
Abstract
BACKGROUND:
Practice guidelines (CPGs) provide informed treatment recommendations from systematic reviews and assessment of the benefits and harms that are intended to optimize patient care. Review of CPGs addressing rehabilitation for people with moderate/severe traumatic brain injury (TBI), has not been fully investigated.
OBJECTIVE:
Identify published, vetted, clinical practice guidelines that address rehabilitation for people with moderate/severe TBI.
METHODS:
Six data bases were accessed using key word search terms: “Traumatic Brain Injury” and “Clinical Practice Guidelines” and “Rehabilitation”. Further inclusions included “adult” and “moderate or severe”. Exclusions included: “mild” and “concussive injury”. Three reviewers read abstracts and manuscripts for final inclusion. The AGREE II template was applied for additional appraisal.
RESULTS:
There were 767 articles retrieved using the search terms, 520 were eliminated because of content irrelevance; and 157 did not specify rehabilitation treatment or did not follow a process for CPGs. A total of 17 CPGs met all criteria and only 4 of these met all AGREE II criteria.
CONCLUSION:
There are few CPGs addressing rehabilitation for people with moderate/severe TBI. More interventional trials are needed to determine treatment effectiveness. Timely and methodologically sound vetting of studies are needed to ensure CPG reliability and facilitate access to quality, effective treatment for people with moderate/severe TBI.
Introduction
In 2011, the National Academy of Medicine, formerly the Institute of Medicine, proposed a definition for Clinical Practice Guidelines (CPGs) (Institute of Medicine (US) Committee on Standards for Developing Trustworthy Clinical Practice Guidelines, 2011). CPGs are statements that provide recommendations which are informed by a systematic review of evidence about diagnosis or treatment and include an assessment of the benefits and harms of alternative care options that are intended to optimize patient care (Institute of Medicine (US) Committee on Standards for Developing Trustworthy Clinical Practice Guidelines, 2011). They are developed to assist practitioners in making decisions about appropriate health care for a specific clinical condition.
Members of the committee that developed the report went further to identify additional recommendations so that there would be an assurance that CPGs would be trustworthy. The committee listed 6 points for people developing these guidelines to consider. These include: CPGs should be based on a systematic review of the existing evidence; be developed by a knowledgeable, multidisciplinary panel of experts; consider important patient subgroups and patient preferences; be based on an explicit and transparent process; provide a clear explanation of alternative care options and health outcomes, using quality of evidence and the strength of the recommendations; and be revised when new evidence warrants modifications of recommendations (Institute of Medicine (US) Committee on Standards for Developing Trustworthy Clinical Practice Guidelines, 2011).The recommendations for CPG development have been generally accepted and helped raise the standard for what is appropriate and reimbursable care.
CPGs help establish what is meant by quality medical care, reduce practice variation and ensure uniform utilization of treatments in order to establish standards of care and create performance measures that can be applied to patients with similar medical diagnoses/problems. Additionally, CPGs have educational value for practitioners, patients and care givers/family; and may help non-specialists extend quality practice in under-sourced specialties. CPGs are an important resource to health care consumers and providers. Significant obstacles to CPG adoption include access to resources and feasibility of implementation in low income areas (Patel et al., 2016).
Much has been written about the value of CPGs in improving quality health care. The importance of assuring the process by which they are developed, assuring the quality of the studies included in forming a decision about what to recommend for practice and the ease of access to CPGs are all important components of providing quality, timely and reliable care (Guyatt, 2006, 2011; Laine, 2011). In specialties such as rehabilitation, studies are infrequently randomized controlled trials. Clinical cohorts are often small and treatments while standard treatments, are highly individualized. This presents challenges for practitioners trying to determine best practices and level of evidence to support treatment planning. Despite these difficulties, when CPGs are properly performed, they help overcome some of these limitations (Kredo et al., 2016).
With respect to specifics about treating people post traumatic brain injury (TBI), there are significant benefits of having CPGs. For complex medical and biopsychosocial conditions, CPGs have the potential of bringing together recommendations for treatment from several disciplines to address this patient population’s multi-domain problems. For example, TBI is a chronic illness whose impact affects mood, behavior, physical and intellectual function (Corrigan & Hammond, 2013; Hammond, 2019, 2021). A wide variety of symptoms frequently follows from this injury; insomnia, depression and fatigue, to mention a few. Additionally, medical comorbidities may delay start of recovery, or/and degree of recovery (Malec et al., 2019). These include: hypertension, type 2 diabetes, rheumatoid arthritis, cancer, movement disorders, among others. CPGs can also provide a reliable review of literature, assessment of the level of evidence and best practices. Best practices do not meet the level of rigorous review required for CPGs, which depend upon a thorough and systematic review of published data from a variety of sources. CPGs report the different levels of evidence in their recommendations, assure the quality of the review process, rate and assess usefulness and practice experience. The absence of CPGs also may be the result of gaps in our current level of knowledge about treatment, a problem previously reported in a review of the literature about clinical rehabilitation research for people with TBI where it was reported that not much of the literature includes general rehabilitation and trials (Gerber et al., 2019).
Therefore, the motivation for this review is to determine which TBI-CPGs have been published that meet the criteria for inclusion for this review including: 1. clinical practice guidelines published between 2010–2020; 2. a stated process for providing reliable and trustworthy CPGs; and 3. that CPGs addressed rehabilitation and functional needs of people with TBI.
Methods
The following databases were searched for articles: PubMed, Cochrane Data Base, Ovid Medline, EMBASE, CINHAL and Web of Science. Selection criteria for the literature search included: “Traumatic Brain Injury AND Clinical Practice Guidelines AND Rehabilitation.” Further inclusions included “Adult”. Exclusionary terms included mild TBI or concussive injury. Additionally, a review from a general Google search that used the keywords mentioned, was performed to learn if there were CPGs from other sources that are not identified through the databases listed above that met inclusion criteria and had no exclusions. This included searching websites from well-known organizations, foundations and professional societies addressing practice guidelines for TBI. An additional inclusion criterion, determined after articles were read in full, was to determine that development of guidelines followed an established, accepted vetting process such as that by Oxford, or United States Preventive Services Task Force or Institute of Medicine (Institute of Medicine (US) Committee on Standards for Developing Trustworthy Clinical Practice Guidelines, 2011; Oxford Centre for Evidence-based Medicine, 2019; U.S. Preventive Services Task Force, 2018). The key elements for these vetting processes include some or all of the following: establishing transparency, managing conflicts of interest, developing guidelines for group composition, establishing a process for systematic literature review, establishing foundations of evidence for and strength of recommendations, articulating recommendations, establishing a process and committee for external review, and updating recommendations. Additionally, all articles were reviewed to determine whether they addressed rehabilitation. Criteria for qualifying as rehabilitation was that the CPG aimed to improve, maintain, or restore human function and/or provide treatment(s) designed to facilitate the process of recovery from injury, illness, or disease to as normal a functional condition as possible. The definition of the word “function” in this context is taken from the International Classification of Functioning, Disability and Health (ICF). Functioning, as used in the ICF descriptions is defined as “a dynamic interaction between her or his health conditions, environmental factors, and personal factors” (World Health Organization, 2018). The criterion for “rehabilitation intervention” was that there be a specific rehabilitation treatment recommended, not a general comment about “refer to rehabilitation, physical or occupational therapy” and that a functional outcome measure was included in the methods section. The search process followed the PRISMA algorithmic approach using the inclusion and exclusion criteria (Moher et al., 2015). A schematic using this approach is presented in Fig. 1. The specific articles were reviewed as described above and selected for inclusion after meeting all criteria. The summaries of the articles reviewed which we selected for this report include: title of the article; the journal in which it was published; authors and the professional affiliation of the endorsing organization (E.g. Monash University, French Society of Physical and Rehabilitation Medicine et al); the setting for which the guidelines apply (E.g. acute care, post-acute care, community-based care) (Table 1). A brief summary of the recommendations made by each of the guidelines is also provided. Information gathered from publications addressing TBI and rehabilitation which did not undergo a standard vetting process by the practice guidelines developers, but had informational value or included TBI as one of many conditions in the guideline development process (E.g. disorders of consciousness or stroke), is also provided for informational purposes (Table 2).
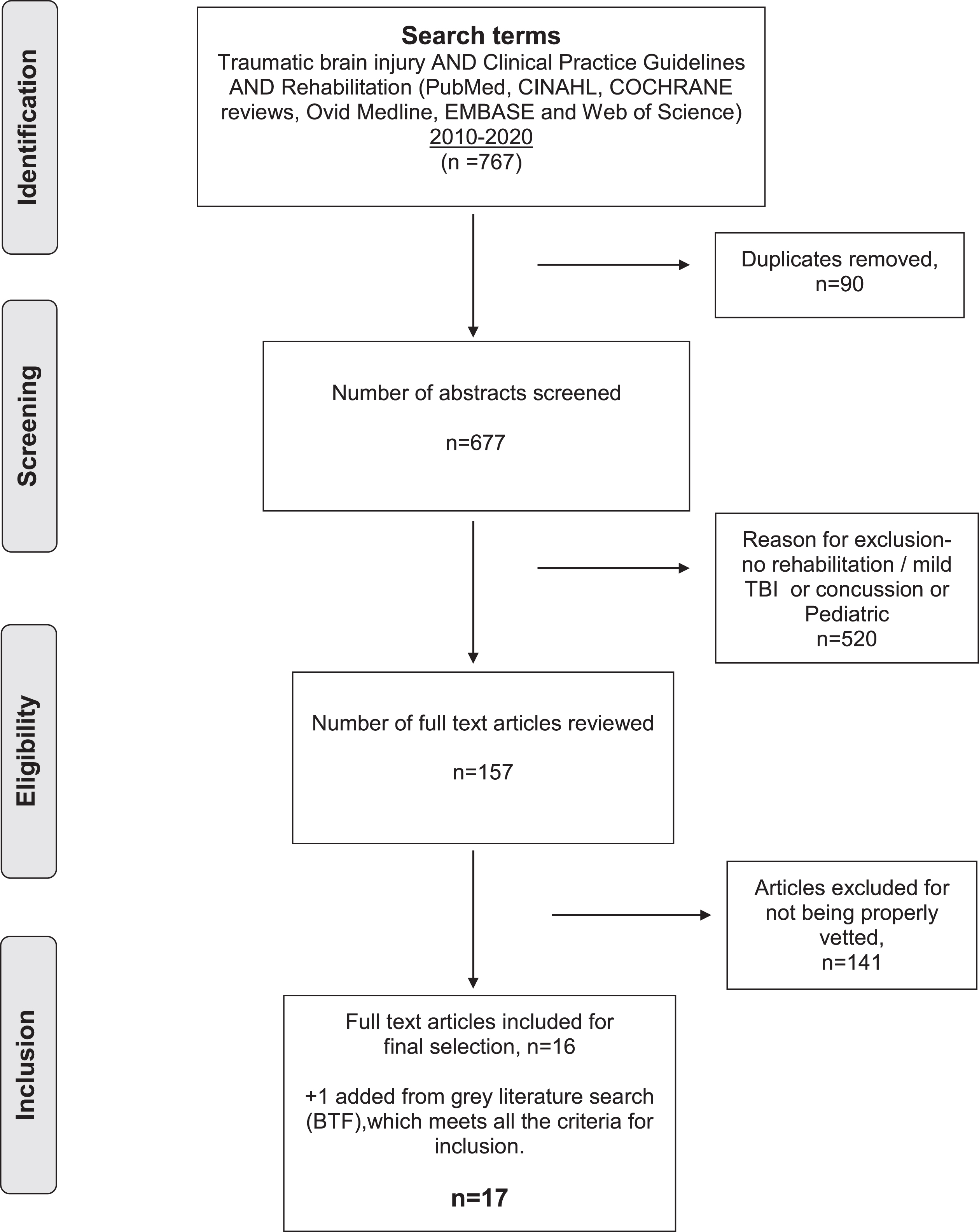
The PRISMA flowchart of the results from the database searches.
All entries have met criteria for inclusion and have no exclusions. One reference was added as a result of Google search that was not retrieved from the database searches
All entries were retrieved from database searches. None of the references identified specific rehabilitation prescriptions, but did mention recommendations for referral for general rehabilitation or physical/occupational therapies
Additionally, the publications were evaluated using the Appraisal of Guidelines for Research and Evaluation (AGREE II) (3). The AGREE II template is a validated instrument for appraising CPGs (https://www.agreetrust.org/wp-content/uploads/2016/02/AGREE-Reporting-Checklist-2016.pdf) which comprises 23 questions grouped into 6 domains: 1. scope and purpose of CPG; 2. Stakeholder involvement; 3. Rigor of development; 4. Clarity of presentation; 5. Applicability; 6 editorial independence (Brouwers et al., 2016). All CPGs that met inclusion criteria were further assessed for meeting AGREE II requirements.
There were 767 articles retrieved when applying the search terms. There were 90 duplicates leaving 677 for abstract review. Following this, 520 were eliminated after full reading of the manuscript they did not meet inclusion criteria. Some did not address rehabilitation or addressed mild TBI or concussive injury, leaving 157 articles for review. One hundred forty-one did not specify any vetting or standard review process, leaving 16 that met inclusion criteria and no exclusion criteria. A Google search for key search terms identified one CPG that had not been retrieved from the database searches. This was a CPG from the Brain Injury Foundation and was included in the final count. An additional summary publication included CPGs and other aspects about TBI management and diagnosis but did not meet criteria for CPGs (Togher et al., 2014). The total number of CPGs for TBI (excluding mild/concussive injury) is 17 (Bayley et al., 2014; Brain Trauma Foundation, 2016; Doncevic & Boerman, 2010; Honan et al., 2019; Levine, 2016; Maas et al., 2017; MuCulloch et al., 2016; Ontario Neurotrauma Foundation, 2015; Pattuwage et al., 2017; Ponsford, 2014a, 2014b; Scholten et al., 2017; Stergiou-Kita et al., 2012; Tate et al., 2014; Togher et al., 2014; Uomoto, 2012; Velikonja et al., 2014). These data are presented using the PRISMA flow diagram (Fig. 1 and Table 1). Tables for CPGs meeting all criteria included: title of the article and authors; the journal in which it was published; the professional affiliation of the endorsing organization (E.g. Brain Injury Foundation, International Group of Researchers and Clinicians (INCOG) etc.); the setting for which the guidelines apply (E.g. acute care, post-acute care, community-based care); and, which vetting criteria were used (E.g. IOM, Oxford, USPSTF, et al.). A brief summary of the recommendations made in each of the guidelines is also provided.
Information gathered from publications addressing TBI and rehabilitation which did not undergo a standard CPG vetting process, is also provided in a separate table for readers’ comparison.
These 17 were further evaluated using the AGREE II template (Table 1). There were 4 that met all 6 criteria and 10 that met 5. The missing domain was “editorial independence”. One CPG met 3 criteria, one met 2 and one met one criterion. The CPG that only met a single criterion was reported as “Continuum of Care” and the other, that met only 2 criteria was titled “Best Practices”.
During the review process, additional articles were identified that used CPGs in the title but were not, in fact CPGs. They were literature and systematic reviews of CPGs, practice guideline reviews and/or specialty societies appointed to develop guidelines without an established vetting process. These are presented in Table 2 (Chantsoulis et al., 2015; Cicerone et al., 2019; Farrell & Bendo, 2018; Giacino et al., 2018; Kolias et al., 2013; Kondziella et al., 2020; Lee et al., 2019; Levine & Flanagan, 2010; Lump, 2014; Martelli et al., 2012; Nielson et al., 2015; Stephens et al., 2015). One CPG was developed using a Delphi process following an American Academy of Neurology process (Giacino et al., 2018). While this is a rigorous approach to the quality of the publications reviewed, it omits several key features of the vetting process and was assigned to Table 2.
Discussion
One of the most challenging tasks in the practice of medicine is to be sure of the effectiveness, safety and reliability of practice recommendations. These characteristics are essential if we wish to bring new, research findings into practice. Possible hurdles to accomplishing this goal, especially in clinical rehabilitation research, include the small sample sizes in most studies, the personalized nature of the deficits and disabilities, lack standardized interventions and common data elements for functional outcomes and dependencies on patient reported outcomes (Dijkers et al., 2020). These are challenges, but can be overcome and accommodated. Several researchers in the field of clinical rehabilitation research have been working on approaches to link best evidence within the context of the kind of research that is typically done in physical medicine and rehabilitation and preserve quality (Negrini, 2016, 2018).
Specifically, this review demonstrates several key themes evident from reviewing CPGs for people with TBI There is a paucity of intervention trials addressing rehabilitation outcomes for this population. We have chosen to include rehabilitation as a necessary component of the review, one that includes function as an outcome. This would, in our opinion, be especially valuable for the multi-disciplinary professionals from different backgrounds responsible for the care of people with TBI (E.g. neuropsychologists, physiatrists, occupational and physical therapists et al.).
In prior work (see Gerber, 2019, for more detail), it has been shown that there are relatively few intervention trials addressing functional outcomes for people with TBI and therefore, the number of publications available for systematic reviews is low. This creates a problem if one is to reach a high level of evidence. In this review, a total of 157 were found, 141 of these were eliminated from the final cut because they were not vetted or no vetting process was cited. Many of the CPGs addressed concussive injury rather than moderate to severe TBI, hence were eliminated for the purposes of this review. While not all of the final 17 CPGs that met inclusion criteria met the guidelines for AGREE II in all 6 domains, all met some and 4 met all.
An additional issue that needs to be addressed when applying CPGs is quality of the data supporting the recommendations. This was discussed in a recent publication (Dijkers et al., 2020). It reviewed the published CPG literature and determined that there has been an increase in the number of CPGs published over the past 20 years, reaching more than 7000 listed in PubMed as of May, 2020. In that review, the following search terms were used;, “(physical medicine)OR (rehabilitation) AND (clinical practice guideline))”. When approaching the question of quality, they applied the AGREE II template to CPGs. They reported that all 6 domains of the AGREEII were good predictors of quality, and that Domain 3 (rigor of development) was the strongest predictor, suggesting emphasis on rigor of development will improve quality among CPGS (Dijkers et al., 2020). Not all review processes apply the AGREE II template. Using it would be an important step forward.
Another important finding from this review is that the published guidelines frequently address issues of symptom control. Clearly, these are clinically important issues facing patients but, in the view of these authors, should be linked to functionally based outcome measures. For example, 6 CPGs addressed treatment of symptoms only (spasticity/deformity/contractures, depression/anxiety, amnesia, memory loss, mental health, dizziness) with no mention as to whether there was a functional impact of symptom control. Nine used functional measures as primary or secondary outcomes for their studies and 2 of these provided an integrated approach to function across several domains of measure (impairment, functional limitation and participation) as well as in different stages of recovery. There were 2 studies that provided guidelines for the selection of outcome measures, both of which used a conceptual framework addressing the needs for people with TBI across the continuum of care and included multidomain measures. The use of outcome measures that address the functional needs of people with TBI is critical to assessing rehabilitation outcomes. The use of functional measures as primary or secondary outcomes is an important design feature of all clinical rehabilitation research. The acceptance of a multidomain model and effort to extend beyond the acute care setting into the community and assessment of independent living status is another desirable outcome for clinical rehabilitation research.
We made some choices as we planned this review. These included selecting publications that addressed moderate or severe TBI and not all brain injuries. This was arbitrary but is of significant concern because of its complexity, its need for coordinated rehabilitation interventions. Because of the multi-domain problems for people with moderate/severe TBI, we required that when rehabilitation intervention(s) were recommended, they needed to address a specific need and include specific interventions not only a comment “refer to rehabilitation, physical/occupational therapy”. General referrals are frequently supported by expert opinion without literature resulting from intervention trials.
The items selected for inclusion in the tables, we hope, will provide readers with a ready reference to the CPGs that met criteria. As part of the vetting process, it is recommended that sponsors for CPG development be identified to be entirely transparent about whether there was funding for the effort. Occasionally, bias can be introduced into final recommendations for practice and readers should be aware of sponsors for the guideline development. Additionally, CPGs expand the knowledge base for treatment options when they consider important patient subgroups and patient preferences and provide a clear explanation of alternative care options and health outcomes. When studies CPG development was rigorous, but did not include these options, they were assigned to Table 2, which are informative and many have utility in advancing practice.
We acknowledge that concussive and mild TBI is prevalent, important and in need of continued research. However, because the level of severity, the types of interventions and determination for longer term followup in this population may require different research designs, treatments and data gathering approaches, we chose to address only moderate/severe TBI. Another decision was made to exclude publications published before 2010. This was decided because the field is changing quickly and the number of reviews, studies and practice changes are increasing rapidly and we wished the review to be current. We acknowledge that creating CPGs is time consuming and labor intensive and hence there is likely to be a significant amount of time that elapses between in preparation and publication. Nonetheless, currency is important in clinical care. We are surprised that some of the most comprehensive and well documented CPGs are more than 20 years old and have not been updated as of this review (Maas et al., 1997).
The development of reliable CPGs requires a careful, time consuming process. When done properly, we believe, they are an important resource for primary care practitioners, first responders and family who may have little experience with evaluating, transporting and managing problems associated with TBI. CPGs can provide needed, reliable and up to date information. In an under-sourced specialty such as physical medicine and rehabilitation, they are essential contributors to the field.
Conclusion
There are relatively few CPGs addressing rehabilitation for people with moderate or severe TBI. Remedies for this situation might include stimulation of more rehabilitation intervention trials, use of functional outcome measures as primary and/or secondary outcomes and possible inclusion of patients in selecting outcomes that are relevant and useful to this stakeholder group. One approach that may contribute to increasing the quality of CPGs, would be convening a group of investigators and relevant stakeholders to try to reach consensus on which measurements of function should be used in these studies. Commitment to strong metrics is likely to raise the level of evidence for intervention trials. Since many published CPGs have not been vetted to comply with published standards of reliability and trustworthiness for implementation for practice, journal editors should require all published CPGs to follow an accepted vetting process so that users are assured of their quality and trustworthiness. The addition of a template such as AGREE II, would also improve their quality.
Conflict of interest
The authors have nothing to declare.
Funding
This work was funded through a subcontract to Inova Health System from the American Institutes for Research, supported by NIDILRR Federal Grants #90DP0082, #90DPBU0001, and #90DPBU0004.