
Abstract
BACKGROUND:
The prevalence of knee osteoarthritis is increasing due to population growth, ageing and other risk factors. However, the majority of patients can successfully manage their symptoms using conservative management strategies with only a minority requiring surgery. In 2019, a patient waited four years to be seen if deemed routine for an elective orthopaedic out-patient appointment in a large acute hospital in Ireland.
OBJECTIVE:
To establish a Fast-Track Knee Pathway in an Irish healthcare setting, creating a more efficient channel into elective orthopaedics for patients requiring surgical intervention whilst providing community-based care for those with non-surgical needs.
METHODS:
a) Establishment of a dedicated community-based physiotherapy and dietetic service for knee osteoarthritis, b) implementation of a Rapid Access Knee Clinic in elective orthopaedic clinics, and c) economic evaluation of the Fast-Track Knee Pathway’s cost effectiveness compared with the traditional pathway.
RESULTS:
403 patients with knee osteoarthritis were removed from physiotherapy waiting lists with 9 patients requiring referral onwards to the Rapid Access Knee Clinic. On average there was a 64% reduction in wait time to access an orthopaedic consultant across 4 pilot sites. An incremental cost-effectiveness ratio of € 22,535.03 per QALY was estimated. Comparing this to the national accepted threshold of € 45,000 per QALY the Fast-Track Knee Pathway can be considered cost-effective.
CONCLUSION:
The Fast-Track Knee Pathway provides a fully integrated pathway of care for patients with knee osteoarthritis, facilitating earlier access to orthopaedic intervention. An economic evaluation concluded that this model of care is more cost-effective than the traditional pathway.
Introduction
The Irish Longitudinal Study on Ageing (TILDA) study estimated overall osteoarthritis (OA) prevalence rate at 12.9% in the Irish population over 50 years of age [1]. Estimated global prevalence of knee OA was 22.9% in individuals aged 40 and over in 2020, with a prevalence of 13.4% in Europe [2]. Projections of population growth, ageing and other risk factors will increase dramatically the burden of musculoskeletal disease over the coming decades [3] with OA significantly impacting quality of life due to increased pain [1], sleep interference [1, 4], fatigue, emotional stress [4] and limitations in activities of daily living and social participation [1].
There are a number of pathways described internationally which address delivering models of care and implementing more efficient clinical pathways for knee OA across both primary and secondary care [5–7]. In the Netherlands BART (Beating osteoARThritis) provides a stepped care strategy to optimize the utilization and timing of conservative treatment options [5]. The Osteoarthritis Chronic Care Program (OACCP) in Australia utilizes a musculoskeletal coordinator to assess and link patients with relevant health care providers to ensure a flexible and individual response to patients’ needs [6]. Also in Australia, the Orthopaedic Wait List (OWL) project developed a prioritisation tool which could be used to monitor patient symptoms whilst on an orthopaedic waiting list to assist in identifying deterioration and facilitating timely surgery [7].
In 2019, a patient waited on average four years to be seen if deemed routine and two years if deemed urgent for an elective orthopaedic out-patient (OPD) appointment in a large acute hospital in Ireland. Within the orthopaedic OPD there was in excess of 8,000 patients awaiting appointments. During the pandemic national elective OPD waiting lists further grew by 15.1% with a 61.4% growth in those patients waiting 12 months or more [8].
We know from our local data audits that only a minority of knee OA patients (20%) are listed for surgery, while the remaining are managed through non-surgical interventions [9]. However, both cohorts of patients are often triaged to the same waiting list and wait similar lengthy periods to be seen in orthopaedic OPD despite them having very different needs.
The Fast-Track Knee Pathway is a care pathway for patients with knee OA with improved integration of primary and secondary care services. Dedicated physiotherapists and dietitians ensure quicker access to community-based intervention with additional accelerated access to an orthopaedic consultation for patients who require further review and intervention.
Established in 2020, the Fast-Track Knee Pathway aims to create a more efficient channel into elective orthopaedics for patients who were more likely to need surgical intervention whilst providing local, community-based conservative management for those with non-surgical needs.
The objectives of the Fast-Track Knee Pathway include: Establishment of a dedicated community-based physiotherapy and dietetic service for knee OA. Implementation of a Rapid Access Knee Clinic in elective orthopaedic clinics in an acute hospital setting. Economic evaluation of the Fast-Track Knee Pathway’s cost effectiveness compared with the traditional pathway.
Methods
Study population
The study population consists of patients on elective orthopaedic and physiotherapy waiting lists in an Irish healthcare catchment area with a population of over 580,000 [10]. Elective orthopaedic services are provided in the acute hospital setting with physiotherapy provided in community-based healthcare settings for the region [11].
Patients with chronic knee pain are referred to public physiotherapy services within the community healthcare setting by their GP. In 2019 local audit results reported over 1,000 patients with knee pain waiting on physiotherapy waiting lists in this catchment area with wait times in excess of two years in several sites [9].
Patient involvement
The objectives of the study were based on patient feedback from previous service-user experience surveys on the baseline service. Patients were not involved in the setting of outcome measures or the specific implementation of the study but played a role in disseminating the results by participating in reporting of project outcomes and patient experience.
Fast-track knee pathway project design
Four pilot sites across two counties within the catchment area were chosen to establish a dedicated physiotherapy and dietetic service for patients with knee OA. A Rapid Access Knee Clinic was also established in the orthopaedic services in the acute regional hospital.
Two part-time senior physiotherapists were specifically recruited in both counties to deliver community-based physiotherapy for patients with knee OA. The physiotherapists selected all patients aged over 40 years with chronic knee pain from the physiotherapy waiting lists in the respective pilot sites which included a combination of adult musculoskeletal and non-musculoskeletal referrals. Patients were initially offered an individual consultation in chronological order. Based on the outcome of the consultation patients were offered either a place in a group knee class or individual care in line with evidence-based guidelines [12]. The group knee class format comprised a five-week exercise and education programme tailored to each patient’s needs with participants attending once weekly for approximately one hour. Due to the various waves of Covid-19 and fluctuating restrictions, physiotherapy care was offered via in-person and telehealth at different time points during the project period.
A part-time senior dietitian was also specifically recruited to cover all four pilot sites to deliver community-based dietetic care for patients with knee OA. Patients with chronic knee pain selected from the community physiotherapy waiting lists were invited to avail of dietetic care. Due to Covid-19 restrictions and the geographical base of the dietitian outside the pilot sites, care was delivered via telephone. The dietitian also pre-recorded a 20-minute educational video on components of a healthy diet, portion control and weight management strategies which was shown to patients attending both in-person and telehealth physiotherapy consultations as appropriate.
A Rapid Access Knee Clinic was established by the orthopaedic department in the regional hospital. On completion of the physiotherapy care programme outlined above, patients who satisfied specific inclusion criteria for an orthopaedic consultation were booked into the Rapid Access Knee Clinic. Inclusion criteria included mono-articular knee OA with x-ray confirmation, duration of symptoms > 3 months, Oxford Knee Score (OKS)<20 [13] and patient desire for intervention in relation to potential injection therapy and surgery. A part-time clinical specialist physiotherapist was also specifically recruited to work in orthopaedic OPD clinics in the acute hospital setting to ensure that rapid access knee referrals were appropriate and to facilitate fast-tracking to an orthopaedic consultant clinic. The key project performance indicator identified at project outset was a reduction in physiotherapy wait time to four months in the pilot sites.
Data collection
Patient outcome measures were collected at the initial physiotherapy consultation and again seven weeks later on completion of their course of care. The Oxford Knee Score (OKS) was the main outcome measure used to collect data on patient clinical outcome and was also used to conduct the Cost Effectiveness Analysis (CEA). The OKS is a previously validated outcome measure based on a 12-item questionnaire. Participants can have a total score of 0 to 48, where 48 indicates the best possible outcome [13].
The second measure, the EQ-5D-5 L, measures health-related quality of life on five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. The EQ-5D-5 L has widespread availability, is generally easy to use and interpret, and is based on preferences of the general population [14]. Irish weighting is also available for EQ-5D-5 L scores [15].
Economic analysis
The economic analysis followed methodology for economic evaluations as detailed in national Health and Information Quality Authority (HIQA) guidelines [14]. The base case analysis was a Cost Utility Analysis (CUA) comparing incremental costs to incremental benefits in terms of quality-adjusted life years (QALYs). The Health-Related Quality of Life (HRQoL) outcome data (EQ-5D-5 L) were converted to utility values using the Irish weighted values [15], which were then adjusted for time to calculate QALYs as recommended by national guidelines. A Cost Effectiveness Analysis (CEA) was also conducted comparing incremental costs to incremental change in the OKS. The perspective of the analysis is from that of the healthcare provider and payer (Health Service Executive (HSE).
The pathway delivery costs included direct resource and material costs which were identified and valued using standard national guidelines [14] in 2022 euro, applying appropriate unit costs. A conservative “do nothing” approach was adopted for both CUA and CEA which assumed that for the traditional pathway, no change in costs or outcomes occurred during the period.
Results
Physiotherapy and orthopaedic wait times
Four hundred and three patients with knee OA across four selected pilot sites were removed from physiotherapy waiting lists between October 2020 and December 2021. Nine of these patients required referral onwards to the Rapid Access Knee Clinic in the acute hospital setting with all patients seen within four weeks of referral. Initial physiotherapy intervention consisted of individual in-person and telehealth consultations in October 2020. In-person classes commenced in September 2021 and a hybrid model of individual in-person/telehealth and group in-person consultations continued until the end of the project period in December 2021. Dietetic intervention was via telephone only during the project period with 12% of patients (n = 47) availing of this service for weight management care.
On average there was a 64% reduction in wait time to access an orthopaedic consultant across the four pilot sites. In October 2020 there was an average wait of 36 months to access an orthopaedic consultant across all four pilot sites. This reduced to an average of 13 months by December 2021 at the end of the project period. Two sites (Site 2 and Site 4) reduced the wait time for physiotherapy to under four months. Patients in these sites identified as requiring orthopaedic input were seen within seven months of initial GP referral to physiotherapy (Fig. 1). This represents up to five times quicker access to orthopaedics than the traditional pathway. The remaining two sites (Site 1 and Site 3) had wait times of 17 months and 21 months respectively from initial GP referral to physiotherapy at the end of the project period. Covid-19 restrictions resulted in reduced capacity to run group classes and this impacted on the rate of reduction of physiotherapy wait lists. Sites which resumed group classes at an earlier date achieved shorter physiotherapy wait times. The project also experienced high staff turnover due to recruited staff changing roles for permanent job opportunities. This resulted in vacant positions which required recruitment and training of new staff.
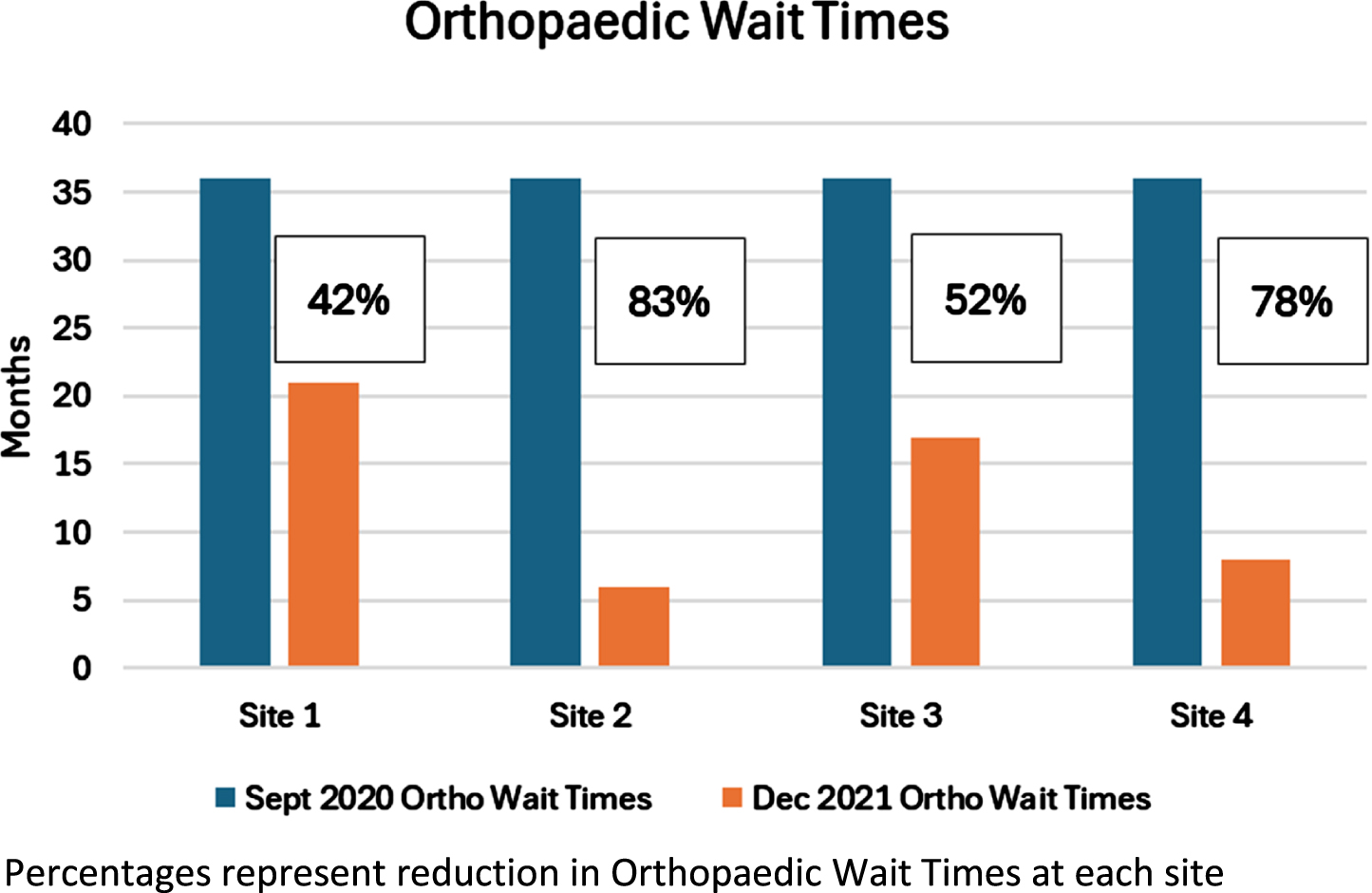
Reduction in orthopaedic wait times.
Clinical outcomes, measured using the Oxford Knee Score (OKS) demonstrated an overall improvement from baseline to re-evaluation at seven weeks. From Table 1.0, we see the mean baseline OKS was 24.92 while the mean OKS at 7 weeks was 32.30 which yields a mean difference in OKS of 7.38.
Oxford Knee Scores –Fast-Track Knee Pathway
Oxford Knee Scores –Fast-Track Knee Pathway
OKS –Oxford Knee Score.
Table 2 below details the QALYS gained by the Fast-Track Knee Pathway group in the 7-week period. The Fast-Track Knee Pathway group gained 0.02 QALYs which we consider to be the incremental effectiveness between Fast-Track and the traditional pathway.
QALYs –Fast-Track Knee Pathway
QALYs –Fast-Track Knee Pathway
QALYs –Quality-Adjusted Life Years.
Table 3 outlines the results of both the CUA and CEA. The CUA compared the incremental costs of the Fast-Track Knee Pathway (€ 445.20) and the incremental gains in QALYs (0.02). An incremental cost-effectiveness ratio (ICER) of € 22,535.03 per QALY was estimated. Comparing this to the national accepted threshold of € 45,000 per QALY [14] the Fast-Track Knee Pathway can be considered cost-effective. For the CEA, the incremental change in OKS was 7.38 which yielded an ICER of € 60.30 per point change in OKS.
Economic evaluation –cost utility analysis and cost effectiveness analysis
CUA –Cost Utility Analysis; CEA –Cost Effectiveness Analysis; QALYs –Quality Adjusted Life Years; ICER –Incremental Cost Effectiveness Ratio.
The Fast-Track Knee Pathway resulted in a 64% reduction in wait time for an orthopaedic consultation in a large regional acute hospital. The reduction in wait time fluctuated across the pilot sites due to a variety of physiotherapy-related factors including staff availability, access to facilities to run group classes and local Covid-19 restrictions. Once physiotherapy treatment was complete, all suitable patients were seen in the orthopaedic department within four weeks of receipt of referral. A total of 2% (n = 9) of patients seen in physiotherapy were referred to the Rapid Access Knee Clinic in the acute hospital setting. It is unclear if Covid-19 influenced this outcome with patients reluctant to attend an appointment in the acute hospital setting or to pursue a surgery treatment option.
Similar to the musculoskeletal coordinator described in the Australian OACCP model of care [6], the clinical specialist physiotherapist was a common link between stakeholders, ensuring that the patient received the most appropriate level of treatment for the stage of their condition. In contrast to the OACCP model the patient journey in the Fast-Track Knee Pathway always begins at community level with GP referral to community physiotherapy to avail of first-line recommended treatment [12]. Depending on a patient’s symptom and disease severity the clinical specialist physiotherapist can intervene to accelerate their access to orthopaedic consultant option as early as required. The Australian OACCP model of care accepts referrals from multiple sources with patients not always entering the programme from community level [6]. Both programmes demonstrated improved clinical outcomes with the OACCP model additionally reporting up to 11% removal of patients from surgical wait lists as a result of the programme [16] As the Fast-Track Knee Pathway further develops it too should expand its accessibility to patients currently on orthopaedic and knee surgery wait lists who may also benefit from its offerings.
The results of the CUA suggest that the Fast-Track Knee Pathway is cost-effective, albeit with a degree of parameter uncertainty in terms of effectiveness. The Fast-Track Knee Pathway is more costly, but it delivers more benefits in QALYs (0.02) than the traditional pathway. An ICER of € 22,535.03 per QALY was estimated which falls well below the proxy ceiling of € 885.48/point change in OKS. Whilst there is uncertainty in the effectiveness values, both CUA and CEA suggest that the Fast-Track Knee Pathway is highly cost effective. The ICERs for both analyses are significantly below the willingness to pay thresholds which would suggest that only changes of scale in variables would affect the decision of cost-effectiveness of the Fast-Track Knee Pathway. Further studies may be of interest to include some of the parameters that were absent in this study including healthcare utilisation costs or related costs such as absenteeism or disability.
Strengths and limitations
Although the scope of the current analysis is narrow, the Fast-Track Knee Pathway would appear to be highly cost-effective as an intervention for knee OA. The model of care is also reproducible within the Irish healthcare system.
No clinical or demographic profile of the patients who went through the pathway was provided in this study. It is also unclear if patients who did not get referred to the Rapid Access Clinic subsequently required input from the orthopaedic service for a surgical opinion. Lack of detailed clinical data in relation to the impact of the dietetic service is also a limitation of this study. The main focus of the project was the implementation of both a dedicated physiotherapy and dietetic service for patients with knee OA and the subsequent effect on orthopaedic consultation wait times. In contrast to physiotherapy, clinical outcomes for dietetic input were not collected and future studies should include such data to fully understand the benefits of the pathway.
Implications for policy, practice and research
The Fast-Track Knee Pathway provides a framework which can be easily modified and replicated in other sites and for other chronic musculoskeletal conditions. The physiotherapy and dietetic interventions described are in line with standard, recommended practice [12], it is only the referral pathway that requires modification. The pathway permits flexibility for implementation in line with local organizational structures and facilities but will require collaboration and engagement from relevant stakeholders across both primary and secondary care. With an increased focus on the delivery of services which focus on prevention, community care and integration of care across all health and social care settings [17], the Fast-Track Knee Pathway is ideally positioned to improve accessibility to high-quality care for patients with chronic musculoskeletal conditions.
Conclusion
The Fast-Track Knee Pathway resulted in a 64% reduction in wait time for an orthopaedic consultation and demonstrated the pathway as a cost-effective model of care. The Fast-Track Knee Pathway provides a fully integrated pathway of care for patients with knee OA, facilitating earlier access to orthopaedic intervention. This results in a more seamless patient journey from initial GP referral through to orthopaedic intervention if required. The inclusion criteria for the Rapid Access Knee Clinic helps to prioritize patients with the most urgent needs and who have exhausted all evidence-based conservative treatments. Findings of both the CUA and CEA conclude that this new model of care is more cost-effective than the traditional pathway.
The pathway is novel in an Irish healthcare setting and provides a template at national level which can be reproduced in other sites and for other musculoskeletal conditions. Future pathway developments will require similar dedicated staff for such pathways to be successful.
Funding
This work was supported by funding acquired from the Irish Department of Health: Sláintecare
Integration Funding – Grant number 324 https://www.gov.ie/en/press-release/a98320-minister-for-health-announces-20-million-funding-for-122-slaintecare/
Footnotes
Acknowledgments
The authors acknowledge South-East Community Healthcare Physiotherapy and Dietetic Departments and University Hospital Waterford Physiotherapy Department who contributed to facilitating this project.
Conflict of interests
There are no competing interests to declare.
Ethics approval
This project was Quality Improvement in nature and not subject to local Ethics Committee oversight.