
Abstract
Destructive outcomes of coronavirus pandemic call for medical research which can report all of the influential agents not only for the treatment of the disease but also preventing its severe impacts on the societal health in the most efficient manner. Zinc plays an integral role in the function of cellular enzymes and transcription factors. Owing to its anti-inflammatory and cellular immunity regulation activity, zinc is regarded to be effective on strengthening the immune system. Its crucial antiviral effects have long been established as well. Studies suggest that low serum zinc level predisposes the patient to severe COVID-19 infection, which makes patient’s zinc profile a potential determinant of prognosis and severity of this disease. Furthermore, zinc supplementation has indicated promising outcomes of coronavirus infection management. Zinc modulates cell-mediated immunity and participates in the killing of microorganisms in cytotoxic immune cells. Zn2+ has anti-inflammatory effects by inhibiting IL-6 production. Although there is still not enough evidence, it seems that zinc could be a promising supplementary treatment for COVID-19 especially in zinc-deficient patients. The aim of this review is to clarify the role of zinc in pathogenesis and therapy of COVID-19 in detail.
Introduction
Since March 2020, a pandemic caused by coronavirus (SARS-COV 2) was declared by the World Health Organization. For the first time, COVID-19 was diagnosed in Wuhan, central China, in December 2019 [1, 2]. Up to September 15, 2021, more than 4 millions of deaths has been reported worldwide [3]. The disease is less frequent in children and the symptoms are less severe within this age group [2]. Male gender, age older than 60 years, obesity, pre-existing chronic metabolic diseases including hypertension, diabetes mellitus, chronic obstructive pulmonary disease (COPD), coronary artery disease, cancer, and immunodeficiency are related to the severity of infection [1].
An effective treatment protocol is crucial in tackling with this pandemic [4]. Although there is no known specific treatment yet, some drugs and supplement therapies such as zinc, selenium, vitamin C and vitamin D are highly recommended [5, 6].
Considering the role of zinc in boosting the immune system, its protective role against inflammation and reactive oxygen species (ROS) together with evidences of higher severity of the COVID-19 infections in zinc-deficient pateints, zinc supplementation has been assessed in several clinical trials [7–11]. Due to the synergistic effects of zinc on anti-viral drugs and its inhibitory role on SARS-CoV-2 replication it can be a remarkable candidate for COVID-19 treatment [10].
The aim of this review is to clarify the role of zinc in pathogenesis and therapy of COVID-19 in detail. Given the proven role of zinc in cellular function and immune system [10], hereby, we have prepared an overview of the latest clinical data on the role of zinc in the pathogenesis and treatment of COVID-19.
Methods
This integrative review was performed by searching PUBMED data base using the following keywords: [“COVID-19” OR “SARS-CoV-2” OR “2019-nCoV”] AND [Zinc] up to October,1st 2021. The search was limited to clinical trials published in English and those conducted in humans and those mentioning zinc role in COVID-19 pathogenesis and treatment. At first, 428 articles met the inclusion criteria. After excluding articles that did not match our target scope based on their full-text content, 91articles entered the study.
Data were categorized according to zinc‘s metabolism, its role on health and immunity and the pathogenesis of zinc in SARS-COV-2 infections or treatment.
Zinc metabolism
Zinc, the second most aboundant cation of the body, is a necessary trace element that acts as a cofactor in more than 300 enzymes [12]. Zinc can be found in different foods such as fish, meat, egg, nuts and legumes [12]. Absorption of this concentration dependent trace element is determined by the type of diet, the amount of phytic acids [13], iron [14] and proteins [15] of the foods and the zinc status of the body [16, 17]. Therefore it seems that it would be absorbed more efficiently in diets with poor sources of zinc by upregulating its retention [16].
In cell nucleus or other organelles, zinc is distributed by vesicles called zincosomes and in the cytoplasm it binds to metallothioneins. Zinc transporters are membrane transport proteins that regulate the concentration of zinc through influx or efflux of zinc [18]. Internal zinc hemostasis is mostly controlled by two zinc transporter families which are essential for survival [18, 19].
A balance between zinc absorption and intestinal excretion maintains zinc hemostasis [20]. Although absorbed zinc is secreted through biliary tract and intestines, a great amount is reabsorbed. Gastrointstinal tract is responsible for more than half of the eliminated zinc [16]. The excreted zinc is in balance with the dietary intake, the amount of absorption and the physiologic needs [17]. Daily requirement of zinc increases during infancy, childhood, adolescence, pregnancy and lactation [16]. Moreover, elderly people have low level of zinc in their diet [21]. Figure 1 shows the summary of zinc metabolism.
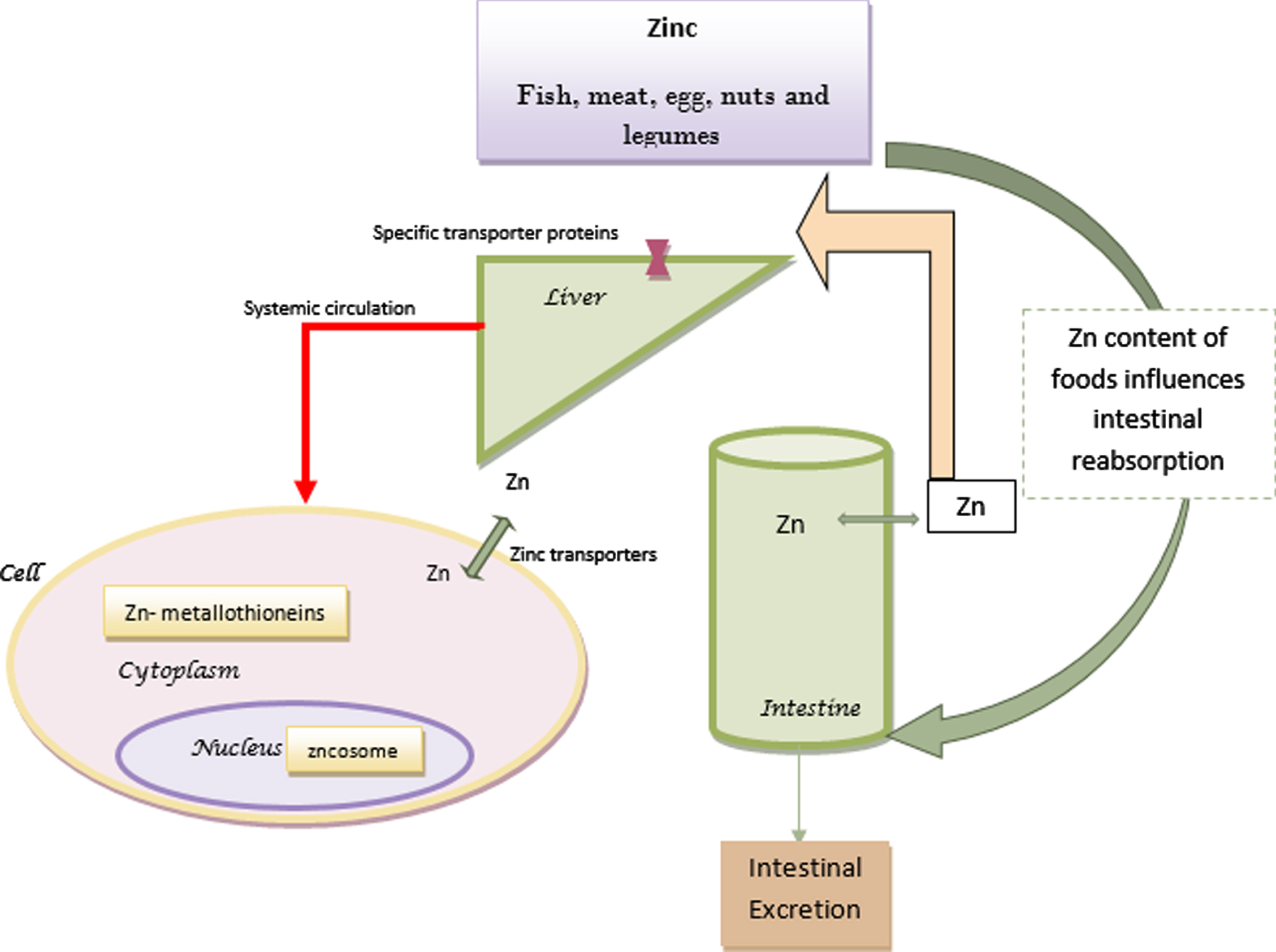
Zinc metabolism.
The majority of zinc in the plasma is bound to albumin, alpha-2-macroglobulin (A2M), and transferrin, however, there is a very small amount of free zinc in the plasma that is still very important for its homeostasis [18, 22]. Insufficient zinc in the diet, increased requirments, impaired absorption and abnormal losses may lead to zinc deficiency [16].
Zinc maintains cell membrane integrity; is important in cellular proliferation, DNA and RNA replication, gene expression and regulates the function of T, B and natural killer cells [23].
Skin, gastrointestinal tract, central nervous system, immunologic system, bones and genitourinary tract may be affected by zinc deficiency [16]. The role of zinc in human health have been clarified since the detection of a patient with anemia, hypogonadism and dwarfism in Iran in 1961 [24]. The relationship of zinc deficiency and febrile seizure is well considered in different studies [25, 26]. Acrodermatitis enteropathica is a well-known disease caused by zinc deficiency [16]. Many studies pointed out the effect of zinc deficit on impaired growth and development [27]. Moreover zinc may have a protective effect on inflammation and atherosclerosis [28].
In the elderly it is suggested that reduced immunocompetence, wound healing impairments (non-healing skin ulcers) and neurological problems are partly due to zinc deficiency. Psychological changes such as impairment of memory, mentality, cognitive functions and behavioral problems may be caused by zinc deficiency [16]. Furthermore, growth retardation and alopecia can be seen in zinc-deficient children. Given that malnutrition and infections are among the most common causes of mortality and morbidity in childhood, zinc supplementation may have preventive effects on childhood death [29]. Adminstration of this trace element can protect children against childhood obesity and metabolic syndrome [30, 31].
The consequenses of zinc deficiency in infections has been extensively studied. It is reasonable to control serum zinc level during infections, due to transient hypozincemia during infection and inflammation [13, 17]. It is hypothesized that in patients with prior hypozincemia, decreased transient zinc level during infections may cause hyperinflammation [18]. Due to poor hepatic reserve of functional zinc, during increased zinc demands like infections, the required amount could not be delivered to plasma [12]. The relation between diarrhea and zinc deficiency can be explained by the alteration of zinc transport across intestinal mucosal cell and the negative impact of zinc deficiency on immune system [16]. Zinc supplementation in children has also significantly decreased the frequency of pneumonia in developing countries [16] and malaria episodes in endemic areas [32].
Zinc and immunity
The function and folding of cellular enzymes and transcription factors depend highly on zinc cations. Zinc is also a co-factor of viral proteins. It is also noteworthy that zinc affects viral proteases and interferes with viral polyprotein folding [33, 34].
In the human body, the first defensive mechanisms against infectious agents are ciliary mucous membrane and anti-microbial peptides [35]. By controling tight junction proteins, zinc supports mucous membrane coherence [12] and protects cells with blockage of virus entry [33]. Moreover, it increases ciliary beat frequency [36] and improves ciliary length of bronchial epithelium [37].
In viral infections, zinc can interfere with membrane fusion, protein translation and stabilization of viral envelope, the function of viral polymerase, liberation of viral particles and uncoating [35, 38].The inhibitory action of zinc on viral replication has been illustrated on rhinoviruses, HCV, and influenza virus. In Nidoviruses, of which SARS COV- 2 is a member, zinc can decrease RNA synthesis [33]
Zinc has favourable impacts on adaptive and innate immune cells and enhances their growth, development, and function [39, 40] such as: development of Th17, Th9, and regulatory T cells, production of IFN γ, complement system activity, cytokine production and release, cytotoxic function of NK cells, proliferation and differentiation of T cells [41, 42], and IgG production [42, 43].
Zinc may restrict infection by the production of IFN-γ. The production and antiviral effects of IFN-α (human interferon alpha) are also influenced by this trace element [18, 44]. Zinc downregulates IL-1b and TNF-alpha expression and inhibits Nuclear Factor kappa-light-chain-enhancer of activated B cells activity (NF-kB) and therefore decreases inflammatory cytokines that are important in severe lung inflammation [16]. IL-6 is a key factor in cytokine storm and higher IL-6 responses are seen in hypozincemia [18].The zinc deficiency in obese and elderly patients may increase IL-6 levels. In addition, gene expression of IL-1 alpha, IL-1 beta, and IL-6 are increased in obese patients with reduced zinc levels [18].
Zinc is responsible for the secretion of pro-inflammatory cytokines and it suppresses inflammation by inhibition of leukocyte function-associated antigen-1 binding to ICAM-1 [45].
This trace element can inhibit the transfer of proteins across capillaries and reduces edema and inflammation [46]. Moreover, zinc is essential in the IL-2-dependent proliferation of T cells [47] and increases cell’s resistance to apoptosis [48] which can result in the increase of T helper cells [46]. It also protects against the adverse effects of Reactive Oxygen Species (ROS), that has a main function in the progression of inflammation [10].
It was proposed that the excess level of intracellular zinc causes metal ion poisoning of pathogens in the innate immune cells. The excess zinc results in mismetallation of essential proteins and impairment of other metal trace elements of microorganisms. It seems that zinc can also influence nitric oxide production in the innate immune cells and therefore help the free radicals to attack intracellular pathogens. The resistance of these pathogens depends on their detoxification systems [49].
Alternatively, zinc deficit is accompanied by thymic atrophy, decreased number and impaired function of T cells and changes in the production of thymic hormones. It is supposed that thymulin which is important in the function of peripheral T cells and differentiation of immature T cells in the thymus is decreased in zinc deficiency. Therefore an increased risk of infection can be seen with zinc deficiency because of altered cellular- and antibody-mediated immune responses [33]. Furthermore, zinc deficiency is responsible for impaired phagocytosis and neutrophil function, lymphopenia, decreased antibody and IFNγ production which may increase the risk of infection [12].
Adequate immunity needs balanced zinc levels because elevated zinc levels cause inhibition of T and B cell function, impairment of a destructive function of macrophages, and overload of regulatory T–cells, that may harm the immune function as well [12].
The pathogenesis of zinc in SARS-COV-2 infections
SARS-COV-2 the newly introduced member of Coronaviridae family, is approximately 50–200 nm in diameter. It has a single stranded nonsegmented positive-sense RNA covered with neucleocapsid, membrane proteins and spike proteins [50]. The first infected cells with this virus are nasal and bronchial epithelial cells and pneumocytes [51]. SARS-COV-2 attaches to angiotensin-converting enzyme 2 (ACE2) receptors via spike glycoprotein (S protein), and then enters these cells [10]. ACE2 is a zinc metalloenzyme [52] and its expression is influenced by this trace element. Therefore, any impairment of gene expression in pneumocytes influenced by zinc can modify viral entry [35]. After entry, the virus is transported by endosomes in the cytoplasm, subsequent to the low pH of the endosome, viral envelope fuses with endosomal membrane, releasing the positive-strand viral RNA (+RNA) [10].
SARS-COV-2 poly proteins (pp1a and pp1ab polyproteins) are translated by using the 5′-proximal open reading frame (ORF1a and ORF1b) which at last result in the formation of sixteen nonstructural proteins [10]. These nonstructural proteins bind to the replicase–transcriptase complex and undergo cloning and transcription and participate in the formation of viral membrane structures [10, 53]. RNA-dependent RNA polymerase (RdRp) domain which is in nonstructural protein 12, together with the two encoded cysteine proteases, main protease (Mpro) and papain-like protease (PLpro), are targets for SARS-COV-2 future therapy. For instance, Disulfiram can have an inhibitory effect on PLpro and Mpro. This is caused by releasing zinc from these enzymes and destabilizing them concurrent with an increase in cytoplasmic zinc levels [53]. Some studies showed that high levels of cytoplasmic zinc could inhibit RdRp action and replicase polyproteins [54]. RdRp is united with a viral enzyme complex leading to the formation of a negative RNA chain which will be a template for viral mRNA synthesis [10]. The similarity of more than 95%RdRp with SARS-COV-2 protease together with the inhibitory effect of zinc on RdRp, can lead to the idea that zinc can have antiviral effects on this virus [33].
In vitro studies have shown the effectiveness of zinc on rhinovirus, RSV, and SARS-COV-2. They have demonstrated that Zn2+ has inhibitory effect on SARS-COV replication in cell culture [54]. Zinc can inhibit papain-like protein 2 that is crucial for SARS-COV virulence [55].
During the first phase of COVID-19 disease, the release of cytokines and chemokines are delayed. However, at the later phase of the disease, the level of interleukins (IL) IL-1β, IL-6, tumor necrosis factor (TNF), chemokines, and interferon are increased and is called as “cytokine storm” [56–58]. The inhibition of NF-kB (nuclear factor kappa light chain enhancer of activated B cells) by zinc may have anti-inflammatory effects and limit the cytokine storm [59, 60].
Lung damage in COVID-19 is related to increased IL-6; IL-6 reduces zinc bioavailability by inducing expression of zinc bounded proteins like metallothioneins (MT) and alpha-2-macroglobulin (A2M). Zinc reduces IL-6-mediated activation of the Signal transducer and activator of transcription 3 (STAT-3) thus has anti-inflammatory action [18].
The role of zinc in inhancing drugs’ effects
The synergistic action of zinc with some antiviral agents in treatment of viruses like hepatitis C, HIV, SARS-CoV-1 has been demonstrated [33].
Inhibitors of Mpro may act against many types of coronaviruses but drugs for PLpro or RdRp may act against SARS-CoV-2 and SARS-CoV [33, 61]. Ionophores are molecules that facilitate ion transport across cell membrane and their action depends on the pH changes. Some drugs act as zinc ionophores like Disulfiram and Chloroquine [53]. Chloroquine disrupts lysosomal acidification and therefore has cytotoxic effects. Chloroquine can also increase zinc absorption and when combined together, its efficacy and cytotoxic effects are increased [10]. Same mechanism is explained for quercetin and epigallocatechin-gallate but with lower cytotoxic effects [62]. Other drug targets in viral infections are zinc fingers. Zinc fingers are protein structural motif in a great number of viral proteins, which contain cysteine, histidine, and attached zinc [63]. The three-dimensional structure of these proteins and their foldings are maintained by the presence of zinc [53]. “Labile zinc fingers” can release Zn2+ which will make the protein unfolded and increase cellular zinc level. Agents that are capable of removing zinc from zinc fingers in viral metalloenzymes are under investigation. They can destabilize viral proteins and increase intracellular zinc [53]. If zinc is administered with an ionophore, the increase of intracellular zinc will be remarkable which can inhibit viral RdRp and therefore viral mRNA synthesis. In addition to the decrease of protein synthesis, an increase of intracellular zinc can lead to apoptosis [53].
Zinc and COVID-19
Surprisingly, diseases that are considered to be the risk factors of COVID-19 such as chronic obstructive pulmonary disease (COPD), obesity, diabetes mellitus, malignancy, coronary artery disease, cirrhosis, and suppression of the immune system are also accompanied with a low serum Zn2+ level [35].
Moreover, due to the reduced sense of smell and taste in zinc deficiency, these symptoms which are seen in COVID-19 infection as well, can be attributed to transient zinc deficiency during infection [18].
Also, elderly are at increased risks of infections, COVID-19, cancer, and autoimmune diseases. Aging leads to immunosenescence (age-related changes of the immune system). These changes may be contributed to zinc deficiency that may be a result of low intake, decreased absorption, and/or drug interactions with zinc [64].
Findings showed that the efficacy of some drugs used in the treatment of COVID-19 such as ribavirin, remdesivir, lopinavir/ritonavir, azithromycin and doxycycline is improved with zinc supplementation [10].
Despite numerous scientific data about the effect of Zn2+ on infection in the literature, very few clinical trials have been performed about the relation of zinc and COVID-19. As of October 1st 2021, 67 studies were found after searching with the keywords “zinc” and “COVID-19” at the clinical trial website https://clinicaltrials.gov/ct2/home. Among 55 clinical trials, studies with no intervention of Zn2+ supplementation to the patient were excluded. From 24 remained study, 14 used a combination of zinc with different drugs, vitamins or trace elements. Only 10 studies invested on zinc alone in the experimental arm from which 4 were completed but none of them had reported their results. Data are summarized in Table 1. Other studies with reported zinc effects on COVID-19 are summarized in Table 2.
Clinical trials with zinc+other drugs/dietary supplements for COVID-19
Clinical trials with zinc+other drugs/dietary supplements for COVID-19
Studies with reported zinc effects on covid-19 patients
It has been seen that Zinc addition may decrease hospital stay and accelerate recovery in children with Lower respiratory tract infection [65]. Another double blind trial has demonstrated a faster recovery of pneumonia in children with zinc supplementation. Moreover, the study mentioned reduced antibiotic resistance with zinc administration [66].
In a recent study in Japan on 62 patients with COVID-19, the severity of the disease was significantly related to low serum zinc levels. According to this study, prolonged hypozincemia may increase the severity of COVID-19 [67].
In another study on 47 patients with COVID-19, the fasting zinc levels were significantly reduced compared to controls. In zinc deficient patients, the chance of experiencing complications, hospital stay and mortality were much higher (with the Odds Ratio of 5.54) [68]. Furthermore, in a study by Finzi et al., a 24 hours supplementation of high dose zinc (115–207 mg daily) showed significant improvement of symptoms in all 4 studied patients [69].
A retrospective study by Carlucci et al. in 2020 showed that addition of 50 mg zinc sulfate twice daily for 5 days to hydroxychloroquine can decrease the mortality rate in patients who were not treated in ICU [70]. As explained previously, there are reports mentioning the role of chloroquine as an ionophore for Zn. Therefore the amount of zinc absorption by the lysosome is intensified. As a result, the cytotoxicity of chloroquine is boosted when combined with zinc supplements [10].
Although most of studies supporting zinc supplementation in COVID treatment, there were several studies showing contradictory results.
A result of a recent published clinical trial in Egypt that conducted on 191 COVID-19 patients treated with hydroxychloroquine or chloroquine with or without zinc sulfate supplementation, did not show any significant difference in the mortality, the necessity of mechanical ventilation and clinical improvement between cases and controls [11].
A retrospective study by Yao et al. did not find a significant association in survival of hospitalized patients with COVID-19 who were treated with zinc sulfate compared to control group [5].
In the study performed by Natarajan et.al, the viral load reduction was compared between two groups. The first group used a mixture of 15 herbal drugs, known to have anti-pyretic, anti-inflammatory, and anti-bacterial effects. The second group were given daily oral tablets of zinc (100 mg) and vitamin C (60,000 IU).The results showed significant decrease in the CT value of RT-PCR in both groups, but the mean difference in the CT value was more notable in the herbal group [71].
In the retrospective chart review of 102 critically ill COVID-19 positive patients performed by Capone et al, patients treated with vitamin C plus zinc had no overall survival impact in comparison to the intravenous immunoglobulin (IVIG) and anticoagulation group [72]. This may be caused by the patients’ status when invested since zinc is more beneficial in mild illnesses.
Despite various studies mentioned about zinc supplementations in the treatment of COVID-19 patients, there are still insufficient data explaining the exact mechanism of its effects.
It is important to mention that high dose zinc usage for a long period can damage lymphocyte and neutrophil functions and disturb the immune system responses [73]. The adverse effects of high doses of zinc consumption are anemia, genitourinary tract complications, and consequences of copper deficiency [74, 75]. However, to support immune system, it seems that it is better for cancer patients to receive zinc supplement for up to three months [75].
It should be considered that gastrointestinal absorption, diet, abnormal excretion and drug interactions can influence the effect of zinc. As explained by Das RR, the benefits of zinc supplements take around 100 hours to be notable. Thus in acute scenarios there is not enough time for an adequate response [76]. This may explain the different responses seen in patients.
The present study has some limitations. First, the reviewed articles only obtained from PUBMED database. Second, most of related clinical trials has not been published yet; so, certain effect of zinc therapy on COVID-19 treatment cannot be determined.
In conclusion, findings of the most reviewed articles approved the effect of zinc supplementation on reducing the chance of complication, length of hospital stay and mortality rate of COVID-19. Although there is still not enough evidence, it seems that zinc is beneficial as a supplementory treatment for COVID-19 especially in zinc deficient patients. Zinc inhibts viral replication and excess cytokyine relase, thereby protects against lung damage. It can also inhance anti-viral drug effects causing shorter duration of disease specially in milder cases. Considering that gastrointestinal absorption, diet, abnormal excretion and drug interactions can influence the effect of zinc, for future trials, we recommend to match these factors in the study groups. We also recommend performing cohort studies in order to determine preventive role of zinc in COVID-19.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Author’s contribution
All authors contributed equally to this project.
Conflict of interests
There is no conflict of interests.
Funding/support
This study did not receive any funds or financial support.