
Abstract
Objective
To review challenges associated with health economic studies in rehabilitation, providing a context for the new Clinical Rehabilitation collection of papers concerned with health economics.
Rehabilitation
Analysis of the health economic effects associated with rehabilitation must recognise that rehabilitation consists of both a problem-solving process that facilitates the person's adaptation by providing information, advice, and sometimes specific interventions targeting multiple areas. Second, it operates within a complex, adaptive system, specifically the biopsychosocial model of illness. Third, its goals are to enhance well-being and quality of life through its effects on lower-level systems. Consequently, the effects of rehabilitation are unpredictable and typically manifest in several domains. Comprehensive single or multiple focused outcome measures are needed. As evidence-based selection of people who might benefit from rehabilitation is impossible, evaluative studies should have broad inclusion criteria.
Systems
Rehabilitation is a healthcare service. Traditionally, it is delivered in series, after the biomedical treatment has ended. This allows researchers, including health economists, to isolate the influence of rehabilitation. However, it will be more effectively delivered in parallel, with biomedical care from the outset, as happens, for example, in trauma and intensive care units. Evaluating individual components of healthcare in isolation is unnecessary. Rehabilitation will always involve non-healthcare services. Conversely, the effects of rehabilitation may significantly reduce non-healthcare costs. This close interrelationship necessitates a societal perspective on the economics of rehabilitation.
Conclusions
Using a combination of a global, comprehensive clinical outcome measure and societal-level health economic data will increase the likelihood of detecting effects.
Introduction
Why are health economics of interest to rehabilitation? For many years, rehabilitation was considered ineffective. This belief justified the low allocation of resources. Resources remain inadequate despite the emergence of strong evidence of effectiveness. 1 The perceived relative expense of rehabilitation may be used to justify not providing sufficient resources.
Health economic studies indicate that rehabilitation provides significant value for money. For instance, a study from Australia concluded that investing one Australian dollar in rehabilitation saved A$$91 in long-term costs. 2 A similar study in the UK on highly specialised inpatient rehabilitation found that costs were recovered within 3 years. 3
In 2016, a systematic overview of economic evaluations of health-related rehabilitation
4
identified 64 systematic reviews. Although all study designs were included, many evaluations were concurrent with randomised trials. The authors concluded that the evidence showed:
Some interventions were effective, but cost more Some comparisons showed one intervention to be cheaper and equally effective Some studies found cost savings across various budgets, including health, social services, and employment.
Rehabilitation research must consider health economic outcomes to increase the evidence and sustain our services; most healthcare now undergoes health economic evaluation, and we cannot fall behind. This editorial highlights several key issues for readers and researchers. It advocates that most rehabilitation research should use global outcome measures and, where possible, include a health economic perspective. Indeed, health economic data could serve as the most meaningful primary outcome for many rehabilitation studies. It also introduces a new collection of health economic papers published in the journal.
Clinical rehabilitation collections
Clinical Rehabilitation first published three collections of papers about specific topics in early 2020. It will soon have five.
In the last 39 years, Clinical Rehabilitation has published at least 30 papers focused on the health-economic aspect of rehabilitation, including two papers in 2025.5,6 Given the importance of health economics, we have developed a fourth collection to add to the three published in 2020.
The collection includes all papers that concern or are relevant to health economics. In addition to research papers reporting economic analyses of randomised trials, we have included documents on methodology, measurement, and other aspects of health economics. They join numerous studies on economic aspects of rehabilitation published in a wide range of other journals.
Our health economics collection includes two essential papers on the UK context, written by Professor Turner-Stokes and her colleagues at Northwick Park Hospital, that have influenced costing and funding decisions in the UK.7,8
Soon, a fifth collection of the papers chosen as the Editor's Choice each month joins the other four collections, so they will cover:
Health economics
Health economics is not restricted to the financial cost of healthcare. The University of York's Health Economics Consortium defines it: ‘Health economics is a field of economics that focuses on the “analysis and understanding of efficiency, effectiveness, values and behaviours involved in the production and consumption of health and healthcare”’. 9
A recent review
10
identified five key types of comparative evaluation:
Cost-effectiveness: relative costs and a single outcome of disability (or life) Cost-utility: relative costs and an outcome combining life and disability (e.g., disability-adjusted life-years) Cost-benefit: costs and outcomes, where outcomes are expressed in monetary terms Cost-minimisation: costs, assuming the same outcome is achieved Cost-consequence: relative costs and multiple outcomes (e.g., pain, function, well-being)
The outcome measured will affect the type of analysis used. For example, many rehabilitation trials will measure outcomes across several domains, and a cost-consequence analysis allows for the evaluation of the effect on each.
The quality of a health-economic comparative study can be assessed using the updated Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) statement. 11
Is rehabilitation an intervention?
Rehabilitation is a slippery word. Sometimes it refers explicitly to a specific therapy, such as gait retraining; sometimes its use is more generic, referring to receiving occupational therapy or vocational rehabilitation; occasionally, it relates to providing aids, adaptations, prostheses, or medications.
Biomedical research assumes that the initial assessment and diagnosis of the specific cause (disease) has occurred and compares different particular treatments. Rehabilitation is based on a different model of health, the holistic biopsychosocial model. 12 The initial assessment and formulation identify multiple factors that need to be altered; there is no single cause or specific treatment. The term rehabilitation encompasses both the initial analytic phase and the various treatments.
An example illustrates the confusion. In a systematically developed definition, rehabilitation is referred to as a ‘multimodal, person-centred, collaborative
It is better to distinguish between the two basic meanings. The first is that rehabilitation refers to a healthcare problem-solving process that involves analysing the situation to reach a formulation and developing a plan, typically comprising multiple actions based on the analysis. 14 This corresponds to the initial phase of biomedical care, and formulation is analogous to the biomedical term diagnosis.
The second meaning refers to the actions undertaken by a rehabilitation team. These actions are usually complex, but their goal is to catalyse and facilitate the person's adaptation to their illness. 15 This is equivalent to biomedical treatments using drugs, surgery, or other interventions.
Therefore, as far as possible, health economic studies should make explicit whether the experimental part of the study includes the phase of assessment, formulation, and planning, or whether the investigation only considers the ‘treatment’ phase, studying an intervention exclusively. This is essential because many of the benefits of rehabilitation may arise from an accurate analysis of the clinical situation and giving precise information and advice. 15
Therefore, if randomisation occurs after the patient's assessment period, when judged suitable for either of the options being evaluated, the trial is considering a specific intervention. All other designs incorporate the influence of assessment, formulation, and advice, and the trial evaluates the effectiveness of achieving a formulation
Rehabilitation interventions, after formulation
Once the rehabilitation team has an accurate formulation, it will plan actions which vary greatly, from providing information and giving advice to helping a person learn new skills, with many additional actions such as organising housing alterations. Figure 1 gives an overview of rehabilitation's roles as conceived by the General Theory of Rehabilitation, 15 identifying several distinct classes of action that may be necessary on the right-hand side.
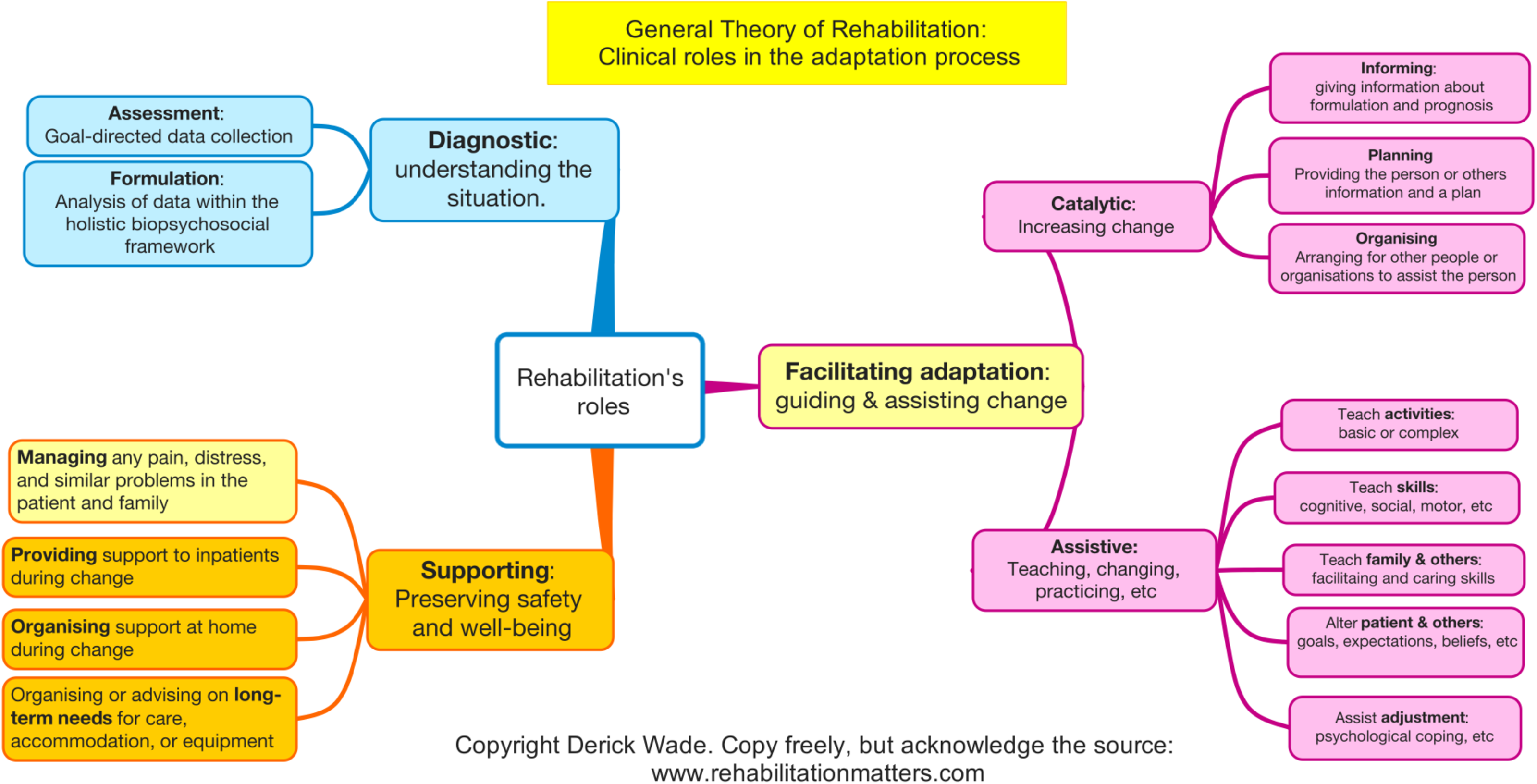
Overview of rehabilitation's roles and types of specific intervention.
The Medical Research Council developed a framework for evaluating complex interventions.
16
They gave examples of how an intervention might be complex. A review of effective rehabilitation
1
demonstrates that rehabilitation interventions have all the features of a complex intervention mentioned by the Medical Research Council:
Many components Targets many behaviours Specific expertise and skills are needed
17
Many groups, settings, and levels may be targeted Flexibility and tailoring of components
The Medical Research Council (MRC) framework emphasises that complexity arises from the components and their interactions with the system or context in which they are deployed. The healthcare system and the patient are complex adaptive systems, 18 which complicates the evaluation of their effects because system adaptation may amplify or negate the desired change.
The challenges associated with health economic evaluations of complex interventions were discussed in 2008 by Alan Shiell et al., who argued that complexity is a property of a system, not an intervention. 19 They stress that the relationships between an intervention and its intended effects are rarely linear, and, more importantly, distal effects on other outcomes may be larger and not predicted.
Rehabilitation inevitably involves many other organisations such as social services, housing, employment, and education. This significantly affects the rehabilitation process, as some vital rehabilitation actions depend on and are funded by non-health agencies. Conversely, non-health budgets may benefit from health-funded actions.
Therefore, health economic studies of rehabilitation must consider both resources used and benefits from a societal perspective, because focusing only on healthcare costs and benefits risks overlooking broader costs and benefits.
Service organisation
Traditionally, specialist rehabilitation has been provided after biomedical treatment. A patient is first managed by an acute medical, surgical, psychiatric or other service. Once the biomedical phase is complete, they are transferred to rehabilitation.
This suits researchers, as it reduces the variance introduced by biomedical treatments, and managers, as it increases their control over the service and its budget. The patient, however, will start adapting to their limitations immediately, and the sooner a rehabilitation service is involved to guide and facilitate adaptation, the better.
Thus, rehabilitation services should be delivered in parallel with other healthcare. 20 This is happening. For example, rehabilitation is now offered in intensive care units with some benefits,21,22 and delivery of rehabilitation in hyperacute rehabilitation services is developing significantly, usually in association with trauma services. This approach is likely more efficient and effective.
This model of service delivery may complicate the identification of the unique contribution of rehabilitation to the outcome. However, at present, we do not know the unique contribution of the biomedical diagnostic process to any outcome. Our concerns should be with efficient and effective services, rather than the unique contribution of any one component.
The patient is not interested in whether the medical or rehabilitation input is helping; their interest, as well as that of the clinical teams, is in the outcome. Indeed, one could argue that research comparing the effects of parallel and in series service organisation should have a high priority, with an explicit focus on health economics.
Choice of outcomes
Research into the effectiveness and cost-effectiveness of targeted actions can be conducted using traditional methods. Since rehabilitation has broader and less predictable effects than most biomedical interventions, typically several outcomes are measured, covering a range of possible benefits. Moreover, effects typically take longer to become evident than in biomedical research, and patient outcomes should be measured months or even years later.
The paradigmatic trial design specifies a primary outcome, which is typically the variable directly and specifically affected by the treatment, because that reduces variance caused by other influences. However, rehabilitation is characterised by many interventions, each aimed at a different factor; the paradigm does not apply, but rehabilitation researchers and funders still like a proximal primary outcome.
There are now many suitable global measures of rehabilitation outcomes, such as the World Health Organisation's Disability Assessment Scales (WHO DAS), which have been well-developed.23–25 Other measures include subjective well-being26,27 and the EuroQol 5D-5L.28,29 It could be argued that other factors may influence global measures; however, a counterargument is that their broad scope increases the likelihood of capturing crucial benefits unrelated to the implicit target of the treatment.
In two studies of rehabilitation after traumatic brain injury,30,31 most patients only needed initial assessment and advice, not specific treatments. 32 The benefits of general advice can only be detected using global measures because the range of potential benefits is vast, including, for instance, reduced emotional distress due to lessened uncertainty and inappropriate expectations.
There may be a few patients entering rehabilitation who will not require any treatment and for whom no helpful advice can be given. Even then, the assessment will benefit patients by reassuring them that nothing more is needed, thereby preventing a fear of missing out on a potentially beneficial treatment, and avoiding repeated or prolonged attendance at other health services seeking help.
The addition of data on resource use as an outcome ensures the broadest possible perspective. The benefits may include less use of resources across many domains; someone may return to work more quickly, be provided with equipment to reduce the need for carers, or may stop seeking further help and adapt faster. These hidden effects can only be captured using health economic data. Crucially, a relatively small benefit in most people will have more impact than a large effect on a few selected and atypical patients.
In summary, any research evaluation investigating the effects of a rehabilitation that includes undertaking an assessment should use a global measure of outcome and a societal measure of resources used by the individual to maximise the likelihood of detecting benefit; the outcome should be measured at least 6 months after starting, and preferably at 12 months. Policymakers and public funding organisations should also consider overall societal benefits when allocating resources.
Practicality
This inclusive approach to rehabilitation and its evaluation appears daunting. One is recruiting all patients presenting with a condition. However, it has been done. Many of the trials investigating stroke unit care were, in effect, investigating all patients receiving rehabilitation. 33 The two studies on rehabilitation after head injury also included all patients.30,31 A current study of vocational rehabilitation is also investigating the whole rehabilitation process, with clinical and health economic outcome data. 34
Nevertheless, many researchers and funding organisations would prefer to select people who might benefit or, alternatively, to exclude people who will not be helped. These are laudable aims but cannot be achieved.
First, as emphasised above, being seen and reassured that no further action is needed is often very therapeutic. Just consider the effect of being told that the lump you felt is not cancer.
More importantly, there is no valid way to determine who has ‘rehabilitation potential’. 35 The concept is itself ill-defined; for example, it usually includes the idea of improving some functional activity. However, no person with a complete thoracic spinal cord injury will ever achieve any improvement in their personal mobility, yet they have vast potential. My recent review concluded, ‘The solution is to offer all people not recently seen by an expert multi-professional rehabilitation team a full rehabilitation assessment and formulation, which will reveal what rehabilitation might achieve’. 35
Conclusions
When comparing two types of rehabilitation, it is essential to assess outcomes using a comprehensive measure of disability or life satisfaction, or both, as well as gathering health-economic data on resources utilised. These outcomes should be measured at 6 and 12 months after the start.
This method will maximise the likelihood of identifying the effects of rehabilitation across various affected domains. Each study should include inclusive selection criteria that encompass any individual who might benefit. Therefore, simple data collection tools are necessary, capable of easily acquiring data from participants. This approach would significantly increase the evidence about the effects of rehabilitation.
When studying a single treatment that might be suitable for many people with various conditions, the same advice applies because the incidental, unpredictable benefits will be detected, and it will also enable meta-analysis of data from many trials.
Clinical messages
Existing health economic studies suggest that rehabilitation reduces long-term societal costs.
They also provide data on a few specific rehabilitation interventions.
Future studies should use global clinical outcomes and economic data as their primary measures.
Footnotes
Acknowledgements
I am grateful for being introduced to health economics in my first research project in 1980, and for the support I have received from experts since then. I would like to extend my special thanks to the two reviewers, Audrey Bowen and Natasha Brusco, who provided many stimulating and engaging comments that substantially improved this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.