
Abstract
BACKGROUND:
Emerging early intervention vocational rehabilitation (EIVR) services aim to improve employment outcomes after SCI. Beyond employment, EIVR services present an opportunity to support psychological resources, potentially promoting coping and adjustment. The construct of psychological empowerment represents several such resources, including hope, self-efficacy, and motivation.
OBJECTIVE:
To analyse the extant literature on employment after SCI published since 2006, to synthesise the support for and usefulness of the psychological constructs that underpin empowerment in the return to work process, particularly as they pertain to the early phases of rehabilitation.
METHODS:
A quantitative approach to systematic review, combined with a narrative synthesis of the literature.
RESULTS:
Hope, self-efficacy, and motivation were found to be related to RTW after SCI. Research gaps were identified, particularly relating to studies with newly-injured participants. The findings were contextualised within an empowerment framework.
CONCLUSIONS:
An empowerment model of EIVR could serve to both promote employment outcomes and support psychological wellbeing during early recovery from SCI. Further research is needed to develop this model, establish its use in practice, and explore the benefits of EIVR for a person’s psychological wellbeing.
Keywords
Introduction and background
Spinal cord injuries (SCI) are catastrophic events that can interrupt every domain in a person’s life. Career trajectories are often disrupted significantly, with long term employment rates of approximately 30–40% and return to work (RTW) occurring an average of five years after the initial injury (Bloom et al., 2018; Krause et al., 2010). In response to these low rates of employment, emerging vocational rehabilitation (VR) programs introduce VR during primary rehabilitation. The aim of these services is twofold: to enhance employment outcomes in the long-term, and to inspire hope that working, and therefore “a normal life”, is possible after SCI (Ramakrishnan et al., 2016). Questions remain, however, about the effectiveness of such services during the early stages of recovery, given the significant physical rehabilitation and psychosocial adjustment that the person must undergo.
Ville and Winance (2006) suggest that a period of recovery must be undertaken in order to maximise the person’s capacity to “appropriate”, or self-direct, their career trajectory after SCI. Evidence suggests, however, that this adjustment period is shorter than previously thought, with participants reporting readiness to make career decisions within a month of injury (Fadyl & McPherson, 2010). Incorporating strategies to support psychological resources in these early stages could work to bridge these ideas –VR could contribute to adjustment and the gaining of independence rather than burdening the client during the early rehabilitation phase, and ultimately enhance the person’s capacity for appropriation of their career trajectory. The psychological empowerment construct encapsulates many such resources. Although vocational rehabilitation systems may be complex and disempowering, and environments inaccessible, the psychological processes which underpin empowerment may be reinforced in the VR context.
Empowerment and vocational rehabilitation
Empowerment is conceptualised in a number of ways across various disciplines. Broadly understood as the process by which a person gains control over their life (Rappaport, 1995), empowerment is also conceptualised as a motivational state (Thomas & Velthouse, 1990), a state of increased capacity (Staples, 1990), and a precursor to self-determination (Fawcett et al., 1995). These different facets of empowerment have been applied in the health and human services, where empowerment frameworks are used to promote self-direction of care (Anderson & Funnell, 2010) and facilitate health behaviour change (Woodall et al., 2010). These conceptualisations of empowerment seem well-suited to vocational rehabilitation, wherein a goal is restoring self-determination. This is particularly the case following spinal cord injury, where one’s opportunities for self-determination may be diminished.
Evidence suggests that psychological empowerment is beneficial to a person’s wellbeing, and to improved mental health (Baba et al., 2017). For people with SCI specifically, adjustment to the injury can be a time during which coping skills and resilience are challenged. Despite this, relatively few interventions have been identified that aim to strengthen psychological resources after SCI (Peter et al., 2012). Psychological empowerment encapsulates many such resources (Zimmerman & Warchausky, 1998), making it a useful framework for reinforcing psychological wellbeing after SCI. Given that the goals of VR align with the conceptualisations of empowerment discussed above, EIVR is potentially well-positioned to fill this service gap and support psychological resources during adjustment to SCI.
Empowerment theory
Empowerment within the vocational rehabilitation space may be understood as the process by which a person gains control over their life, or over the aspects of their life that are important to them. Although empowerment is conceptualised and operationalised in a variety of ways according to the population under investigation, there are some common components, including an internal psychological component and an external contextual/environmental component.
Zimmerman’s (1990) conceptualisation of psychological empowerment identified three facets; intrapersonal processes such as self-efficacy and motivation to control; interactional factors including the environment; and a behavioural component referring to the person’s actions taken on the journey to becoming ‘empowered’, such as participation in organisations. Building upon this theory, Fawcett et al.’s (1994) contextual-behavioural theory of empowerment proposed two dimensions – the person and the environment – with the overall level of empowerment being a function of these two parts. Personal variables include competence, knowledge, skills, experiences and psychological/physical capacity. Environmental factors are said to both promote and limit empowerment, through the provision of resources and the presentation of barriers respectively. A rehabilitation-specific model proposed by Kosciulek (2001) also posited two underlying components: internal/psychological factors such as sense of control, competence and future orientation; and situational/social aspects like work skills, interpersonal skills, and “savvy”.
Within vocational rehabilitation specifically, Breeding (2008) proposed an empowerment framework for rehabilitation counselling, identifying self-efficacy, locus of control and outcome expectations as major underpinning processes. These factors, particularly self-efficacy and outcome expectations, are malleable in the VR context through the raising of self-knowledge, facilitation of mastery experiences, and the provision of information (Breeding, 2008).
Interventions at the environmental/contextual level may include advocacy, the provision of information, and the removal of physical barriers (Fawcett et al, 1994). However, the changes required to promote empowerment at the societal level are rarely achievable within individual VR. The internal/psychological components, nevertheless, may be supported within the VR context generally, and within early intervention VR after SCI specifically. According to the aforementioned theories, these empowerment processes may include self-efficacy, future orientation, and personality factors such as locus of control.
Motivation is closely tied to conceptualisations of empowerment with some researchers suggesting that empowerment is itself a motivational state (Thomas & Velthouse, 1990). The relationship between empowerment and motivation has made empowerment prevalent in the field of organisational psychology and human resources, which have found links between empowerment and work engagement (Spreitzer, 1995). Brooks and Young (2011) highlighted the overlap between the two processes in the educational context, finding a strong positive correlation between learner empowerment and intrinsic motivation, and a strong negative correlation with extrinsic motivation. Given these links with empowerment and the well-documented impact of motivation within VR, motivation was also incorporated as a psychological process of interest in this review.
Underpinning processes and SCI motivation
Motivation has been shown to be related to employment outcomes across a range of domains, including for the chronically ill (Berglind & Gerner, 2002), people with schizophrenia (Saperstein et al., 2011), and vocational rehabilitation (VR) service recipients (Iwanaga et al., 2019). Motivation is also associated with enhanced rehabilitation outcomes after SCI, including increased physical activity (Kerstin et al., 2006) and better pain self-management (Molton et al., 2008). Pain, fatigue, secondary health conditions and depression may diminish motivation after SCI (Hammell, 2010; Hammell et al., 2009), subsequently diminishing engagement with the rehabilitation plan and negatively impacting outcomes.
Self-efficacy
Self-efficacy is an important indicator of whether a person will attempt a certain behaviour, making it particularly relevant within the vocational rehabilitation context that relies heavily upon a person’s impetus to engage with the rehabilitation plan. This sense of self-belief may be diminished following SCI due to the subsequent loss of functional independence (Craig et al., 2015; Fadyl & McPherson, 2010). Self-efficacy is associated with a range of positive outcome indicators after SCI, including quality of life (Hampton, 2000), subjective wellbeing (Hampton, 2004), social participation (Craig et al., 2015), and the prevention of secondary health conditions (Munce et al., 2016; Spungen et al., 2009).
Hope
Positive appraisals of the future are also associated with positive outcomes after SCI, with hope having the strongest evidence base. High levels of hope are said to be integral to recovery from both acute and chronic illnesses and injuries (Lohne, 2001), promote coping and psychosocial adjustment after SCI (Dorsett, 2010; Nunnerley et al., 2013), and support psychological health and subjective wellbeing during re-integration into the community (Brazeau & Davis, 2018). Hope is also associated with increased community participation after SCI (Blake et al., 2018). The related concept optimism has similar effects, promoting life satisfaction after SCI (Byra, 2016), protecting against despair and promoting psychological wellbeing (Geard et al., 2018), and supporting functional health status in the long term (Vassend et al., 2011). These positive benefits, and the association of hope with participation, suggest that hope may play and an integral role in employment outcomes after SCI.
This review
Previous research has largely focused on determinants of RTW after SCI, including demographic variables like age, education or time since injury (Anderson et al., 2007; Ottomanelli & Lind, 2009; Trenaman et al., 2015; Yasuda et al., 2002), and contextual variables such as employment history (Ottomanelli & Lind, 2009) or available vocational rehabilitation interventions (Roels et al., 2016; Trenaman et al., 2014). Taken as a whole, prior research reflects the preponderance of demographic factors in the literature base, and the clear need to develop and target vocational service provision to this population, while overlooking the importance of the individual’s psychological resources in the RTW process.
However, a meta-analysis was undertaken by Kent and Dorstyn (2014) with the aim of investigating differences in psychological variables between employed and unemployed groups. The best support was found for psychological wellbeing (anxiety or depression), quality of life, and life satisfaction, with a variety of individual factors such as self-efficacy and adjustment having weaker or inconsistent associations with employment after SCI. However, another systematic review investigating the role of psychological resources in the adjustment process found that self-efficacy and self-esteem were most consistently linked with adjustment outcomes after SCI (Peter et al., 2012). Peter and colleagues noted that these associations were rarely extended to key rehabilitation outcomes including participation, of which employment is an important part, potentially explaining the lack of consistent linkage between self-efficacy, adjustment, and SCI identified by Kent and Dorstyn (2014). Given the stringent inclusion criteria necessary for meta-analysis, this review method may overlook qualitative studies and potentially exclude research without standardised measures. Although these exclusions ensure rigorous analysis and highly reliable conclusions, they are potentially less suitable in identifying evidence in the emerging field of EIVR post-SCI, and may exclude emerging factors that could promote self-determination and therefore assist in the RTW process after SCI.
Aims
Much of the existing research has examined employment outcomes for participants often many years post injury. Research has identified a gap in knowledge pertaining to the employment situation of people with newly acquired SCI. Vocational rehabilitation offered soon after injury represents an opportunity to preserve pre-injury jobs, which is said to prevent the loss of pre-injury skills and preserve the bond between the person and their employer, maintaining long-term career development across the lifespan (Bloom et al., 2017). There is a corresponding lack of research about the specific psychological or intrinsic constructs that may have relevance when working with newly injured individuals. As indicated above, research investigating facilitators and barriers to RTW after SCI has historically focused on physical or demographic characteristics such as functional independence or time since injury, with less research devoted to investigating the impact of psychological constructs specifically. Therefore the current review aims to explore the literature about employment after SCI to summarise the support for the psychological processes which underpin empowerment relevant to employment, particularly as they relate to newly-acquired injuries.
Methods
Search strategy
The literature search was carried out between March 2016 and October 2019. Firstly, research publications related to employment following SCI were identified using the electronic databases ProQuest, CINAHL, Web of Science and Google Scholar. Keywords for the search were ‘spinal cord injury’ or ‘spinal injury’ in combination with the following terms; ‘vocational rehabilitation’, ‘occupational rehabilitation’, ‘employment’, ‘rehabilitation counselling’, ‘job’, ‘resilience’, ‘optimism’, ‘participation’, ‘motivation’, ‘hope’, ‘self-efficacy’, ‘empowerment’, ‘self-direction’ and variations thereof. Additional papers were identified from the reference lists of papers found in the database search.
Inclusion and exclusion criteria
The following inclusion criteria were applied for inclusion in the review: Study investigated variables identified as being relevant to employment after SCI. Study was original research; reviews were excluded. Participants were between the ages of 18 and 65 years, with traumatic SCI. If a mixture of traumatic and non-traumatic SCI, or a mixture of SCI and other similar conditions, SCI-related data must be differentiated. Study published between 2006 and 2019 inclusive. Employment outcome (such as; employment rate, hours worked, satisfaction, time taken to RTW, and vocational interests) assessed as either a predictor or outcome measure. English language publications.
Articles published prior to 2006 were excluded on the basis that rehabilitation, compensation environments, and the labour market itself have undergone significant changes since the early 2000 s such as ongoing decline in fulltime employment rates, increase in precarious work, and the rise of the ‘gig economy’ (Churchill et al., 2019). These factors potentially render research published before 2006 less relevant to the current labour market.
Quantitative synthesis
The review formed part of a broader systematic review, the detailed methodology is described elsewhere (Bloom et al., 2018). The systematic review method used was a quantitative approach outlined by Pickering and Byrne (2014). This method has been widely adopted across disciplines and yields reproducible and reliable reviews (Pickering & Byrne, 2014). The method minimises bias through systematic and transparent identification, screening and database entry of the selected studies. It also allows for tabulating of the studies to identify the amount of support for a concept or intervention in situations that preclude meta-analysis. In accordance with the method, a Microsoft Excel database was developed to record details including: author(s), year of publication, research design and method, results, and any limitations identified. In addition, each paper was also classified based on whether internal states or traits, such as optimism or personality factors, were considered in relation to employment outcomes. The intrinsic predictors of employment recorded for each paper included mental health conditions; resilience; hope; motivation; personality factors; optimism; and ‘other’, which included predictors that did not fit into the other broad categories. It was also noted whether these were reported to impact on employment outcomes, or on the vocational rehabilitation process itself.
Selection and screening
Screening of titles and abstracts was completed by the first author. Studies that appeared to fit the inclusion criteria were read in full and included or discarded based on the inclusion criteria. Studies that were debatable in fulfilling the inclusion criteria were determined through discussion with the authors and included through unanimous agreement.
Quality appraisal
Studies were appraised using the Mixed Methods Appraisal Tool (MMAT) designed for systematic reviews which include studies with a variety of designs and methods (Pluye et al., 2011). The MMAT was chosen for its ability to deal with qualitative, quantitative and mixed-methods designs, as well as its reliability and its applicability to complex, context-dependent situations like employment after SCI (Pluye et al., 2011). The MMAT includes criteria each for qualitative and quantitative studies, and additional criteria for mixed-method studies. Scores are calculated by tabulating the percentage of criteria met. Efforts were made to obtain supplementary reports and publications to minimise the risk of underestimating the quality of the studies reviewed.
Analysis and synthesis
Themes were sorted according to the major domain assessed; work-related concepts, hope/optimism, perceptions of own resources/self-efficacy, and perceptions of supports. Studies that reflected more than one major domain were analysed within each relevant category, such that studies that investigated both future orientation and perceptions of supports were analysed under both of these categories. Although this was intended to maximise the amount of information gathered, there was a significant disadvantage to this approach. Substantial methodological heterogeneity was evident in the extracted studies, and combined with the re-use of data in subsequent publications, precluded a large amount of quantitative analysis. Thus, where appropriate, a narrative approach to synthesis was used.
Results
Studies included
The review formed a part of a larger, more comprehensive review of employment after SCI, for which the initial search identified 614 articles for potential review after duplicates were removed. Initial screening of titles and abstracts excluded another 302 articles based on the exclusion criteria. A full-text review of the remaining articles identified a further 185 articles for exclusion, leaving a final set for the broader review of 117 studies. Of these, a final set of 33 studies were identified that explored intrinsic psychological factors related to empowerment and employment after SCI. Figure 1 shows a PRISMA diagram detailing the extraction and screening process.
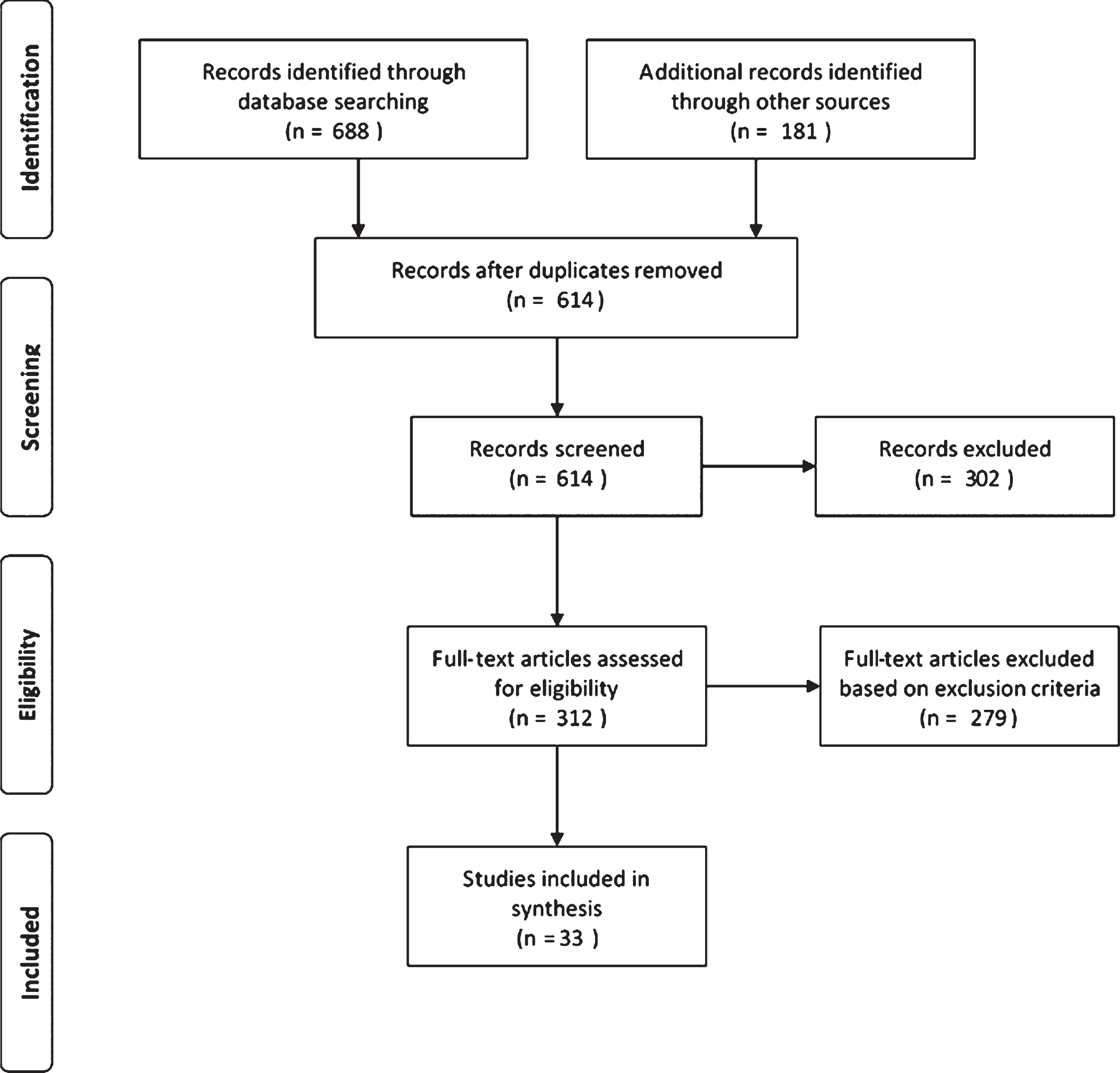
PRISMA Flowchart describing the literature search and screening process.
Considering the literature as a whole, there was a slight upwards trend in the number of studies that investigated intrinsic concepts in each year from 2006 to 2019, and when considered as a proportion of the total number of studies extracted it appears that the relevance of intrinsic constructs to employment following SCI has increased in the previous five years.
Of the 33 studies included, 16 (50%) met all of the major criteria (and rated 100%) on the MMAT tool, indicating a study without prominent sources of bias. A further 15 studies scored 75%, and two studies scored 50%. The most common sources of bias were sampling procedures, particularly convenience sampling, and low response rates.
Study designs
Cross-sectional research was dominant, with 24 (70%) studies adopting such designs. Ten studies (30%) adopted a longitudinal design. Twenty-four studies (73%) collected quantitative data, followed by qualitative (15%), and mixed data (12%).
Motivation
Eight (24%) studies investigated the impact of intrinsic drive on employment after SCI. Motivation was unanimously associated with RTW in both cross-sectional and longitudinal research, with studies indicating that intrinsic energy directed towards RTW goals facilitates employment. Seven studies conceptualised this as motivation, with one study operationalising this concept as ‘RTW intention’ (Kennedy & Hasson, 2016). Factors said to enhance motivation to RTW were positive relationships with rehabilitation professionals and family members (Wilbanks & Ivankova, 2015); valuing work (Middleton et al., 2015); a higher level of endorsement of gender norms (Burns et al., 2010); and desiring normalcy (Hay-Smith et al., 2013; Wilbanks & Ivankova, 2015). Financial motivation and intrinsic work ethic were also notable factors (Wilbanks & Ivankova, 2015). Two studies identified a relationship between motivation and RTW such that high motivation was a facilitator and low motivation a barrier to employment (Cotner et al., 2015; Hansen et al., 2007).
Average times since injury within studies investigating motivation ranged from newer injuries (less than 12 months) (Kennedy & Hasson, 2016; Middleton et al., 2015) up to 20 + years since injury (Krause & Reed, 2011; Wilbanks & Ivankova, 2015), suggesting that motivation may remain an important factor beyond the initial rehabilitation phases.
Self-efficacy, self-perceptions and internal resources
Constructs pertaining to a person’s perceived control over their situation as it related to their RTW were investigated in eight (24%) studies. This was usually conceptualised as ‘self-efficacy’, or a person’s confidence in their ability to perform a task or exert control over a given situation. The studies found mixed support for its relationship to returning to work following SCI. Three studies reported that increased self-efficacy was indicative of increased employment rates (Craig et al., 2015; Miller, 2009; Umucu et al., 2016). Within the VR context, Middleton et al. (2015) included self-efficacy building efforts within an early intervention VR program, emphasising its utility in this setting. Qualitative research within a similar injury population concluded that SCI can result in a devastating loss of self-confidence, which may be ameliorated through early intervention self-efficacy and self-confidence raising efforts (Fadyl & McPherson, 2010).
In operationalising the perceptions of self, Smedema et al. (2014) investigated the impact of core self-evaluations (CSE), one component of which is generalised self-efficacy, finding that high CSE is related to employment following SCI via an increase in hope. Krause and Broderick (2006) also found that a high internal locus of control, or a high level of confidence in one’s ability to impact outcomes, was associated with increased rate of RTW.
Hope or future orientation
Future orientation was acknowledged in the literature as being of potential importance to returning to work after SCI; six (18%) studies investigated this area, finding empirical support for its relationship to RTW after SCI. Evidence supported hope as being related to working after SCI (Hay-Smith et al., 2013; Krause & Pickelsimer, 2008; Smedema et al., 2014). Optimism (Glaessel et al., 2012; Middleton et al., 2015) positive appraisals (Middleton et al., 2015), and interest in the future (Glaessel et al., 2012) were also perceived to be predictors of positive vocational outcomes. These investigations of hope and related variables were undertaken mostly with participants at least 10 years post injury, highlighting a gap in the research relating to how hope operates within the new injury space.
Other measures
Two studies (6%) observed a link between perceptions about SCI and/or disabilities and employment after SCI. Fadyl and McPherson (2010) highlighted that people with SCI often have preconceived notions of what a person with SCI can do, and these notions can influence employment decisions. Quantitatively, Kennedy et al. (2010) found that a negative perception of disability is associated with reduced participation and life satisfaction after SCI, potentially due to these participants’ belief that the injury was more unmanageable than others with a more positive perception of disability.
Discussion
Synthesising the various theories of empowerment suggests that psychological empowerment is underpinned by three psychological variables: self-efficacy, hope, and motivation. These variables are associated with a broad range of outcomes post-SCI, and are said to promote psychological wellbeing and coping after injury. The current review found that these three factors are also linked to improved employment outcomes, suggesting that they are useful factors to target in VR for this population. These results, combined with the protective effects of these variables, indicate that an empowerment framework of EIVR may be useful in promoting employment outcomes and strengthening psychological resources for people with newly acquired injuries.
Motivation
Some theories of empowerment suggest that motivation and psychological empowerment are linked, such that empowerment is an intrinsically motivated state (Spreizter, 1995; Thomas & Velthouse, 1990). The current review found that studies about employment after SCI tend to measure motivation broadly, without differentiation between intrinsic and extrinsic motivation. It seems that all motivation is useful in the VR space, insofar as the goal is merely obtaining employment. Evidence suggests that extrinsic motivation, such as financial need or insurance-mandated VR, undermines employment outcomes in the long-term, diminishing job satisfaction and increasing turnover intentions (Kuvaas et al., 2017). This is an important consideration for VR services in promoting sustainable outcomes, and therefore more research on the impact of extrinsic versus intrinsic motivation within VR is recommended.
Although intrinsic motivation was not directly investigated, factors that might serve as intrinsic motivators have been identified in prior reviews (Bloom et al., 2019). Intrinsically motivated tasks are driven by personal rewards, such as a sense of satisfaction or enjoyment derived from the task (Deci & Ryan, 2000). Therefore, the valuing or salience of work is potentially an intrinsically motivating factor when considering RTW after SCI. Research suggests that the importance, value, or primacy of work is related to employment post-SCI (Burns et al., 2010; Krause & Reed, 2011; Marti et al., 2012). Qualitatively, personal beliefs about the value of working were said to come into play when making career decisions soon after injury (Fadyl & McPherson, 2010). These factors are said to be components of a person’s occupational bond, or their connection to the world of work (Bloom et al., 2019). Although evidence supporting the conceptualisation of the occupational bond is limited, this construct presents useful targets for intervention when considering intrinsic motivation after SCI.
Self-efficacy
Relating specifically to the new injury group, research highlighted that self-efficacy and confidence potentially decrease following injury, commensurate with the loss of physical function (Fadyl & McPherson, 2010). Self-efficacy was mostly supported as a facilitator of participation and employment for this group (Craig et al., 2015), with one VR trial including self-efficacy raising efforts in their program (Middleton et al., 2015). Going beyond the new injury group, there was mixed support for generalised self-efficacy, with two studies finding no significant relationship between self-efficacy and employment (Ferdiana et al., 2014; Murphy et al., 2011). Ferdiana et al. (2014) suggested RTW self-efficacy may be a more appropriate construct than generalised self-efficacy due to its stronger predictive relationship with RTW amongst people with musculoskeletal disorders. Viewing this process through an empowerment lens, the presence or absence of contextual factors may be moderating the relationship between self-efficacy and employment outcomes, such that self-efficacy promotes outcomes when there is an ‘empowering’ environment.
Hope
There were comparatively few studies on the role of hope, or other constructs relating to the role of positive expectancy, in RTW after SCI, however the results of these few studies are promising. Hope was supported as being related to employment for injury groups spanning one to 10 + years since injury (Hay-Smith et al., 2013; Krause & Pickelsimer, 2008; Smedema et al., 2014), suggesting that its importance does not diminish over time. Although no studies examined this construct within the new injury group, researchers proposed that hope or ‘interest in the future’ enhances motivation in the VR program (Glaessel et al., 2012; Middleton et al., 2015). These findings align with the empowerment perspective, which suggests that positive expectations underpin the motivated state of being “empowered” (Kosciulek, 2001). Beyond employment or VR, research suggests that hope is protective, promoting coping and adjustment and preventing despondency after SCI (Dorsett, 2010; Glaessel et al., 2012; Lohne, 2008). These findings highlight the benefits of reinforcing hope after SCI, and support the integration of an empowerment framework of VR for this population, of which hope is a key component.
Empowerment and EIVR
Although the review demonstrated support for psychological empowerment for people with SCI, there was a clear gap in the literature about people with newly acquired SCI (within the first year of injury). Psychological empowerment is potentially more relevant during this early time when conceptualisations of the self and hope for the future are challenged by this significant life event. As increased self-efficacy and hopefulness are associated with adjustment after SCI (Craig et al., 2009; Dorsett et al., 2017), there is an opportunity for EIVR to reinforce these psychological resources during this time and potentially support psychological wellbeing during early rehabilitation. Further research could explore psychological resources in the new injury phase and establish the role of EIVR in strengthening or reinforcing these resources.
Implications for research
Mixed support was found for some variables, particularly self-efficacy or self-appraisal. This is potentially due to the highly contextualised nature of employment – environmental accessibility, service availability and discrimination can impact on RTW after SCI (Anderson et al., 2007). Empowerment theory suggests that there is a contextual/environmental component of empowerment, whereby inaccessible environments, prejudice and challenging service arrangements can be disempowering, regardless of a person’s psychological resources (Fawcett, 1994). VR traditionally aims to mitigate the impact of these factors through job matching, advocacy, information provision and job accommodations. Combined with the results of this review, there is clear potential for the utility of an empowerment model of vocational rehabilitation after SCI which takes into account both individual and environmental factors, and more research is needed to develop this model.
Supporting self-efficacy and hopefulness within EIVR could potentially augment the broader rehabilitation program. From an empowerment perspective, promoting hope and self-efficacy is theoretically motivating, potentially enhancing participants’ engagement with the rehabilitation program. These factors are also protective psychological resources that potentially promote coping and adjustment, further supporting recovery. Despite these benefits, there are relatively few interventions targeted at strengthening psychological resources for this population (Peter et al., 2012). Emerging evidence suggests that EIVR contributes to this function, promoting hope and self-efficacy by focusing on possibilities and strengths rather than losses (Ramakrishnan et al., 2016). Further research is needed to confirm this function of EIVR, investigate the impact of EIVR on coping and adjustment after SCI, and explore the impact of EIVR on the broader rehabilitation program.
Finally, it seemed common in this review for the research about employment after SCI to incorporate single psychological variables such as self-efficacy, motivation, or appraisals, to control for individual differences. Incorporating psychological empowerment in future studies could go further in controlling for psychological differences, given that such a variable would ostensibly measure a range of dimensions of the self.
Implications for practice
The evidence for any individual psychological construct is insufficient to recommend their inclusion within early intervention VR programs following spinal cord injury. Taken as a whole, however, the literature base clearly supports the inclusion of empowerment-related variables within the VR space. As some of these constructs are already recognised in established VR practices more generally, their inclusion in VR programs following recent SCI may be supported while the development of a research basis establishing the empowerment model is ongoing. Given the impact of SCI, the variations in how these injuries affect functioning, and the unique psychological profiles of each individual, it is vitally important that interventions are delivered in individualised, person-centred ways, regardless of the constructs being utilised or measured.
Bolstering self-efficacy
Self-efficacy may be supported by the rehabilitation counsellor by including self-efficacy raising interventions within early intervention VR programs for this group. Adapting Bandura’s model of self-efficacy, Betz (2007) proposes four essential domains to improving career self-efficacy: facilitating successful accomplishments (mastery experiences); use of role models for vicarious learning; social persuasion and encouragement; and anxiety management techniques. These may be incorporated into an early intervention VR program from the initial interview, during which the vocational assessment allows for the discussion and revisiting of previous professional accomplishments and to identify goals for future mastery experiences (Sullivan & Mahalik, 2000). Social persuasion and support can be gained from the rehabilitation counsellor and peer support, which would also assist with role modelling (vicarious learning). Finally, anxiety management techniques such as role playing job interviews and countering negative self-talk may be built into the VR program (Sullivan & Mahalik, 2000).
Other factors identified that may impact a person’s self-efficacy following SCI, include their perceptions of SCI and disability in general (Fadyl & McPherson, 2010; Kennedy et al., 2010). Participants with a more negative appraisal of disability are potentially more likely to perceive their situation as unmanageable (Kennedy et al., 2010), thus decreasing their self-efficacy. Conversely, participants’ confidence is increased by peer role modelling, which impacts their perception of the capabilities of people with SCI (Fadyl & McPherson, 2010). These findings highlight the value of peer support and education about the injury, particularly as it relates to the employment space.
Fostering hope
One of the features of early intervention VR is that it is hope inspiring; participants of such programs have reported that enshrining RTW as a possibility early in rehabilitation gave them hope that recovery was possible (Ramakrishnan et al., 2016). The early provision of information, linking to resources, and discussion of possibilities serves to reinforce hopefulness in this context (Ramakrishnan et al., 2016). Snyder’s Hope theory (2000) holds that hope is comprised of the ability to devise pathways towards one’s goals (pathways thinking) and the ability to generate energy towards achieving those goals (agency thinking). Thus, establishing meaningful vocational goals and devising clear pathways towards those goals would theoretically enhance a person’s hope post-SCI (Dorsett et al., 2017). Hope may also be supported by holistically considering the person’s situation to identify barriers to hopefulness, which might include chronic pain, financial hardship or lack of access to services (Dorsett et al., 2017). Strategising and advocating to remove or minimise these barriers may also support hope in the VR context.
Limitations and challenges to synthesis
Although this review extends previous reviews in the area of employment after SCI, there remain some limitations to the findings. Firstly, the heterogeneity of the studies reviewed limited their aggregated ability to support the constructs examined. The studies were also limited to English language journals accessible through the author’s institutional library database subscription. There were some challenges to quantitative synthesis in this review. Firstly, there were issues with the identification and screening of studies that utilised a ‘new injury’ sample. Reporting of time since injury was often absent or unclear, with some studies reporting both ‘average age at injury’ and ‘average age at study’ without specifying time since injury, or indicating participants were ‘post discharge’. Participants with newly acquired injuries were often aggregated into larger samples ranging one year to decades since injury, potentially disguising the unique needs of this population.
There was significant geographical and demographic heterogeneity present in the studies reviewed; the eight studies investigating the early injury group represented six different countries. These countries potentially have differing political and compensation environments, different cultural attitudes towards disability and working, different social welfare schemes, and different job markets. Although not all of these factors are different country to country, they impact the extent to which conclusions can be generalised to other contexts, as they may influence a person’s internal psychology in unforeseen ways. For example, cultural variations impact the value placed on work (Schwartz, 1999), general self-efficacy (Scholz et al., 2002), the tendency towards optimism (Chang, 1996), and the perceived helpfulness of social support (Taylor et al., 2007).
In addition to the geographical and sampling variability, there were also some methodological inconsistencies, namely in the operationalising of employment success, and in the measurement of the constructs themselves. The majority of studies in the overall review utilised employment rate as the main measure of employment success, usually dichotomising this as ‘employed’ versus ‘unemployed’. It was also reasonably common to group participants into these categories based on a threshold of paid hours worked per week, and to differentiate between full-time and part-time work. There were similar subtle differences in the measures of the constructs themselves; one construct could be measured with many different tools. These methodological variations impacted the extent to which the literature could be aggregated, and the reliability of the conclusions drawn about each construct.
Conclusion
Overall, the results of the review indicated that an empowerment VR framework could be useful in early intervention VR following SCI, with the processes underpinning the psychological component of empowerment being empirically supported with this population. More research could establish a comprehensive empowerment model incorporating both intrinsic/individual and extrinsic/environmental components. This could mitigate any potential pitfalls of early intervention VR and augment the broader rehabilitation program by supporting coping and adjustment to the injury while also working towards vocational goals.
Conflict of interest
The authors declare that they have no conflict of interest.