
Abstract
BACKGROUND:
Falls have a detrimental effect on Ireland’s ageing population and result in a significant personal and healthcare cost burden. Evidence-based falls prevention programmes reduce the harmful effects of falls. The Covid-19 pandemic disrupted in-person programme delivery and necessitated a shift to telerehabilitation. The feasibility and acceptability of falls prevention telerehabilitation needs further investigation.
OBJECTIVE:
The objective of this study was to explore the opinions of participants and physiotherapists about a falls prevention telerehabilitation programme, and identify key barriers and facilitators to improve the quality of future similar programmes.
METHODS:
A qualitative study design was used, 13 semi-structured one-to-one telephone interviews (n = 11 participants, n = 2 physiotherapists) were performed. Data were coded and thematic analysed.
RESULTS:
Four inter-related themes were identified: technical considerations for change in mode of programme delivery to online and blended; facilitators and barriers for effective delivery of the online and blended programmes; factors promoting programme engagement and progress; significance of supportive interpersonal relationships.
CONCLUSIONS:
Participants and physiotherapists reported improvements in strength, balance and confidence, and willingness to continue the exercises long-term. Telerehabilitation had some advantages over in-person including flexibility and convenience; however, these gains must be considered against the drawbacks of less social interaction and group cohesion. Key insights identified regarding satisfaction with the technology, format and delivery can be used to improve the quality of future online and blended programmes.
Introduction
Falls can have detrimental physical and psychosocial effects on older adults, causing serious injuries and even death [1]. A third of community-dwelling adults aged 65 years and over fall each year, with a high incidence of fall-related injury affecting this population [2]. The resulting hospital stay, injury treatments and follow-up care create a significant healthcare cost [1], estimated to reach 2000 million euro per annum in Ireland by 2030 [3]. There is increasing evidence indicating exercise-based programmes can dramatically reduce the incidence of falls [4–6]. Evidence-based programmes such as OTAGO [2] have been shown to effectively reduce the rate of falls in the community [1, 7]. These strength and balance programmes reduce the risk of fall-related injuries by 32–40%, including severe falls requiring medical care or hospitalisation [8].
Although physiotherapy-led OTAGO falls prevention programmes are being run in community healthcare settings in Ireland [9], the Covid-19 pandemic altered the way in which these could be delivered, as group exercise classes were cancelled due to public health measures in place at the time. These measures exacerbated falls risk as isolation and ‘cocooning’ strategies resulted in sedentary behaviour and associated activity restriction [10]. The consequent physical deconditioning resulted in strength and balance deficits and a fear of falling which can lead to a cycle of further activity restriction and increased likelihood of falls [11]. Integration and innovation were required for new modes of service delivery to provide a service that met the needs of older adults at risk of falling in the context of limited resources of healthcare workers.
The Covid-19 pandemic necessitated fundamental changes in the delivery of health services, with a resultant substantial increase in the uptake of telehealth [12]. Delivering a falls prevention programme online via telerehabilitation offers a solution to the issue of reaching a larger population with limited healthcare personnel but, as it is a novel way of delivering interventions, with differences in implementation to a physical setting, research is needed on how it is perceived by physiotherapists and participants [13]. These perspectives can provide information about levels of confidence in, and satisfaction with, the technology, format, and delivery of the intervention [14]. They can also inform future iterations and improve the quality of provision by adapting rehabilitation techniques and refining approaches to better meet participant needs [15]. Given the paucity of qualitative studies evaluating participant and physiotherapist experiences, there is a need for research on the feasibility, safety, and efficacy of telerehabilitation in falls prevention, as well as usability of the technology and accessibility of newer modes of delivery [14].
This paper aimed to gather the opinions of participants and physiotherapists on their experience of a blended online and in-person delivery of a falls prevention intervention to inform subsequent iterations of the programme. Physiotherapist perceptions of their experience will provide information about intervention fidelity, set-up, referral process, and delivery, as well as barriers and facilitators to implementation.
Methods
This study was part of a larger study evaluating the feasibility and effect of an OTAGO falls prevention programme in the west of Ireland. Eligible participants were screened and assessed in their homes at baseline, followed by an 8-week programme of one physiotherapist supervised session and two unsupervised home-based sessions per week. Initially, the programme was an online only intervention but became blended, with participants experiencing online classes at first then in-person classes in accordance with the Covid-19 government guidelines. Participants were also supplied with a ‘Staying Steady’ exercise booklet which contained all the OTAGO exercises, one per page, and information on bone health, eyecare and hearing, knowing your medications, foot care, home hazards and what to do if you have a fall. They also received a ‘Get Up and Go’ information booklet with information on falls prevention. Issues were also discussed in the class such as pendant alarms and how to apply for them, suitable classes running in the community and where to access information on classes. Following this, participants were interviewed for this study, which focused on a qualitative evaluation of the participant and physiotherapist experiences.
Study design
A qualitative study design was utilised, with semi-structured one-on-one interviews used for data collection. Data were coded and thematic analysis was used to form themes [16]. Ethics approval was obtained from the University Hospital Ethics Committee in Ireland on the 16th of January 2021.
Participants
Participants in this study were recruited from the primary study to provide exit interviews for qualitative analysis. Primary study participants were community-dwelling, independently mobile adults aged over 63 years who reported a history of falls, fear of falling or difficulty with balance. Recruitment for the primary study occurred through healthcare provider referral from local hospitals and primary care centres or self-referral to the study team following a health promotion campaign on local radio. All individuals who completed the eight-week programme between the 23rd March 2021 and 3rd July 2021 were invited to participate in the qualitative analysis, with all those who consented to taking part selected for this study. The physiotherapists involved in the delivery of the falls prevention programme were also recruited to participate.
Data collection
Before entering the study, participants and physiotherapists provided written consent to be involved in the intervention and be contacted to take part in exit interviews via telephone. The falls programme ran in consecutive eight-week blocks from March to July 2021. In line with Covid-19 Government guidelines at the time, participants took part in either an online only programme (n = 5) or blended programme where individuals completed first online and then in-person sessions (n = 6). Participants who could attend in person and were geographically and physically able to access the venue were more likely to choose the blended programme.
One-on-one semi-structured interviews were conducted by two final year MSc in Physiotherapy students. Participants were interviewed in the week after they completed their individual eight-week programme to ensure accurate recall and reflections of their experience. Two physiotherapists involved in leading the intervention were interviewed for their perspectives as stakeholders in September 2021.
The 13 interviews (n = 11 participants, n = 2 physiotherapists) were audio-recorded and transcribed verbatim. Interviews were an average of 17.23 minutes (range 8.38–39.34 minutes). The questions used for the interviews were formulated and pre-approved by the research supervisor and the interviewers. This semi-structured approach was chosen as it enabled the interviewee an opportunity to explore meaningful issues which allows diverse perceptions to be expressed. It also enabled reciprocity between the interviewer and participant, giving space for follow up questions based on the interviewee’s response [17].
Data analysis
Data were analysed using Braun and Clarke’s 6-step approach of familiarisation, coding, generating initial themes, reviewing themes, naming and defining themes, and writing the report [16]. Initially, two randomly selected transcripts (one from each interviewer) were independently coded by the two physiotherapy MSc students and their research supervisor. Codes were discussed, clarified and agreed upon in a peer debrief meeting which provided rigour to the process. A coding framework was established to capture the opinions of the participants and physiotherapists. The remaining transcripts were then independently coded and agreed upon by the two students. NVIVO 12 software was used to organise and manage data. Data were anonymised, encrypted, analysed, and reported according to COREQ reporting guidelines [18].
The coded data were collated into an initial thematic mind map (Fig. 1) and themes were identified by analysing patterns of shared meaning. These patterns resulted in overarching concepts which were refined into four final themes.
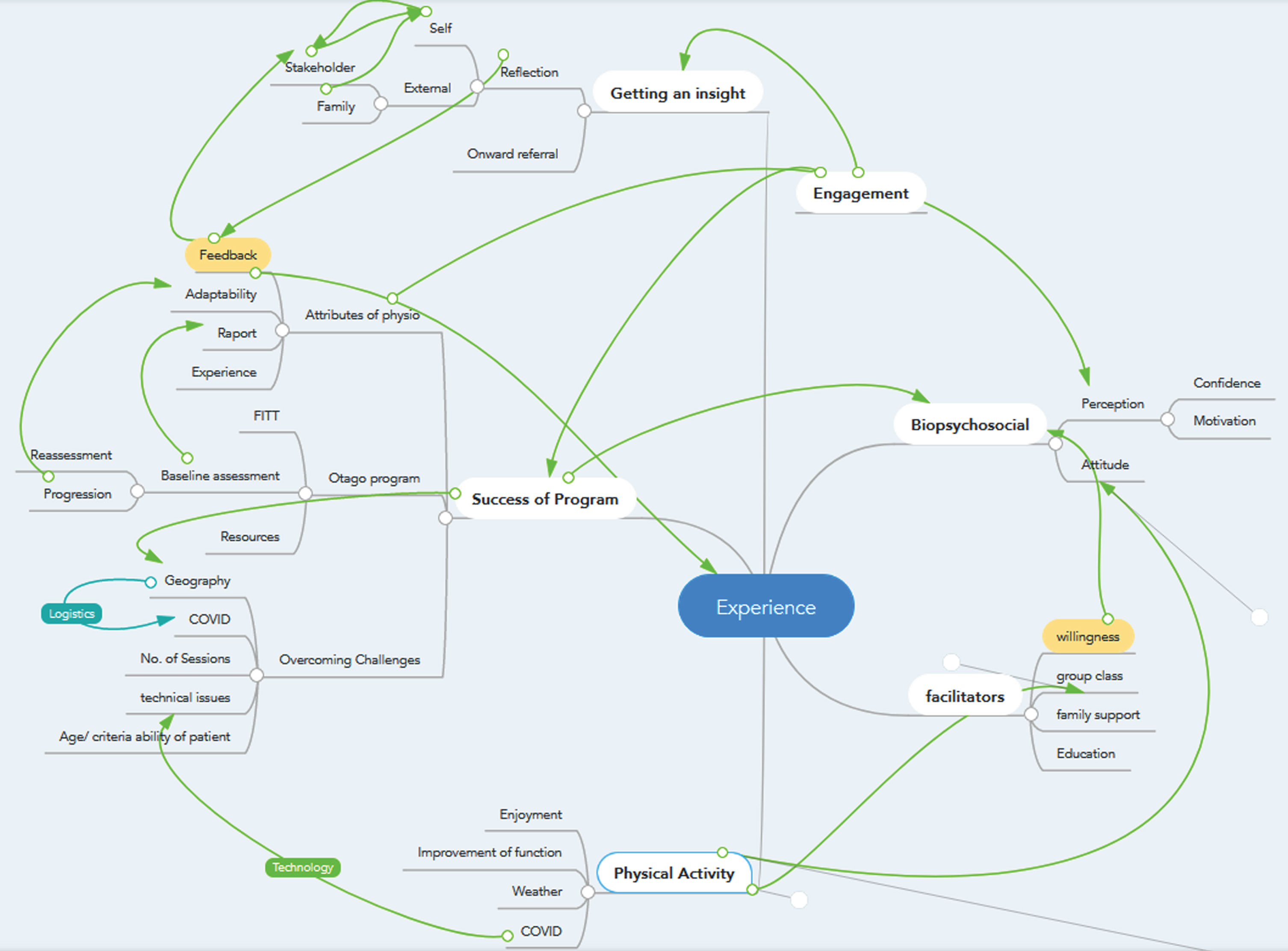
Initial thematic mind map.
Eleven female participants aged 63–88 years (mean of 75.94 years) were interviewed. One of the study physiotherapists was more experienced in delivering falls prevention programmes than the other, but both were new to delivering group interventions via telerehabilitation.
An overarching concept generated from the interview data was the positive perception of the programme experience, shared by the participants and the physiotherapists in both the online and blended forms of delivery. Another key concept was the personal preferences for mode of delivery identified by both the participants and physiotherapists. Thematic analysis of these concepts resulted in the identification of four inter-related themes. Figure 2 represents a link between the themes and how the supportive interpersonal relationships were significant throughout, linking each of the individual themes and contributing to the overall positive perceptions of the intervention and informing the preferences for mode of delivery.
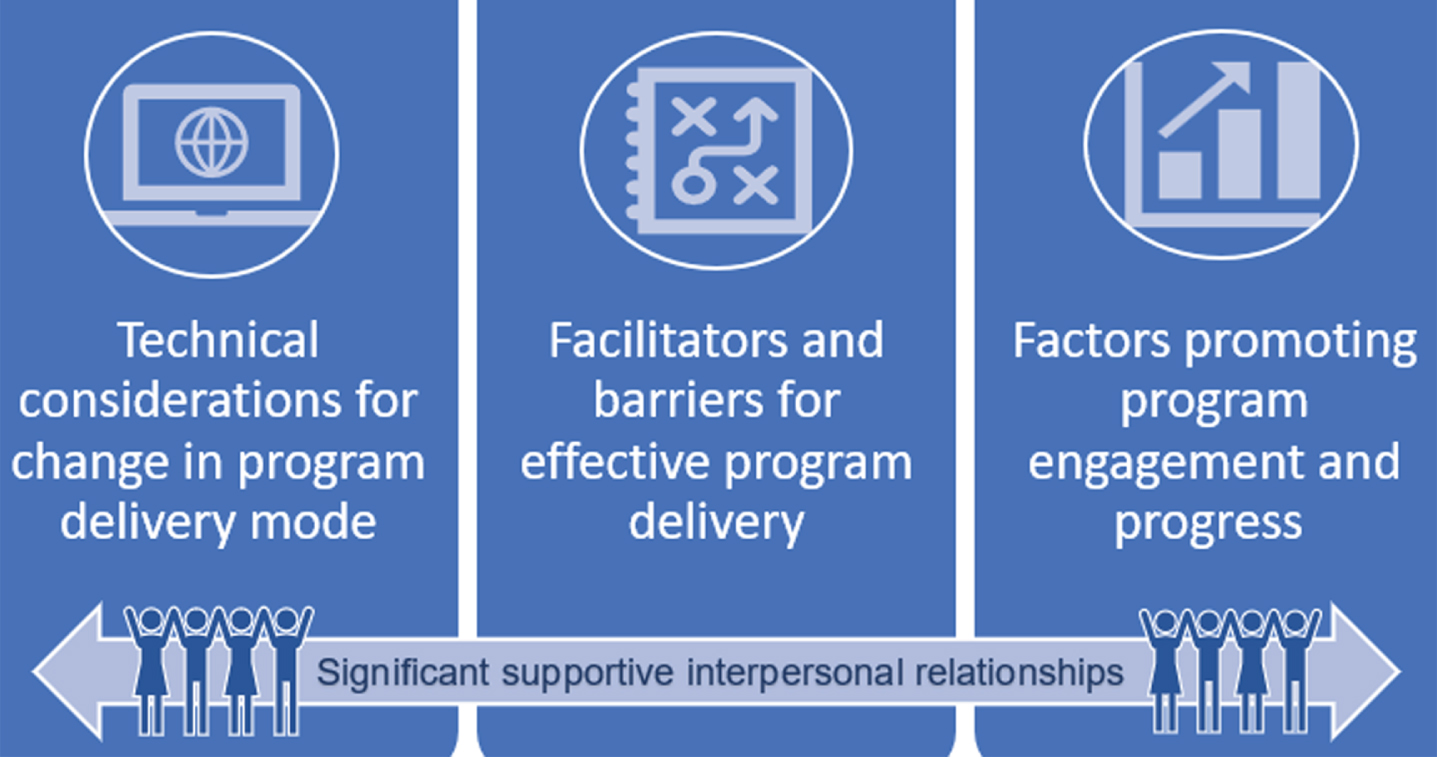
Finalised themes.
This theme describes the variety of technical and logistical considerations necessary to alter the mode of delivery of the programme from in-person to online and blended. Both physiotherapists and participants discussed the increased resource requirement in people and equipment to run the programme safely and effectively. Considerations mentioned by the physiotherapists included limiting the class size to five participants and requiring a big screen to monitor everyone’s safety as the exercises challenge balance and pose a falls risk. They reported finding the online supervision more ‘intense to keep an eye on everybody’ (physiotherapist 1) compared to in-person, although the big screen was seen as an advantage over using a laptop. However, this was also described as a limiting factor in terms of coordination and flexibility of class time and location as they only had access to a big screen television in one location. Physiotherapist 1 explained ‘so we managed to do that, but now there’s competing for it, so now we can only have it from 12 o’clock’.
Physiotherapists also felt it was important to do a pre-programme home visit to take baseline measurements and show participants how to set up the technology to ensure that the screen was positioned for optimal visibility... ‘so that we can see them doing the walking and then all of the footwork’(physiotherapist 1). Physiotherapists also found this visit helped to establish a positive therapist/client relationship... ‘I think it helps to develop the rapport’ (physiotherapist 1). Participants also shared this view with most expressing appreciation for the initial visit and technical support... ‘I thought that was very thorough’ (participant 11 online).
As technology use was a requirement for the online classes, participants discussed their ability to access technology either independently or with family support. Most participants interviewed cited lack of technical skills as the reason for needing assistance. One participant summarised the varying technical abilities of this age group:
‘The only thing with us older people, is we can’t set up these tablets and things... So that made it a bit awkward...but a lot of older people can do that stuff.’ (participant 2 online)
This opinion was also shared by the physiotherapists who had initial concerns about older people’s ability to use technology. However, they found that... ‘older people can manage the technology. Some of them are whizzes’ (physiotherapist 1).
Theme 2: Facilitators and barriers for effective delivery of online and blended programmes
This theme focuses on the range of factors enhancing and limiting online and blended programme participation and, thus, perceived quality of the experience and preference for mode of delivery.
Firstly, although participants’ responses showed a positive attitude to their online experience overall, some barriers in using the technology were mentioned which negatively affected their ability to engage as fully in the online class as they would be able to in person. These included physical restrictions such as poor eyesight and limited mobility resulting in difficulty seeing the small screen at a distance. This led one participant to express a preference for ‘the group meeting because I feel I’m more in control then’ (participant 4 blended); and another participant describing how she needed her daughter to position the tablet on the floor as she couldn’t bend down due to a hip dislocation... ‘I’m just afraid to bend down.... so in one sense I was glad that the class went back to (in person),’ (participant 5 blended).
Other reported barriers with the online delivery included connection issues such as poor broadband service... “Sometimes the picture... would go blank on us,’ (participant 2 online). Some participants felt they lacked the technical skills to solve these issues and couldn’t continue the class unless they had someone in the house who could assist them:
‘My husband had to stay in the other room, and I’d call him if I needed him. And if you had nobody in the house and it went blank it was gone... whereas if (the therapist) was in the place with a person it might be different.’ (participant 2 online)
Despite these challenges with technology impacting the class delivery and leading some participants to express a preference for in-person delivery, the convenience and accessibility of doing the programme at home, as well as the close level of supervision online were perceived as facilitating a high-quality programme experience.
Accessibility and convenience were identified as key facilitators as participants enjoyed being able to do it at home as it’s ‘much easier’ (participant 1 online) and allows for easy carry-over of the exercises into at home practice... ‘I can continue with the exercises in my own kitchen,’(participant 1 online). Physiotherapists also felt that the removal of transport was a facilitator... “I think in some ways it’s easier for people,’ (physiotherapist 2).
Finally, the quality of supervision was viewed as facilitating a positive experience in both the online and blended delivery. Participants had mixed views about which mode was better with some feeling they received more individual attention online... ‘I think we did better this way, because I think they were able to watch us individual,’ (participant 8 online), whereas others thought the feedback and correction was better during the in-person class ... . ‘at least you knew you were doing it right. Because if you weren’t doing things exactly like you should be doing them the girls would tell you how to do them,’ (participant 6 blended).
Theme 3: Factors promoting engagement and progress
Programme engagement and progress was reportedly promoted by several factors including motivation, perceived value of physical activity benefits, and educational resources.
Participants’ own baseline and ongoing motivation was a key factor in maintaining engagement as well as the insight gained into the value of sustained exercise to maintain health and function. Physiotherapists indicated that self-motivation was an important part of the inclusion criteria in referral to the programme. .. ‘that they show an interest in doing it,’ (physiotherapist 1).
Most participants reported that prior to the programme they enjoyed being physically active. The majority felt that their baseline level of physical activity increased because of the programme as they saw improvements in their fitness... ‘you felt you were getting a bit more active, and it was helping you,’ (participant 4 blended).
Participants identified an increase in independence with daily tasks, improvements in functional strength and mobility, and increased balance confidence as perceived programme benefits, enhancing their engagement and progress:
‘Now I can hop up out of the chair and sit down quick whereas before I’d be a bit slow....... Well, you’d be more confident at doing stuff.’ (participant 2 online)
The benefits they felt they were gaining gave them increased ‘courage’ and ‘confidence’ to try new exercises and adhere to a more regular exercise routine... ‘when you’re here on your own, stood there watching telly I go to my kitchen and do some exercise where I wouldn’t dream of before,’ (participant 1 online).
Participants felt this increased insight into the importance of exercise was due to the quality of education in the programme as they were provided with an exercise booklet so they could practice twice a week in addition to the classes for the eight weeks and then continue to maintain an exercise routine of three times a week upon completion of the programme. The booklet was viewed very positively by participants... ‘Well, I have the booklet... and I try and do them as often as I can. It’s surprising what you can do when you’re working,’ (participant 5 blended).
Some participants indicated they shared what they learned with their peers in the community.
‘I must try and get one or two (friends) to join the classes... because she had two falls... I’m going to photocopy some of the exercises and maybe she could do them.’ (participant 2 online)
‘I saw him(husband) with my book up on the table and he is doing the exercises ... ..’ (participant 7 blended)
The physiotherapists also discussed onward referral and suggestions to other group-based activities such as ‘activator pole classes’ to ensure maintenance and progress of the benefits acquired from this intervention.
Theme 4: Significance of supportive interpersonal relationships
Having supportive relationships with the therapist and their peer networks of family and friends were identified as significant in the participant’s enjoyment and involvement in the programme. All participants described their interactions with the therapists as positive...’we had brilliant interaction with the physio,’ (participant 8 online). One participant spoke about her appreciation for ‘such interest in us older ones... and it was a great feeling to know that there’s somebody interested in improving your life,’ (participant 3 blended).
Key attributes of the therapists which the participants valued were their ‘helpful,’ ‘down to earth’ and ‘efficient’ attitudes and the excellent quality of instruction in explaining and demonstrating exercises and providing constructive feedback to improve... ‘I liked how she... explained everything and was talking to us and correcting us during the class. It helps you do better’ (participant 10 blended).
The positive view of the instructor feedback was shared by participants in the online only and blended modes of delivery.
‘I was very happy doing the exercises when a physio would come on and their voice would keep me motivated and repetitively assure that I was doing the exercises correctly and bringing me forward.’ (participant 9 online)
Physiotherapists also described the importance of providing encouragement and reassurance while making corrections...‘you have to tell them when they’re doing well,’(physiotherapist 2). This supportive relationship gave participants ‘great confidence’ and ‘motivation’ to continue the exercises after the programme finished as they felt empowered by the therapists ‘telling us that we’re doing it right, helping us along, …encouraging you to go on and to improve,’(participant 4 blended).
The empowering therapist-participant relationship resulted in a positive experience. The participants described the programme as ‘fun,’ ‘beneficial’ and ‘enjoyable’ and the therapists’ delivery of the programme as ‘excellent’... ‘I’d give her 99 out of 100 for everything she did or 100 out of 100,’ (participant 2 online).
Although many participants appreciated the quality of their interactions with the therapists, most mentioned a preference for in-person delivery for social interaction and group cohesion. Online-only participants mentioned missing the peer network...’It would be lovely to be in the room with all the women and the girls but that’s the way things are at the moment,’ (participant 2 online), and blended approach participants felt the in-person provided group cohesion...’It was actually nice to be with the group and have a chat afterwards and see how they were doing in comparison to myself,’ (participant 6 blended).
Due to Covid-19 social distancing measures, some participants in the blended delivery mentioned that peer interaction was limited during in-person sessions... ‘because it was Covid we weren’t interacting with each other, only the girls (therapists) would tell you if you weren’t doing it’, (participant 4 blended). Although the online mode of delivery and Covid-19 reportedly reduced the level of social interaction, participants did mention peer support contributing to their positive experience. Another key aspect of interpersonal relationships was the involvement of family members. Family support with transport helped some participants access the in-person classes. ‘I got a ride from my husband to the centre every time I had a class there so yes, they helped me a lot’ (participant 10 blended).
Discussion
Overall physiotherapists and participants had positive perceptions of their involvement in the online and blended formats, viewing it as enjoyable and beneficial. Technological challenges were overcome with support and positive interpersonal participant-therapist and participant-peer relationships. However, most participants thought these interactions were enhanced in the in-person group setting due to better social interaction and cohesion.
Whilst published literature on the live online delivery of OTAGO is limited, a systematic review on modified delivery of OTAGO including both virtual and DVD formats found similar results to our study, namely that it is positively perceived by participants and provided physical benefits including improvements in functional strength and balance [19]. An increase in balance confidence and independence with activities of daily living noted by some participants interviewed matched that of participants in a qualitative study by Agha et al. (2015) on virtual delivery of OTAGO via DVD to people living in an isolated rural area in Canada [20]. These study participants reported an improvement in their lower body strength and balance, and some mentioned a reduction in their fear of falling. However, in contrast to our findings where participants viewed the live online class mode as enjoyable, some participants in the study by Agha et al. (2015) felt the DVD exercises were ‘too slow and low energy’ to be continued long-term [20]. Thus, the delivery of live online classes could be considered for participant enjoyment and enabling appropriate pacing of exercises to match and progressively challenge the participants’ abilities. This is consistent with the findings of a qualitative synthesis of five studies undertaken by Farrance et al. (2016) which has shown that improvements in wellbeing and a ‘humanised’ programme are important factors in promoting older adults’ long-term adherence to community group exercise programmes [21].
In this study participants felt that progressive physical improvements and the consistent encouragement from the therapists were motivating factors to continually engage in the intervention and a reason to continue with the exercises long-term after they completed the eight weeks. The importance of intrinsic motivation, the development of self-awareness of their agency in exercise participation and a supportive patient-therapist relationship have also been identified as facilitators to sustaining an exercise routine in other studies of older people’s experiences of telerehabilitation [22]. Hence, future iterations of this programme should maintain the same focus on educating participants to empower and self-manage by continuing with regular exercise safely to achieve long-term benefits beyond the eight-week programme.
Other factors which promoted positive participant engagement with the online mode of delivery according to both physiotherapists and some participants were that it afforded greater accessibility and was more convenient for some people to do at home as there were no travel requirements. Studies of telerehabilitation interventions with populations in comparable rural locations have drawn similar conclusions that participants and physiotherapists appreciate the flexibility of delivery that telerehabilitation offers [20, 23]. However, this view was not shared by all study participants as many expressed a preference for getting out and socialising. This view is supported by the literature that found a preference for in-person delivery to optimise social interaction [19–21] and an opportunity to leave the house [23]. Farrance et al. (2016) reported that the feeling of ‘social connectedness’ was considered a facilitator to older people’s long-term group exercise adherence across all five studies included in their qualitative synthesis [21], a view echoed by most participants and physiotherapists interviewed as part of this study who felt there was better group cohesion when the group met together in-person. The psychosocial benefits of group exercise are widely established in the literature [19] so we recommend that the future delivery of this intervention be in a blended format with the online mode used as a complement to face-to-face programmes to reach a wider patient cohort, rather than as a replacement to in-person delivery. Although most participants expressed a preference for in-person delivery, when in-person classes resumed, peer interaction was limited due to social distancing requirements; hence participants stayed apart and did not mingle before or after the class. Other participants reported using family supports and peer networks as social support by sharing the exercise booklet with family and friends and using these peers as exercise buddies. The importance of this strategy has been identified by participants in previous literature as involving friends and family can be a way to promote the social connection that is lacking in a virtual format [20].
As well as involving family and friends for social connection, several participants felt they needed the physical presence of family members in the house to support them in every class with physically positioning the device or solving technical problems if the internet connection was lost. Although participants felt they were adequately supported by family members to overcome these challenges, the usability of the technology is an important factor to be considered by physiotherapists in planning future interventions [22, 23]. It determines the inclusion criteria of the participants as they must be able to use the technology or have someone present to assist them, the internet service must be adequate to allow uninterrupted participation in live online classes, and the therapists leading the intervention require extra resources such as a big screen television to safely monitor all participants. However, research undertaken by Gell et al. (2021) suggests that adequate supports, such as individualised technology orientation sessions and standby technical assistance, can facilitate older adults to successfully partake in telehealth programmes, even if they have little to no experience of accessing teleconferencing platforms [24]. Furthermore, despite the increased resource requirement, participants and physiotherapists reported positive feedback on the level of practical support implemented during their telerehabilitation experience which aligns with the current body of literature that telerehabilitation falls interventions can provide a feasible and cost-effective mode of delivery [25] with no adverse effects for participants according to published studies [26].
Strengths and limitations
A strength of this study was that with one exception, all participants contacted agreed to participate in the interviews which led to a robust data set for analysis. The interviews with participants were conducted in the week they finished the programme and this proximity to the intervention enabled them to give more accurate and detailed reflections on their experience [17]. The semi-structured interview approach was chosen as it is a validated method to explore participant and physiotherapist thoughts, feelings, and beliefs [27] and the utilisation of an interview guide, including a question route as well as possible probes and follow-up questions, prepared and discussed with an experienced qualitative researcher in advance of conducting the interviews, provides rigour to the findings and contributes to the trustworthiness of this study [17]. The study was limited to a geographically small rural area in the west of Ireland which may not be representative of older Irish people living in more urban areas. Other potential limitations were that the interviews were conducted via telephone by novice interviewers rather than in-person. According to research by Drabble et al. (2016), telephone interviews present more challenges in building rapport and being unable to respond to visual cues, but other studies argue it affords participants more privacy and reduces distractions [28]. In this study, we found it provided interviewees more flexibility in terms of time and location of interview.
Implications for future research and practice
Participants’ and physiotherapists’ positive perceptions of the online and blended interventions show falls prevention programmes delivered via telerehabilitation are feasible and enjoyable, but more research is needed into their efficacy. This presents future opportunities for this study to be conducted as a pilot feasibility study and then larger scale randomised controlled trial, with potential for qualitative interviews to be conducted with participants from a wider geographical area, thereby enhancing the applicability of the findings to clinical practice by providing a broader range of participant and physiotherapist views. This would help to improve future designs of this intervention, leading to improvements in the accessibility, convenience, and quality of falls prevention service delivery in Irish healthcare.
Conclusion
This study has shown that participants and physiotherapists viewed their experiences of a community-based falls prevention telerehabilitation intervention undertaken during COVID-19 as positive and effective, resulting in perceived improvements in strength and balance, increased balance confidence, and an expressed willingness to continue the exercises long-term. This study informs the implementation of future iterations of this programme by showing that older people are able and willing to use the technology required for telerehabilitation, however, participant and physiotherapist feedback suggests it would be better utilised as an addition to in-person classes to reach a wider cohort of people, rather than a replacement of in-person as most older people prefer the psychosocial benefits gained from face-to-face group exercise.
Conflict of interest
The authors have no conflict of interest to report.