11 Chiscano-Camón et al. 12 have demonstrated lower extubation failure by comparing a rehabilitation protocol (ACT + early mobilization) against usual care. The authors highlight the potential of pulmonary rehabilitation to decrease the extubation failure rate.
Two years later, knowledge about the pandemic has improved significantly. Therefore, understanding the presence and origin of possible sequelae experienced by post-COVID-19 patients should be an emerging priority for researchers and clinicians.13,14 Addressing these sequelae, early exercise and rehabilitation protocols applied during the patient’s hospitalization and after discharge from the hospital can help improve musculoskeletal pain symptoms and prevent functional deterioration. 15 Physical activity with multicomponent programs has positively affected function and weakness in COVID-19 infected patients and improved pain.16,17 COVID-19 has an evident functional impairment among other comorbidities. 18
The present work aims to present the first case of COVID-19 on March 23, 2020, in Tenerife, Canary Islands, Spain, of a patient on IMV affected by acute pneumonia, which was treated at ICU by ACT, thinking that she was not infected with COVID-19, since the first polymerase chain reaction (PCR) test was negative. At that time, this type of treatment was not performed on patients affected by COVID-19, and the next day we found that the patient had improved, at the same time the second PCR test was positive.
Case presentation
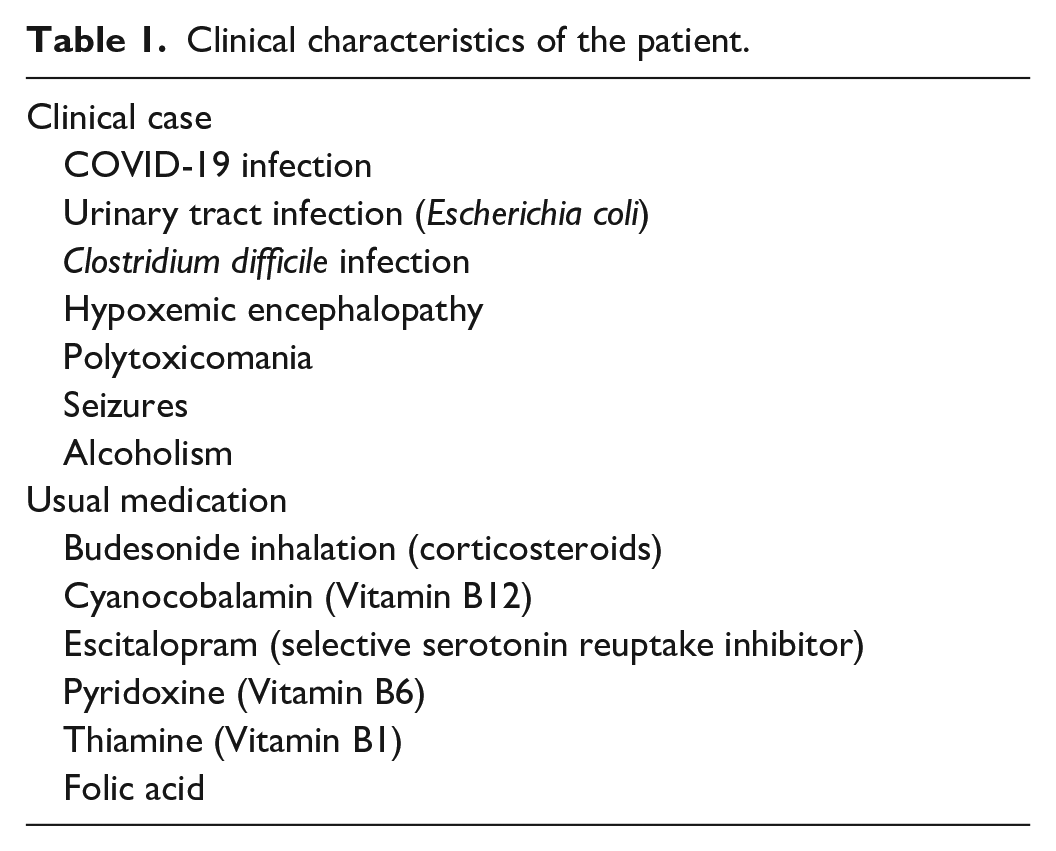
A woman with cardiac arrest, 43 years old, entered the ICU due to alcohol withdrawal syndrome. The subject presented with septic shock secondary to a urinary tract infection, hypoxemic encephalopathy, and seizures. The patient’s clinical characteristics are presented in Table 1.
Clinical characteristics of the patient.
On March 20, 2020, the patient was tracheostomised with an 8 mm cannula, with an orotracheal tube, after 10 days in Invasive Mechanical Ventilation (IVM). She presented a reduction of gas exchange (71 mmHg), needing increasing the ventilator (Evita, Drager, Germany) pressure support level (PS), positive end-expiratory (PEEP), and the fraction of inspired oxygen (FiO2). Echography demonstrated right lung base consolidation and pleural effusion, so it was drained less than 200 mL from the pleural space. However, the patient also presented with critical illness polyneuropathy and tried to contrast. She received standard pharmacological care regarding the pathology.
On day 1, the patient started physiotherapy treatment. The patient presented a fluctuating neurological state but was conscious, with eye closure and opening, without following any orders. The treatment goals were to expand the consolidated lung area, remove the secretions, and improve the gas exchange. The patient presented crackles and rhonchus bilateral during the lung’s auscultation, more evident in the right lung. She also presented pleural rubs in the right lung base.
Moreover, the patient presented hemodynamic stability with the administration of vasopressor. The thorax featured subcutaneous emphysema that surrounded the exit to the “Pleur-evac” system and was drained 400 mL from the pleural spaces before the evaluation. The thorax x-ray presented slight subcutaneous emphysema, small pleural effusion in the right base, and left base consolidation area with an alveolar-interstitial opacity pattern (Figure 1).

Day 1 x-ray: The thorax x-ray presented slight subcutaneous emphysema, small pleural effusion in the right base, and left base consolidation area with alveolar-interstitial opacity pattern.
The patient characteristics, ventilatory parameters, and blood gas analysis are shown in Table 2.
The patient characteristics, ventilatory parameters, and blood gas analysis.

CPAP/ASB: continuous positive airway pressure/assisted spontaneous breathing; cmH2O: centimeters of water; mL: milliliters; PEEP: positive end-expiratory pressure; mmHg: millimeters of mercury; pH: hydrogenic potential; bpm: beats per minute; FiO2: inspired oxygen fraction; mEq/L: milliequivalents per liter; mL/h: milliliters per hour; PaO2: partial pressure of arterial oxygen; PaCO2: partial pressure of arterial carbon dioxide; HCO3: bicarbonate; SpO2: blood oxygen saturation.
After a negative test for COVID-19, the ICU team discussed the utilization of CA (Cough Assist Philips E70) to reach the established goals. It was decided to apply two cycles of five insufflations without exsufflation with the following parameters:
Mode: manual
First cycle:
Five inspirations
Inspiratory pressure: 35 cm cmH2O
Mean flow: (200 L/m)
Inspiratory time: 4 to 5 s
Apnea pause: 3 s
No assisted exsufflation was carried out. Manual chest compression was performed during the expiratory phase (4 sec expiration). The first maneuver reached a tidal volume of 900 mL, measured by the mechanical ventilator.
Second cycle:
Five insufflations
Inspiratory pressure: 35 cm cmH2O
Mean flow (400 L/m)
Inspiratory time: 4 to 5 s
Apnea pause: 3 s
No assisted exsufflation was executed. Manual chest compression was performed during the expiratory phase (4 sec expiration). It reached 1500–1600 mL of tidal volume during the second cycle, measured by the mechanical ventilator.
After the therapy, the mechanical ventilator was reconnected. The pressure support was reduced to 12 cmH2O and PEEP to 8 cmH2O (Table 2). The respiratory frequency after the therapy was 35 movements per minute. Blood gas analysis was stable, and as the patient was fatigued, the ventilatory modality passed to bilevel positive airway pressure (BPAP).
On day 2 of rehabilitation, the patient presented during the daily assessment reduction in the mechanical ventilator parameters (Table 2). It also reduced vasopressors. The auscultation presented vesicular sound and reductions of crackles. There were also x-ray improvements: reduction of subcutaneous emphysema area, improvements of the alveolar-interstitial opacity, and improvements in the consolidated area in the left lung base. It was verified that 360 mL of pleural effusion drained (Figure 2).

Day 2 x-ray: reduction of subcutaneous emphysema area, improvements of the alveolar-interstitial opacity, and improvements in the consolidated area in the left lung base. It was verified 360 mL of pleural effusion drained.
After the treatment on the second day, we were informed that the patient was COVID-19 suspected. The patient was transferred to an isolated ICU. All the professionals involved during the first day of treatment were forced to quarantine. From that moment, it was not feasible to follow the patient’s progress. On the first day, the patient was not classified as a COVID-19 patient, as such we did not follow the recent guidelines of respiratory physiotherapy for COVID-19 patients. 19
Discussion
The clinical findings of this case report showed that the insufflation maneuver with CAs produced a short-term effect in acute lung injury patient COVID-19 positive. Early ACT achieved improvements in gas exchange and expansion of consolidated lung areas. Besides, the ventilatory support was reduced after the treatment. The late diagnosis of COVID-19 stopped the early rehabilitation as the patient was put in isolation but showed that lung recruitment maneuvers, when conducted by expert physiotherapists, may have potential benefits.
The decisions taken by the hospital’s medical and physiotherapy team were based on the urgency of the clinical case and the lack of knowledge of COVID-19 infection. It is necessary to consider the historical context in which the clinical case developed. There is no consistent, evidence-based approach for patients affected by COVID-19 with severe respiratory symptoms.
Unlike the standard care,20,21 CA insufflation-only mode was performed as the patient’s characteristics worsened. The objective was to recruit the lung and re-open the left base since it was found that inspiratory volumes were decreased and oxygenation was worsening.
It was decided to increase flows and pressures until insufflation volumes above 1200 mL were achieved to recruit the lung. Therefore, two progressive cycles were performed until the proposed objective was achieved.
This modality was decided even though the patient had subcutaneous emphysema because the objective of this therapy was to recruit collapsed alveoli. It was verified that the pleural tube placement was correct, and the subcutaneous emphysema was on the way to recovery with good resolution. The patient’s respiratory worsening required ACT treatment focused on opening the left base and reducing edema with positive pressures, anticipating that there would be respiratory improvement after the use of CA if lung recruitment was achieved. The use of CA has always been used with an inflated pneumonia so as to avoid loss of pressure.
The radiographs were taken on consecutive days, with a 24-h difference between the two, proving the radiographic improvement. The ventilator setting improved during the 24 h. The pressure support was reduced from 20 cmH2O to 12 cmH2O. The PEEP improved from 10 cmH2O to 8 cmH2O. It preserved the physiological characteristics of the patient’s lung. Thanks to improved respiratory parameters just after using CA, MV was maintained for 1 h to avoid respiratory muscle exhaustion caused by the CA. However, blood gases and volumes showed an improvement in respiratory parameters that allowed the ventilator pressures to be decreased over the next 24 h.
The exceptional feature of this case is that it was the first COVID-19 case in Tenerife, Canary Islands, Spain, and that it was treated with ACT by CA. However, given the false-negative first testing, the patient was initially treated as a standard respiratory failure. It was a chance that the patient was infected with COVID-19.
Rehabilitation of COVID-19 survivors is the next pandemic challenge. Currently, post-COVID-19 patients that need MV are treated with PR. 10 Those patients present restrictive disorders, mild hypoxemia, sarcopenia, and exertional intolerance. These subjects are usually evaluated with the 6-min walk test, pulmonary function tests, and blood gas analysis. 22 PR may improve those impairments, including aerobic and strength exercise training, respiratory physiotherapy, and pharmacological treatment.8–12,20
It is observed that patients following a PR protocol8–12 improve functional status, peripheral saturation during exertion, and dyspnea.
Conclusions
The use of the treatment showed that CA, in this case, played a fundamental role in the respiratory recovery of the patient described, a highly complex case due to her clinical characteristics.
Research in treating patients with pneumonia secondary to COVID-19 infection in IMV at the ICU is encouraged.
Footnotes
Acknowledgements
The authors thank the entire medical and physiotherapy team of the Hospital Universitario Nuestra Señora de Candelaria, Tenerife, Spain. This study was supported by the Italian Ministry of Health—Ricerca Corrente 2021.
Author contributions
Conceptualization, J.H.V. and E.A.S.R.; methodology, J.H.V. and E.A.S.R.; software, J.H.V.; validation, all authors; formal analysis, C.C.., E.A.S.R., and J.H.V.; investigation, all authors; resources, J.L.A.P.; data curation, J.H.V., E.A.S.R., and C.C.; writing—original draft preparation, J.H.V., I.V.S., and E.A.S.R.; writing—review and editing, E.A.S.R., I.V.S., C.C., and J.H.V.; visualization, E.A.S.R. and J.H.V.; supervision, all authors; project administration, E.A.S.R. and J.H.V.; funding acquisition, J.L.A.P. All authors have read and agreed to the published version of the manuscript.
Data availability statement
Data are available on request due to privacy and ethical restrictions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient to publish this case report and any accompanying images.