
Abstract
BACKGROUND:
Renal cysts are the most frequently occurring incidental renal lesions. They are asymptomatic, which explains why they tend to be diagnosed incidentally as a result of imaging tests. In cases where malignancy is suspected, there are various therapeutic alternatives.
OBJECTIVE:
The objective of this study is to review the diagnostic and therapeutic alternatives for cystic renal lesions.
METHOD:
A systematic search was conducted in Pubmed, Science Direct, Scopus, and Google Scholar databases between May and October 2022. The review of articles was conducted following the methodological recommendations of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 Statement. As a result, 25 articles were selected.
RESULTS:
Thirteen studies focused on diagnostic management. In five of the cases ultrasound was used, multiparametric magnetic resonance imaging (mpMRI) was considered in six articles, and computerized tomography (CT) was studied in three. Eleven papers were retrospective series, one of the studies was prospective, and one was a simulated cost-effectiveness model. Among the 12 articles on treatment, five focused on surgery and one on the results of active surveillance, while three compared active surveillance with other treatments. Four articles assessed the percutaneous approach and radiofrequency ablation. All articles were retrospective cohorts.
CONCLUSIONS:
CT is the most standard of the tests. In doubtful cases, mpMRI and ultrasound can serve as complementary tests. Partial nephrectomy is currently the gold standard treatment and the results are similar for both open and laparoscopic approaches. Percutaneous radiofrequency treatments produce reasonable survival rates free of local recurrence and metastasis and are recommended in patients with high surgical risk.
INTRODUCTION
Renal cysts are cortical or medullary cavities, simple or multiple. They are benign and filled with fluid, and they often go unnoticed. Renal cysts constitute the most frequently occurring incidental lesions in the kidney, representing more than 70% of asymptomatic renal tumors [1–3]. Their origin may be due to various causes such as family syndromes, sporadic appearance, or the terminal stage of dialysis patients. However, renal cystic lesions are predominantly asymptomatic, which explains why they are usually diagnosed incidentally as a result of different imaging tests, such as ultrasound, CT or mpMRI [4]. The Bosniak classification is the method most widely used to characterize renal cystic lesions, assessing the probability of benign lesions or concomitant malignant disease within the cyst. This classification is based on the findings detected by CT. Simple renal cysts (Bosniak class I) are cystic lesions with a well-defined, thin (<2 mm), smooth wall and homogeneous simple fluid, and without septa or calcifications as seen on CT or mpMRI. In addition, an ultrasonographically-based definition (i.e., a round or oval cyst with a thin, smooth, sharply marginated wall and no evidence of calcification or malignancy), is also commonly accepted. According to this classification, when the cyst is classified between groups I, II, and IIF, the probability of malignancy is low; therefore, treatment is not recommended, but follow-up of evolution for class IIF is appropriate. The risk of malignancy increases in classes III and IV, however, and treatment is recommended in those cases [5]. Around 10% of renal cell carcinomas (RCC) are cystic, while some benign cysts display a more complex appearance in conventional diagnostic tests such as CT or mpMRI. These renal complex cystic masses (RCCMs) are challenging in urological practice, and sometimes need complex management, requiring surgical removal [6]. Currently, among the most frequently used available treatments are percutaneous drainage or sclerotherapy in the case of symptomatic renal cysts, and a laparoscopic or robotic surgical approach in the case of suspected malignancy [7]. Nephron-sparing approaches such as partial nephrectomy, tumor enucleation, and percutaneous ablation (e.g., cryoablation, radiofrequency, and microwave ablation) are viable options for the treatment of these tumors and preserve renal function while lowering the risk of cardiovascular events and overall mortality [8].
The present study consists of a systematic review of the previous literature on the management of acquired cystic renal lesions with a suspicion of malignancy, both at the diagnostic level through imaging tests and treatment (both active and surveillance), excluding polycystic syndromes and hereditary renal disease, as well as the management of symptomatic cysts. This study aims to show which diagnostic and therapeutic techniques yield the best results for the management of those renal cystic lesions suspected of malignancy according to currently available scientific evidence.
MATERIAL AND METHODS
Data sources and searches
A systematic search including the terms ‘cystic renal lesion’, ‘cystic kidney lesion’, ‘cystic renal mass’, ‘cystic kidney mass’. ‘diagnosis’ and ‘therapy’, but excluding results with the term ‘genetic’ in the article title, was carried out in Pubmed, Science Direct, Scopus, and Google Scholar databases between May and October 2022. The Boolean operators “AND” / “OR” were included between the key inclusion terms, as well as the Boolean operator “NOT” prior to the exclusion term ‘genetic’. The sequence of terms which produced the best results in Pubmed was: (CYSTIC RENAL INJURY) AND (DIAGNOSIS) AND (THERAPY) NOT GENETIC, and in ScienceDirect: “cystic renal lesion” AND diagnosis AND therapy AND NOT genetic. In this search, 555 results were obtained in Pubmed and 72 in Science Direct. The results obtained in Scopus and Google Scholar were redundant with regard to the previously described databases.
Study selection, data extraction, and quality assessment
The selected articles were filtered using the following inclusion and exclusion criteria:
- Inclusion criteria: Original articles, with case series. Patients over 18 years of age. Asymptomatic patients with incidental diagnosis of renal cyst. Suspicion of malignancy of renal cyst. Prospective or retrospective follow-up by an imaging test (ultrasound, CT or mpMRI). Published since 2012, inclusive. Published in English.
- Exclusion criteria: Clinical cases, systematic or non-systematic reviews where the series described do not appear broken down. Pediatric patients (under 18 years of age). Genetic or hereditary renal cystic diseases. Patients with symptomatic cysts or the spontaneous complications thereof. No data about follow-up imaging tests. Published before 2012. Not published in English.
After applying both the inclusion and exclusion criteria, a total of 122 articles were extracted from Pubmed and 32 articles from ScienceDirect. Paired investigators abstracted data sequentially and independently assessed the risk of bias for individual studies. Eighty articles were discarded after reading both the title and the abstract, leaving a total of 74 articles. A complete review was carried out in these studies, after which another 49 articles were rejected due to insufficient data on the diagnostic or therapeutic methods or follow-up information. In this way, 25 articles were selected for final inclusion (Fig. 1). The review of the selected articles was conducted following the methodological recommendations of PRISMA 2020 Statement [9], according to the preparation and explanation document, checklist, and flow diagram attached to this document.
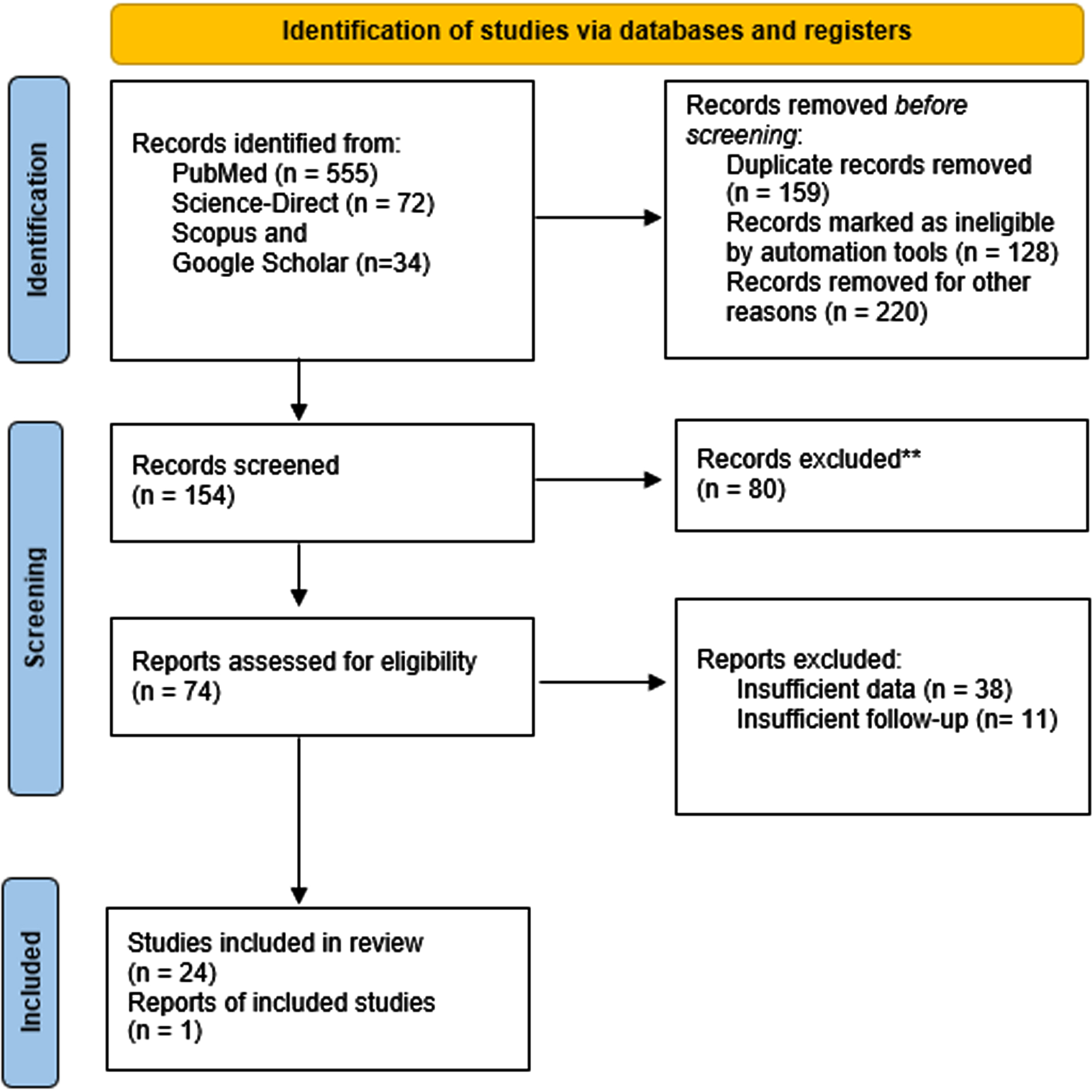
PRISMA flow diagram at three levels [9].
Data synthesis and analysis
All studies were summarized qualitatively. Since no previous studies discussed diagnostic methods and therapeutic alternatives, the reviewed articles were classified based on their objectives and results, focusing on diagnosis or treatment. The summary of the studies analyzed can be seen in Table 1 (available studies comparing diagnostic techniques of renal cystic lesions suspected of malignancy) and Table 2 (available studies comparing treatments of renal cystic lesions suspected of malignancy). These tables collect data about the authors, study type, objectives, imaging test or treatment, number of patients, type of cystic renal lesion, follow-up, and results. Of the 25 articles, 13 focus on diagnostic management with imaging tests. Of these, in five, the different ultrasound modalities were used as an alternative to conventional CT; in six the alternative of contrast enhanced mpMRI was also compared, and in three studies, predictive factors for malignancy of cystic renal lesions diagnosed by CT were defined. Eleven studies in this section were retrospective series, one was prospective, and in one, a simulated cost-effectiveness model was performed. Among the 12 remaining articles, the objectives of which were based on the evaluation of therapeutic alternatives, five focus on surgery, evaluating the different approaches, or comparing histological results in both partial and radical nephrectomy. Regarding active surveillance: one article focuses on the results of active surveillance, while another compares active surveillance versus surgery and a third versus percutaneous radiofrequency treatment. Finally, four articles assess the results of the percutaneous approach and radiofrequency ablation without a comparative group. All articles in this section are retrospective cohorts.
Available studies comparing diagnostic techniques of renal cystic lesions suspicious for malignancy
Available studies comparing treatments of renal cystic lesions suspicious for malignancy
RESULTS
Diagnostic methods and imaging tests in the finding of cystic kidney lesions (Table 1)
In the study by Markic et al. [10], the data of 307 patients who had undergone nephrectomy (partial or radical) for renal lesions visible on CT and ultrasound were retrospectively analyzed. In 6 patients, there were discrepancies between the techniques, with Bosniak II-III cystic lesions diagnosed on CT and lesions with solid poles suspicious for RCC on ultrasound. In these cases, a biopsy was performed prior to surgery, which confirmed RCC, as was later demonstrated in the nephrectomy specimen, where macroscopic areas of renal cancer were observed. The authors conclude that the two techniques can be complementary in doubtful cases prior to renal biopsy.
The study by Muhlfeld et al. [11] concludes that non-contrast mpMRI was more sensitive than ultrasound in the identification of RCC and lesions suspicious for RCC, so this appears to be useful as a secondary screening tool in patients with chronic kidney-acquired cyst disease after transplantation.
In their retrospective series, Goenka et al. [12] analyzed 107 renal lesions classified as Bosniak III on abdominal CT in 101 patients. All these lesions were resected and analyzed pathologically, obtaining 59 neoplasms and 48 benign lesions. The objective of this study was to establish a predictive model to assess the risk of renal neoplasia in Bosniak III lesions. Surgical pathological findings for the resected malignant lesions were clear cell carcinoma (29/59), papillary carcinoma (15/59), unclassified carcinoma (5/59), mixed carcinoma (4/59), and multilocular cystic RCC (6/59). Of the malignant lesions, 46 were non-aggressive, 11 were aggressive variants, and the Fuhrman grade was not available for 2 lesions. The findings for the resected benign lesions were epithelial or fibrous cyst (25/48), cystic nephroma (13/48), mixed epithelial stromal tumor (1/48), oncocytoma (1/48), and other benign tissue with or without atypical cells (8/48).
On univariate analyses, the strongest potential predictors of malignancy were African American race (P = .043), history of RCC (P = .026), coexisting Bosniak III lesions (P = .032), coexisting Bosniak IV lesions (P = .104), body mass index (BMI; P = . 078), and lesion size (P < .001). A model with lesion size (odds ratio [OR] 0.69; 95% confidence interval [CI] 0.58-0.82), history of RCC (9.02; CI 0.99-82.15), and BMI (OR 1.1; 95% CI 0.99-1.19) offered the best performance with a c-index after cross-validation of 0.719. Using an estimated probability of malignancy of > 80%, the positive predictive value of the model is 92% (CI 78% -100%). Goenka concludes that clinical risk factors offer modest but definite predictive ability for malignancy in Bosniak III lesions. In particular, a prediction model encompassing lesion size, BMI, and history of RCC seems promising. Further refinements with the possible inclusion of imaging biomarkers and validation on an independent dataset are desirable.
Nouhaud et al. [13] evaluated and compared the pathological characteristics of renal cysts Bosniak IIF, III, and IV in the light of recent histological classification. The French research network for kidney cancer UroCCR conducted a multicentre study on patients treated surgically for a renal cyst between 2007 and 2016. Independent radiological and centralized pathological reviews were performed for every patient. Pathological characteristics were compared to the Bosniak classification. Of the 216 patients included, 175 (81.0%) tumors (90.9% of Bosniak IV, 69.8% of Bosniak III) were malignant or had a low malignant potential, with 60% of clear cell renal cell carcinoma (CCRCC), 24% of papillary RCC (PRCC) and 6.9% of multilocular cystic renal tumor of low malignant potential (MCRTLMP). Malignancies were mainly of low pT stage (86.4% of pT1–2) and low ISUP grade (68.0% of 1–2). Bosniak III cysts had a lower rate of CCRCC (46.7 vs. 67.3%), a higher rate of PRCC (30 vs. 20.9%), and MCRTLMP (18.3 vs. 0.9%) compared to Bosniak IV (p < 0.001). Low malignant-potential lesions were less likely Bosniak IV, and pT3–4 stage was more frequent in Bosniak IV vs. III (15.7 vs. 3.5% ; p = 0.04). Two recurrences (1.1%) occurred, and no cancer-related death occurred during follow-up. These results confirmed that cystic renal malignancies have an excellent prognosis. Bosniak III cysts had a low malignant potential, which suggests surveillance could be an option for such lesions.
Kahn et al. [14] studied nine renal masses from eight patients (aged 54–74 years) with chronic renal insufficiency. These were evaluated with contrast-enhanced ultrasound (CEUS) and shown to be enhancing after the intravenous administration of contrast agent, of which two of them were found to be cystic lesions. All were pathologically examined following laparoscopic radical nephrectomy. Eight of the nine lesions were renal cell carcinoma (two clear cell, four papillary, two cystic). One resected mass was an unspecified benign renal lesion. Both cystic lesions with contrast enhancement in ultrasound were RCC (cystic and papillary subtypes).
Zhong et al. [15] retrospectively analyzed 35 renal cyst masses in 34 patients who underwent both mpMRI and CT examinations within six months. Twenty-four lesions (9 category III and 15 category IV on CT) received surgical treatment, 4 category IIF lesions on CT were upgraded to category III on mpMRI, and were ultimately accepted for operative resection. The remaining 7 lesions (category II– IIF on both CT and mpMRI) were followed up for at least three years. Findings on mpMRI and CT images were inconsistent in 8 (23%) lesions. Of these, 3 category II lesions on CT were classified as category IIF on mpMRI images, 4 category IIF lesions on CT were upgraded to category III on mpMRI, and 1 category III lesion was upgraded to category IV. In these lesions, mpMRI detected more increased wall/septa thickness (n = 8) and septa number (n = 3) than CT, resulting in an upgrade in classification. Based on the pathological results, 5 of category III (5/9, 56%) and all category IV (15/15, 100%) lesions on CT images were malignant. On mpMRI, 4 of category III (4/12, 33%) and all category IV (16/16, 100%) lesions were malignant. The authors concluded that renal cyst masses, especially category II to III lesions, may be over-evaluated by the Bosniak criteria based on MR findings. Therefore, combining mpMRI features with CT findings is advisable for the assessment and management of such cases of renal cystic mass.
Hoon Oh et al. [16] reviewed the records of 368 patients with renal cysts between January 2001 and December 2014; 14 patients were excluded due to interobserver variability in Bosniak classification between the radiologist and urologist. In 324 surgically excised lesions from patients (n = 312) with renal cysts, the percentages of malignancy in the different Bosniak classifications were as follows: category I, 1.0% (1 of 103); II, 3.8% (2 of 53); IIF, 17.1% (7 of 41); III, 38.0% (27 of 71); and IV, 82.1% (46 of 56). Surgical pathological findings of malignant cystic lesions included clear cell 69.9% (58 of 83), papillary 20.5% (17 of 83), and multilocular cystic renal cell 9.6% (8 of 83) carcinomas. Risk factors of malignancy in complicated renal cyst patients were not different to those published previously. Multivariate analysis identified hypertension, smoking history, and obesity as risk factors for RCCs that were statistically significant predictors of malignancy in complicated renal cysts. In the study of Bosniak III patients, the strongest potential predictors of malignancy included hypertension (p = 0.018), cystic lesion diameter (6.43±4.98 cm vs. 3.66±2.40 cm, p < 0.001), and difference of Houndsfield units (HU) (36±8.7 vs. 61±12.3, p = 0.027), whereas smoking history and obesity were not significant. Multivariate analysis identified cystic lesion diameter as the strongest independent predictor of malignancy, followed by hypertension and difference of HU.
Menezes Ferreira et al. [17] compared the ability of mpMRI and CT to discriminate between benign and malignant cystic renal lesions using the Bosniak classification. Forty two complex cysts, from 37 patients, with CT and mpMRI up to six months apart, were included. Surgery and pathology reports and follow-up of at least 24 months were used as a standard of reference. Twenty-nine lesions were classified as Bosniak I, Bosniak II, or Bosniak II-F by CT and/or mpMRI, and 13 as Bosniak III or Bosniak IV, by one of the methods. The interobserver agreement for Bosniak classification for CT was 0.87 and 0.93 for mpMRI. Fifteen lesions had higher Bosniak categories on mpMRI, including 6 where this resulted in a change in management. Only 2 lesions had a higher category on CT, with 1 resulting in change in management. The frequency of malignancy for Bosniak III was 50 % (2/4) for CT and 20% for mpMRI (1/5), as Bosniak upgrades by mpMRI resulted in surgery for benign lesions: management changed in only 7 of the 15 that were upgraded by mpMRI as compared to CT and in 1 of the 2 cases of wall calcification. Two Bosniak I and 3 Bosniak II lesions were upgraded to Bosniak II-F after mpMRI and initiated our surveillance protocol; all remained stable after more than 24-month follow-up, and 2 lesions classified as Bosniak II-F on CT were interpreted as Bosniak III lesions after mpMRI. Both were resected and showed inflammatory and hemorrhagic changes without malignancy. The lesions upgraded by CT from II to II-F (mpMRI), were downstaged to Bosniak II after a follow-up of 30 months. Category migration and management change occurred in a significant proportion of complex renal cyst cases after mpMRI assessment; probably due to its superior soft tissue and contrast resolution.
Mu et al. [18] evaluated the performance of ultrasound Bosniak classification aided by Superb microvascular imaging (SMI) in the diagnosis of cystic renal masses. SMI is a new ultrasonic technique which applies advanced clutter suppression to reflect microflow information. The sensitivity, specificity and accuracy of a conventional ultrasound and SMI combination in diagnosing renal cystic masses was evaluated by comparison with CEUS and pathology. The study included 55 patients diagnosed with solitary cystic renal mass at the Tianjin Medical University Cancer Institute and Hospital between Jan 2015 and Feb 2017. These patients received a conventional ultrasound, Color Doppler Flow image (CDFI), and SMI. Complex indeterminate Bosniak category IIf, III, IV renal cystic masses were performed CEUS after conventional ultrasound.
Of these cases, 44 received surgical resection of renal cystic masses and a final pathological diagnosis. Eleven patients did not receive surgical resection; of those, 6 cases of cystic renal mass were finally diagnosed as simple cysts after a mean follow-up of 27 months (12–36 month); CEUS was performed on 5 cases with complex cystic renal lesions in Bosniak category IIF-IV, which were then diagnosed as radiologically benign and confirmed at least 1 year after follow-up. SMI had the highest area under the curve (AUC) in diagnosing malignant masses from benign masses [AUC = 0.869(0.743–0.995)]. The sensitivity and specificity of SMI were 94.8 and 75.0%. CEUS had moderate distinguishing efficacy with a higher sensitivity of 97.4% and a relatively higher specificity of 70.6% [AUC = 0.840(0.763–0.977)]. The AUC of CDFI was the lowest, with 76.3% sensitivity and 88.2% specificity [AUC = 0.823(0.702–0.944)]. This study shows that SMI can significantly improve the detection rate of microflow in cystic septa and tiny solid papilla on septa. Due to there being few cystic septa and less blood flow, there was no significant difference between CDFI and SMI in the diagnosis of benign renal capsule lesions, usually graded at Bosniak classification I and II. For the masses with a Bosniak classification above IIF, however, there was a significant difference between CDFI and SMI with regard to the blood flow accessed in Bosniak classification. SMI can detect richer and more subtle blood flow signals, has a lower range, and more sensitivity.
Park et al. [19] evaluated the postoperative outcome of cystic RCC defined on preoperative CT. This study also sought to find the optimal cut-off for the cystic proportion in association with patient prognosis. A total of 1,315 patients who underwent surgery for a single RCC with preoperative computerized tomography were enrolled. RCC were categorized as cystic or noncystic according to a conventional cut-off (i.e., cystic proportion 75% or greater) and an optimal cut-off. Postoperative outcomes between the 2 groups were then compared. Multivariate Cox regression analysis was performed to determine the independent predictor of cancer-specific survival. Of the 1,315 lesions, 107 (8.1%) were identified as cystic RCC according to a conventional cut-off. The postoperative outcome of cystic RCC was significantly better than that of noncystic renal cell carcinoma (p < 0.001); neither metastasis nor recurrence developed after surgery in patients with cystic RCC. In association with the cancer-specific survival rate, the optimal cut-off for the cystic proportion was 45%, and 197 cases (15.0%) were accordingly defined as cystic RCC. On Cox regression analysis, a cystic proportion of 45% or greater of the RCC was an independent predictor of a favorable outcome as regards cancer-specific survival (HR 0.34, p = 0.03). The authors concluded that cystic RCC defined on preoperative CT were associated with low metastatic potential and favorable outcomes after surgery. In particular, a cystic proportion of 45% or greater was found to be an independent prognostic factor for favorable survival.
Mousessian et al. [20] studied the malignancy rate, histologic grade, and initial stage of surgically treated complex renal cysts classified as Bosniak category III or IV. A secondary objective for nonsurgical lesions was to evaluate lesion progression on follow-up examination. Cystic lesions classified as Bosniak category III or IV on CT or mpMRI from January 2008 to April 2016 were retrospectively reviewed. Surgically resected lesions, per category, were correlated with the information in pathologic reports to obtain malignancy rates. For malignant lesions, histologic grade and initial stage were also evaluated. Imaging follow-up of at least two years was used to evaluate the progression of clinically-followed lesions. Altogether, 86 lesions in 85 patients were included in the final analysis. Of the 60 surgically resected lesions (70%), 46 (77%) were malignant, and 14 (23%) were benign. Malignancy rates were 72% for Bosniak category III lesions and 86% for Bosniak category IV lesions. Most malignant cysts were early stage (pT1) with low histologic grades (89% of Bosniak III lesions and 91% of Bosniak IV lesions). Follow-up study of the surgically resected lesions did not show local recurrence, metastasis, or lymph node enlargement. Among patients with lesions managed by watchful waiting (n = 26), all lesions remained unchanged in size and complexity after at least 2-years of follow-up. Although high malignancy rates were observed for both Bosniak category III and IV lesions, results suggest that such malignant cysts are usually early-stage tumors with a low histologic grade. Lesions that underwent follow-up were found to have remained unchanged upon control examination. These findings may indicate the low aggressiveness of these lesions, supporting the idea that more conservative approaches could be used.
Sanz et al. [21] performed a prospective observational study between April 2011 and July 2014. A total of 66 patients with 67 RCCMs were enrolled (Bosniak II– IV) with 24 patients undergoing surgical removal of the RCCM. All participants were subjected to CEUS (experimental) and CT (control). A single highly-experienced observer performed all CEUS procedures. Benign lesions were defined as those exhibiting as Bosniak II– IIF, and malignant as Bosniak III– IV. Statistical analysis was conducted by measuring the consistency (kappa index and Landis-Koch scale) and validity (sensitivity, specificity, positive and negative predictive values) of the study. CEUS has a sensitivity of 100%, specificity of 81.4%, positive predictive value of 70.4%, and negative predictive value of 100%. A total of eight RCCMs were discordant, and 7 of 8 were classified as malignant by CEUS and not by CT. Of those 7 lesions classified as malignant by CEUS, 6 (6 of 7, 85.7 %) were found to be malignant in the pathological exam. The study concluded that CEUS is a very useful tool for assessing RCCM, with good results in terms of consistency and validity. It has excellent diagnostic power, with a sensitivity of 100% and a negative predictive value of 100%. Its main limitations are the experience required, special software, and being observer-dependent.
Spiesecke et al. [21] compared the health-economic aspects of the multiple imaging modalities used to monitor renal cysts; the present study evaluates the costs and outcomes of patients with Bosniak IIF and III renal cysts detected and followed-up either by contrast-enhanced CT (ceCT), contrast-enhanced mpMRI (ce-mp-MRI), or CEUS. Simulation using Markov models was implemented and performed with 10 cycles of one year each. Proportionate cohorts were allocated to Markov models by decision-tree processing-specific incidences of malignancy and levels of diagnostic performance. Costs of imaging and surgical treatment were investigated using internal data from a European university hospital. Multivariate probabilistic sensitivity analysis was performed to confirm results considering input value uncertainties. Patient outcomes were measured in quality-adjusted life years (QALY), and costs as averages per patient, including the cost of imaging and surgical treatment. Compared to the ‘gold standard’ of ceCT, ce-mp-MRI was more effective but also more expensive, with a resulting incremental cost-effectiveness ratio (ICER) > \euro 70,000 (Euro) per QALY gained. CEUS was predominant as compared to ceCT in both Bosniak IIF and III renal cysts in terms of QALYs and costs. Probabilistic sensitivity analysis confirmed these results in the majority of iterations. Both ce-mp-MRI and CEUS can be used as alternatives to ceCT in the diagnosis and follow-up of intermediately-complex cystic renal lesions without compromising effectiveness, and CEUS is also cost-effective. However, the economic results apply to a large university hospital and would need to be adjusted for smaller hospitals.
Treatment alternatives in cystic kidney lesions (Table 2)
The treatment of 61 patients with cystic kidney lesions was retrospectively analyzed in the study by Donin NM et al. [22]. These patients presented with Bosniak II [1], Bosniak IIF [3], Bosniak III [53], and Bosniak IV [4] cysts. Altogether, 19 patients began with active surveillance; following an increase in size or complexity of the cystic lesion, they underwent surgical treatment. In patients with renal cystic lesions, active follow-up was proposed until progression/change without this management, reducing the probability of cure. All of this suggests that the malignant potential of renal cystic lesions is less than that of solid renal masses.
Shigehiko K et al. [23] retrospectively studied the surgical treatment of 21 patients and found that the prognosis of patients with renal cystic lesions is significantly better than that of patients with solid renal masses, especially in multiloculated cystic lesions. Renal cystic lesion carcinoma is a subtype of renal cell cancer that can be completely cured by surgery.
Xu B et al. [24] retrospectively compared the surgical treatment by laparoscopic partial nephrectomy of 42 patients with multiloculated cystic lesions. The results were satisfactory, and there were no relapses or appearance of new lesions during follow-up. They propose laparoscopic partial nephrectomy as the gold standard for multiloculated cystic kidney lesions.
The surgical treatment of 18 patients was retrospectively analyzed in the study by Ji C et al. [25]. The results obtained after open or laparoscopic partial nephrectomy were compared, and no differences in surgical time, bleeding, ischemia time, or complications were found. Hospitalization time, however, was significantly longer in patients who underwent open partial nephrectomy, laparoscopic partial nephrectomy is therefore recommended whenever possible for patients with renal cystic lesions.
Xu B et al. [26] retrospectively evaluated the surgical treatment of 37 patients, comparing the results obtained after open or laparoscopic nephrectomy, No significant differences in terms of surgical time, ischemia time, bleeding or subsequent recurrence were found, hospitalization time and days of drainage, however, were both significantly longer in patients who underwent open nephrectomy. Laparoscopic nephrectomy is therefore recommended whenever possible, although it does involve greater technical complexity.
Weibl P et al. [27] retrospectively analyzed the treatment of 85 patients with Bosniak categories IIF and Bosniak III. Twenty seven patients with Bosniak IIF were subjected to active surveillance: 18 of them continued on surveillance while 9 of them went on to undergo surgery. Comparing the results of the Bosniak IIF and Bosniak III categories, the cystic lesions presented similar stages, grades, and subtypes of kidney cancer (mostly low-grade and low-stage). Active follow-up was recommended for BIIF lesions without implying a decrease in complete healing; instead, BIII lesions should be managed as solid renal lesions due to their higher risk of malignancy.
Bazan AA et al. [28] retrospectively evaluated the active follow-up of 82 patients with small kidney lesions (<4 cm), whether complex cystic lesions (Bosniak IIF-Bosniak IV) or solid masses. There were no significant differences in the growth rate of renal masses (solid or cystic). Only 5 patients underwent surgery due to rapid growth [3], symptomatology [1], or as a result of patient decision [1]. No local or distant progression was detected. No deaths secondary to kidney disease were observed. Active follow-up was therefore found to be a safe and reasonable option for the initial treatment of small kidney lesions, without implying any reduction in survival.
Carrafiello G et al. [29] retrospectively analyzed microwave ablation treatment (guided by CT or ultrasound (US)) in 6 patients with renal cystic lesions. In all of these, the technique was effective without local progression of the tumor lesion and the results showed a cancer-specific and overall survival of 100%. As a limitation of the study, they describe the strict selection of patients: small lesions (<4 cm) and carefully-studied patients; only those in whom the benefit was clear were selected.
Brian C et al. [30] conducted a retrospective analysis of radiofrequency ablation treatment of renal cystic lesions in 38 patients in which a percutaneous biopsy had previously confirmed the diagnosis of a malignant lesion. None had any local or distant progression. Only one patient developed a new solid renal mass during follow-up. The main complications were minor; only one developed a severe complication; the glomerular filtration rate (GFR) decreased by 2.5 ml/min/1.73m2 per patient. Radiofrequency treatment in patients with Bosniak III and Bosniak IV cystic lesions did not show any progression of local or distant tumor disease, however, this study had a follow-up of only three years, so further studies are needed to corroborate these results.
In the study by Menezes MR et al. [31], radiofrequency ablation treatment of 10 patients with complex cystic lesions Bosniak IV was retrospectively evaluated. The volume of the lesions decreased by 25% without the need for further treatment or the development of further complications.
Felker ER et al. [32] retrospectively analyzed the radiofrequency ablation treatment of 16 patients with Bosniak III and Bosniak IV cystic lesions. The treatment was initially effective in 91% of the patients, reaching 96% the second time. There was no distant dissemination of the disease, nor any complications related to the technique; a minority of patients suffered a mild decrease in renal function.
Dennis A et al. [33] retrospectively compared 286 patients treated by surgery, percutaneous ablation, or follow-up imaging. Only one Bosniak III patient treated by percutaneous ablation developed local progression and metastasis; one Bosniak IV patient developed metastatic disease and died. Complications related to the treatment mainly occurred in patients treated surgically.
DISCUSSION
Diagnostic methods and imaging tests in the finding of cystic kidney lesion
This review aims to update the current evidence about the methods of diagnosis and treatment of complex cystic kidney lesions. It includes the indexed series on this subject, most of them retrospective. There is a wide heterogeneity due to the type of lesion studied, the imaging tests used, the types of treatment in each case, and the objectives proposed in each publication. Despite these limitations, this review summarizes all the current management in this pathology.
The management of cystic renal masses entails difficulties, both for their accurate diagnosis and for their treatment. The aim is to identify masses that are susceptible to benignity or low potential for malignancy, thus avoiding overtreatment, especially in cases with impaired renal function. Cystic renal masses, despite having a high potential for malignancy in the case of Bosniak category III and IV lesions, are usually lesions in early stages and with a low histological grade [20]. The cystic percentage of the lesion is a favorable prognostic factor, especially if it exceeds 45% [19]. CeCT is the most standardized test for the characterization of these masses, and the original Bosniak classification is based on this technique. In doubtful cases, mpMRI and US or CEUS appear as complementary tests. These tests complement CT, and in the case of discrepancy between the two, a biopsy of the lesion should be considered before any active treatment [10]. Probably because of its superior soft tissue and contrast resolution, mpMRI can lead to category migration and changes in the management of complex renal cysts in a significant proportion of cases [17], resulting in potential overtreatment due to possible misinterpretation of inflammatory changes. CEUS is also a very useful tool for assessing complex renal cystic masses, with good results in terms of consistency and validity. Its main limitations are the experience required, the specialist software, and the fact that it is observer-dependent [6]. mpMRI and CEUS can be used as alternatives to contrast-enhanced CT in the diagnosis and follow-up of intermediately complex cystic renal lesions without compromising effectiveness. While CEUS is cost-effective, mpMRI is more effective but more expensive [21]. Other ultrasound techniques such as SMI appear to be equivalent or superior to Doppler ultrasound and CEUS in terms of sensitivity, specificity, and precision, but its use is not currently widespread because it is not widely reproducible [18].
Treatment alternatives in cystic kidney lesions
As we have previously commented, cystic renal lesions suggestive of malignancy seem less aggressive than those that are purely solid or have a greater solid component. Active surveillance of these lesions can be an alternative until radiological changes are observed, both in size and composition [22]. Active surveillance continues to be an alternative for Bosniak IIF. In contrast, active treatment prevails in Bosniak III or higher [23, 27], although some studies have also confirmed the safety of active surveillance in these cases combined with radiological follow-up [28]. It is useful to have a second complementary imaging test or even propose a biopsy before proceeding with active treatment [22]. Percutaneous radiofrequency treatments appear to be safe in terms of complications, with good survival rates free of local recurrence and metastasis in both Bosniak III and IV. [30–33]. This treatment appears especially to be recommended for patients with high surgical risk or in cases in which good preservation of renal function is required [30]. Partial nephrectomy is currently the gold standard in the treatment of complex cystic masses in those cases for which the size does not prevent the preservation of the renal unit. From an oncological or complications perspective, the results are similar for both open and laparoscopic approaches. Although laparoscopy adds complexity to the surgical procedure, results do seem to be superior in terms of reduction of hospital stay [25, 26].
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments.
FUNDING
The authors report no funding.
AUTHOR CONTRIBUTIONS
L.I.V. and P.A.L. contributed equally as first authors in conception, performance of work, interpretation of data and writing the article.
J.G.R. contributed in conception, interpretation of data and writing the article.
I.P.S., D.E., A.S.P., J.H.G., L.F.M., E.G.R., J.M.S. contributed in the conception of this article.
All authors had access to the data prior to article submission.
CONFLICT OF INTEREST
L.I.V., P.A.L., J.G.R., I.P.S., D.E., A.S.P., J.H.G., L.F.M., E.G.R. and J.M.S. have no conflicts of interest to report.