
Abstract
Background:
Each year, 1 in 4 people over the age of 65 years of age will experience a fall. It is important to identify and address modifiable risk factors that are associated with falls in adults at high and low risk for falls.
Hypothesis:
Falls risk improves in both high-risk and low-risk participants with the implementation of Stay Active and Independent for Life (SAIL).
Study Design:
Cohort study
Level of Evidence:
Level 3.
Methods:
Seventy-eight older adults (age, 70.9 ± 5.1 years) were included in this study and categorized into high risk and low risk for falling based on the falls risk score from the Physiological Profile Assessment. High risk was defined as having a preintervention falls risk score >1, whereas low risk was defined as having a preintervention falls risk score <1. Both groups had the same 10-week intervention. A multivariate analysis of covariance was used to compare differences pre- and postintervention, using preintervention falls risk score as covariate.
Results:
Results showed that regardless of preintervention falls risk, participants showed significant improvements in right and left knee extensor strength and sit-to-stand after participation in the 10-week SAIL program. Also, noteworthy is that 15 participants who were considered at high risk for falling preintervention were considered low risk for falling postintervention.
Conclusion:
The positive outcomes noted on modifiable risk factors suggest SAIL can be beneficial for decreasing falls risk in older adults, regardless of risk of falling, using a multifactorial exercise intervention. Our results also showed that it was possible for participants not only to improve falls risk but to improve to such a degree that they change from high risk to low risk of falling.
Clinical Relevance:
Our results demonstrated that SAIL was effective in improving overall fall risk after a 10-week intervention. Targeted community-based interventions for the aging population can bring physical health benefits that can decrease falls risk.
Each year, 1 in 4 people over the age of 65 years of age will experience a fall. 2 Further, of those who suffer a fall, approximately 3 million will seek emergency treatment each year for fall-related injuries, with more than 800,000 of these people being hospitalized, many with head or hip injuries.5,35 The health consequences of falls are reinforced by the fact that, from 2007 to 2016, death rates from falls increased 30%. 4 This increase in falls-related injuries has led to healthcare costs estimated to be in excess of $50 billion in the United States in 2015. 8 Given these significant numbers, it is important to identify and address modifiable risk factors that are associated with falls. 6
Risk factors for falls are commonly defined as either extrinsic (ie, within the environment) or those that can affect the functioning of the body itself (ie, intrinsic). 18 Intrinsic risk factors include muscle weakness, cognitive impairment, loss of coordination, gait and posture problems, poor vision, postural hypotension, polypharmacy, and fear of falling.37,38 It is notable that older adults with a history of falling are at 2 to 3 times higher risk of experiencing a subsequent fall. 37 Although various risk factors have been identified, the most modifiable for older adults are muscular weakness, balance control, and walking ability. 30 It is well established that different forms of exercise can lead to improvements in falls risk.24,33 Exercise interventions that have been shown to increase strength and improve reaction times can be instrumental in mitigating falls risk.11,32 Despite evidence demonstrating that exercise can lead to improvements in strength, balance, and walking ability, an ongoing issue is simply getting older persons to engage in regular physical activity. One solution has been to design and implement accessible community-based physical activity programs. 14 However, issues with which programs translate better into community settings for reducing falls risk still need to be resolved. Given that older adults with a previous history of falling have a heightened risk of suffering another fall in the future, there is also a compelling reason to investigate how exercise interventions can benefit both groups.
Stay Active and Independent for Life (SAIL) 40 is a community-based intervention designed specifically to target several risk factors which contribute to falls. SAIL focuses on improving strength, balance, aerobic fitness, and flexibility through group exercise sessions led by an instructor, and can easily be implemented within a community setting. The evidence obtained thus far shows that SAIL improves strength and balance in older adults in the community setting and improves their ability successfully to complete activities of daily living, 40 but further research is needed, particularly in assessing the program’s effectiveness for older adults classified as being at high risk for falling or low risk for falling, as most fall prevention programs focus on those who have already experienced a fall 36 and are at an increased risk of experiencing another fall. Older adults may not experience a fall and still be at a high risk of falling, whereas those who are at a low risk for falling can continue to improve their falls risk.
The purpose of this study was to compare the effects of a 10-week SAIL intervention between community-dwelling older adults classified as low risk for falling and high risk for falling. The impact of this intervention was assessed using a measure of overall falls risk, which was determined from the Physiological Profile Assessment (PPA). This validated assessment includes measures of knee extension strength, lower limb proprioception, reaction time, balance, and vision (edge contrast sensitivity), and has been used previously to determine fall risk in community-dwelling older adults.15,17,20 In addition, sit-to-stand (STS) and timed up and go (TUG) tests were also used to gauge improvements. We hypothesized that falls risk would improve in both high-risk and low-risk participants with the implementation of SAIL.
Methods
Participants
Seventy-eight participants volunteered to participate in this study and gave informed consent that was approved by the University Institutional Review Board. Participants included community-dwelling people, 55 years of age or older, who were recruited from the community. High risk was defined as having a baseline falls risk score (determined from the PPA) >1, whereas low risk was defined as having a baseline falls risk score <1. 39 Twenty-eight participants were classified as high-risk preintervention (age, 72.03 ± 5.12 years; height, 1.62 ± 0.06 m; weight, 78.47 ± 14.13 kg) and 50 matched participants were classified as low-risk preintervention (age, 69.80 ± 5.12 years; height, 1.66 ± 0.09 m; weight, 80.30 ± 18.31 kg). Participants were matched based on age, sex, and falls risk at preintervention. Participants were excluded if they were not mentally capable of participation in the assessments or had health issues that influenced the performance of the assessments (ie, Parkinson’s disease, multiple sclerosis).
Assessments
Assessments of each participant’s falls risk using the PPA were conducted pre- and postintervention. 16 The TUG and STS tests were also included. Each assessment is described in the following.
Physiological Profile Assessment
The PPA assesses falls risk by measuring those physiological measures most frequently associated with falling. The PPA includes assessments of cognition [ie, simple hand reaction time hand (HRT) and foot reaction time (FRT)], lower limb strength [assessed knee extension for both the right leg strength (RLS) and left leg strength (LLS)], lower limb proprioception, balance, and vision (ie, edge contrast sensitivity). 16 Except for the balance tests, all assessments were performed while seated. The PPA generates an overall falls risk score based on data from individual physiological assessments. The overall score ranges from -2 to +4, with higher values indicating an increased risk of falling. 16
Reaction Time
For HRT, a modified computer mouse was used as the timing device. For FRT, a foot pedal was utilized. A light stimulus signaled the beginning of the trials. On presentation of the light, participants were asked to press or tap as quickly as possible. Each participant completed 20 trials for the hand and 20 trials for the foot. The first 5 trials were counted as practice trials, and the average of the middle 10 HRT and FRT trials were used for the PPA. The last 5 trials were removed to offset any potential fatigue effects.
Knee Extension Strength
Each participant was asked to complete a series of maximal isometric knee extension contractions for each leg while seated. For this task, the knee of each person was positioned at 90° with an adjustable strap placed above the malleoli of the ankle. The strap was attached to a strain gauge attached to a crossbar situated between the back legs of the chair. This was repeated for both legs. Each participant completed 3 trials. Peak force was attained (in kg) and normalized to body mass.
Proprioception
An acrylic sheet, with a protractor embedded in it, was placed between each participant’s legs while in a seated position. Participants were instructed to close their eyes, extend both legs out in front of them and match their big toes together. Five trials at varying heights were completed with differences (in degrees) in the big toe placement between both feet being recorded for each trial.
Anteroposterior and Mediolateral Sway
Each participant stood on top of a 15-cm-thick foam pad with a sway meter attached at waist height. Participants were instructed to stand as still as possible with eyes open for 30 s, while the pen that was attached to the sway meter recorded each participants’ postural motion. Maximum amount of sway, for one trial, in both the anteroposterior and mediolateral directions were recorded.
Edge Contrast Sensitivity
The Melbourne Edge Test was used to assess edge contrast sensitivity. With this test, participants were seated 50 to 60 cm away from an angled desk that held a chart with 20 circular 25 mm diameter patches containing edges of reducing contrast. Each participant was asked to identify the orientation of the edges. The last circle with the lowest contrast that was correctly identified was recorded in decibel units (dB = -10log10 contrast). Higher scores represent improved performance on this test.
Timed Up and Go
This test was used to assess a participant’s mobility and identify older adults at greater risk for falls.26,31 To complete the test, each participant stood up from a chair, walked a 3-m loop around a cone, and returned to a seated position in the chair. Three trials were completed. The time (in seconds) taken to complete each trial was recorded.
Sit-to-Stand
To complete the STS test, a participant sat in the middle of a chair with feet flat on the floor. The participant placed hands on opposite shoulders with arms crossed at the wrists and, keeping their back straight and arms against their chest, they rose to a full standing position, then sat back down again. The number of times the participants came to a full standing position in 30 s was recorded.
Intervention
A multifactorial exercise intervention (SAIL) was implemented 3 times a week for 10 weeks. The intervention took place in the community including senior centers, assisted living centers, places of worship, and/or community fitness facilities. Participants were guided through a series of exercises from the SAIL program by trained instructors who had completed the SAIL instructor training. 40 Necessary equipment, such as armless chairs and ankle weights, was provided. Modifications were also provided for each exercise to ensure all participants’ needs were met following SAIL guidelines.
Each session included strength, balance, and aerobic fitness components. Sessions lasted for 1 h and included a 3- to 5-min warm-up, an 18- to 20-min aerobic component, a 10-min balance and cool down, 15 to 18 min of strength exercises, and 8 to 10 min of stretching. The warm-up was composed of movements for both upper and lower body as well as full body movements. The balance component incorporated static and dynamic balance exercises, which included weight shifts, change in base of support, and vestibular activities. Upper body strength exercises included biceps curls, triceps extensions, lateral arm raise, frontal arm raise, overhead press, and seated crunches. Lower body strength exercises included hamstring curl, knee extension, hip flexion, hip extension, lateral leg raise, and calf raises. Three sets were completed, 1 set of 10 repetitions of each exercise for upper body, 1 set of 10 for lower body exercises, and 1 set of 10 of lower or upper body exercises, alternating between upper and lower body each class. Stretches addressed upper and lower body muscle groups.
Data Analyses
Data analyses were conducted with R (R Core Team; Vienna, Austria). 28 Case-wise diagnostics were performed to assess data normalcy. Descriptive statistics were conducted for all dependent measures by time (ie, preintervention and postintervention). Assumption testing was completed and met before inferential statistical analyses. Descriptive statistics were conducted for all dependent measures by time (ie, preintervention and postintervention). A multivariate analysis of covariance (MANCOVA) was conducted to compare the effectiveness of the intervention across time while controlling for preintervention PPA score. Alpha level was set a priori at 0.05.
Results
Attrition and Attendance
Seventy-eight participants were included in this study. Attendance rates were 75% for both low-risk and high-risk groups. As outlined previously, at baseline, 28 participants were categorized as high risk and 50 participants were categorized as low risk. Postintervention, 13 participants were categorized as high risk and 65 participants were categorized as low risk, demonstrating a 53% change from high to low risk. The average falls risk score (PPA) for the 15 participants that changed group membership at baseline was 1.65 ± 0.72 and postintervention it was 0.48 ± 0.25.
Intervention Outcomes
Descriptive statistics for all dependent variables are listed in Table 1. Results of MANCOVA demonstrated a statistically significant effect of time (F6, 130 = 3.454, P < 0.01, Wilks’ Λ = 0.862). Univariate analysis revealed overall falls risk improved from preintervention to postintervention. In addition, right and left knee extension strength was greater in both limbs postintervention compared with preintervention (RLS: F1,76 = 4.788, P = 0.03; LLS: F1,76 = 6.011, P = 0.02) and STS scores postintervention were greater compared with preintervention (F1,73 = 14.3, P < 0.01). Although not significantly different between preintervention and postintervention (P > 0.05), we did observe improvements in TUG, HRT, FRT, edge contrast sensitivity, and proprioception.
Mean and SD for all dependent variables by group for main effect of time (pre- and postintervention time points)
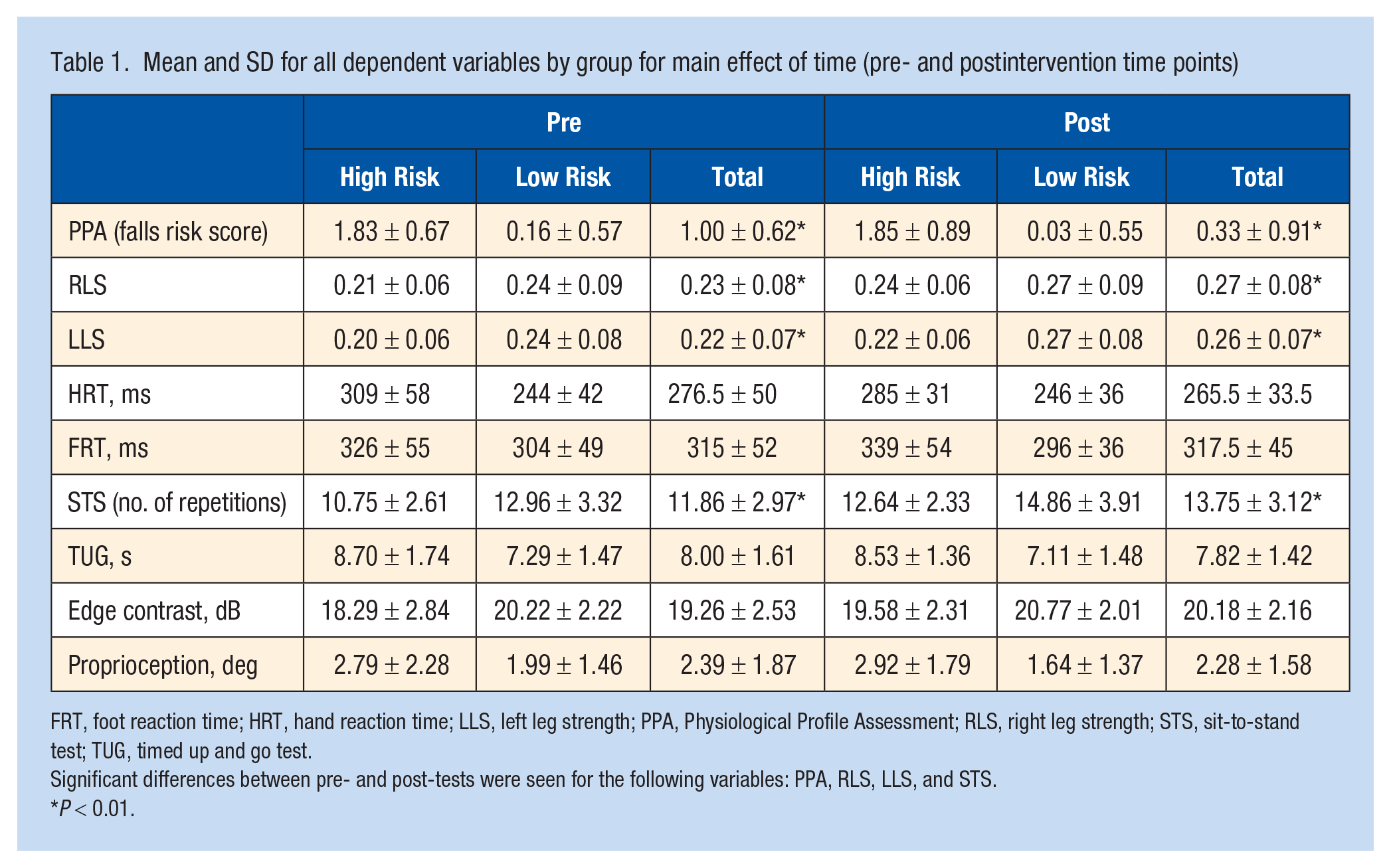
FRT, foot reaction time; HRT, hand reaction time; LLS, left leg strength; PPA, Physiological Profile Assessment; RLS, right leg strength; STS, sit-to-stand test; TUG, timed up and go test.
Significant differences between pre- and post-tests were seen for the following variables: PPA, RLS, LLS, and STS.
P < 0.01.
Discussion
This study was designed to determine the effects of the SAIL exercise intervention on falls risk in community-dwelling older adults. SAIL is an evidenced-based multifactorial exercise program designed specifically for the older adult population. 40 Several components of physical activity are addressed with SAIL, including aerobics, strength, balance, and flexibility. 40 Although previous research indicates that the SAIL exercise intervention leads to improvements in falls risk factors over time, 34 to the best of the authors’ knowledge, it has not been investigated whether improvements in a person’s falls risk depend on their initial preintervention falls risk.
After the implementation of SAIL, falls risk scores decreased significantly, indicating a reduction in overall falls risk. These findings are consistent with previous research that found improvements in PPA scores after the implementation of exercise programs.19,23,24,27 In addition, our results demonstrated that even for participants who are initially at a low risk for falling, their risk of falling can be further reduced using the same type of exercise as the high-risk group. The ability to improve falls risk in both high risk and low risk for falling groups, using the same exercise program, allows for a larger proportion of the older adult population to be targeted in an efficient manner. Furthermore, the results from this study may be used to increase confidence and promote exercise adherence for older adults who are considered at low risk for falling and do not feel the need to engage in exercise to delay age-related declines in function, or those who believe that an increased risk of falling is a normal part of aging and cannot be avoided.
The improvement in the falls risk score was primarily linked to significant increases in knee extension leg strength. Optimal lower body strength, particularly knee extension strength, is important for recovery after tripping, 25 which 60% of falls can be attributed to.1,29 Although not statistically significant, we also saw improvements in HRT, FRT, edge contrast sensitivity, and proprioception. Proprioception is crucial to the maintenance of balance because it provides sensory information about the position of a person’s body or limbs in space. 7 Faster reaction time allows for older adults to react more quickly to obstacles and recover or completely avoid a fall altogether. 13 In addition, after the 10-week intervention, we saw significant improvements in STS. The ability to stand up out of a chair without assistance represents an important measure of independence, 21 and can further contribute to inactivity and muscle weakness if unable to complete repeatedly. 22 TUG scores also improved; however, the improvements were not statistically significant. Furthermore, we had 15 participants from initially being classified as high-risk progress to low risk of falling after participation in the 10-week SAIL program. Not only was the SAIL program successful in improving the falls risk score but improvements were also large enough that 15 participants changed group membership. Given that falls can result in serious injury, participants who are considered at low risk for falling have a better chance of maintaining their independence and quality of life.
The results of this study are consistent with previous studies which have demonstrated that exercise interventions are a critical component of reducing a person’s falls risk. Indeed, it has previously been reported that exercise interventions utilizing not only multifactorial interventions 9 but also dance,12,27 Tai Chi, 10 and resistance training 3 can all be beneficial for mitigating falls risk. Although results varied by the specific program being assessed, the common denominator was that most exercise interventions resulted in decreased risk of falling and improved general balance ability. As a larger part of this project, we delivered community workshops to educate older adults about the benefits of physical activity to decrease falls risk. We believe that informed participants may be more likely to persevere with exercise programs, such as SAIL, and that educating community-dwelling older adults about the potential benefits of such interventions can lead to the adoption of programs for at-risk populations who are currently inactive.
There are limitations with this study that should be addressed. A convenience sample was used for a quasi-experimental study, which limits the generalizability of the effect of these interventions. Participants were recruited from the surrounding area and therefore were generally living close by to where the SAIL program was being offered. In addition, no follow-up took place after the intervention was complete. Although overall falls risk was improved, we do not know how long these benefits lasted and if any participants experienced a fall after the intervention. The benefits may have been temporary. Improving falls risk also means incorporating an active lifestyle and we do not know whether our participants continued to engage in physical activity after the conclusion of the intervention.
Conclusion
Overall, the positive outcomes noted on modifiable risk factors suggest SAIL can be beneficial for decreasing falls risk in older adults regardless of their initial falls risk status. In addition, as SAIL is designed for aging adults, the aging adult population may be more inclined to participate because they enjoy the class. For our study, we saw a 75% attendance rate for both high-risk and low-risk groups. Limiting falls risk is imperative for older adults successfully to complete activities of daily living and maintain independence. Implementing a multifactorial exercise program, such as SAIL, can help to mitigate that risk and assist the aging adult population in maintaining independence.