
Abstract
There is compelling evidence that exercise must be part of main line therapy for people with Parkinson’s disease. In this viewpoint, we outline the four key components of exercise: aerobic exercise, resistance exercise, flexibility exercise, and neuromotor exercises (posture, gait, balance, and agility) that can improve both motor and non-motor symptoms of the disease and, in the case of aerobic exercise, may delay the disease. We outline guidelines on how to change and optimize the exercise prescription at different stages of the disease.
Mounting evidence from the past three decades clearly demonstrates the benefits of exercise for people with Parkinson’s disease (PwPD) [1–4]. Exercise improves the motor and non-motor features of Parkinson’s disease (PD) [2], and may slow disease progression [5–7]. Yet, the best combination of exercises and optimum doses are still not routinely achieved by PwPD in their everyday life. In this viewpoint, we lay out: 1) the evidence supporting the exercise prescription for PwPD, 2) the current guidelines for the exercise prescription for PwPD and how to customize it for different disease stages, 3) practical tips for implementation, 4) medical clearance for exercise, and 5) exercise considerations specific to PD. We would like to stress from the outset that there is a commonly held misnomer that it does not matter what type of exercise a PwPD does, and that they are therefore free to choose whatever they would like. We will show that there are clear guidelines to adhere to if the goal is to optimize the benefit from exercise.
EVIDENCE SUPPORTING GUIDELINES FOR THE EXERCISE PRESCRIPTION FOR PD
PwPD should essentially follow the same exercise guidelines as those for their age-matched peers. As such, the exercise prescription for PwPD is very similar to the guidelines provided by the World Health Organization [8], and many other health agencies responsible for public health and diseases around the world. Of course, in PD, the case for exercise and activity as first-line therapy is even more compelling than in healthy individuals because PD is a relentlessly, and at times, insidiously, progressive disease.
Aerobic exercise
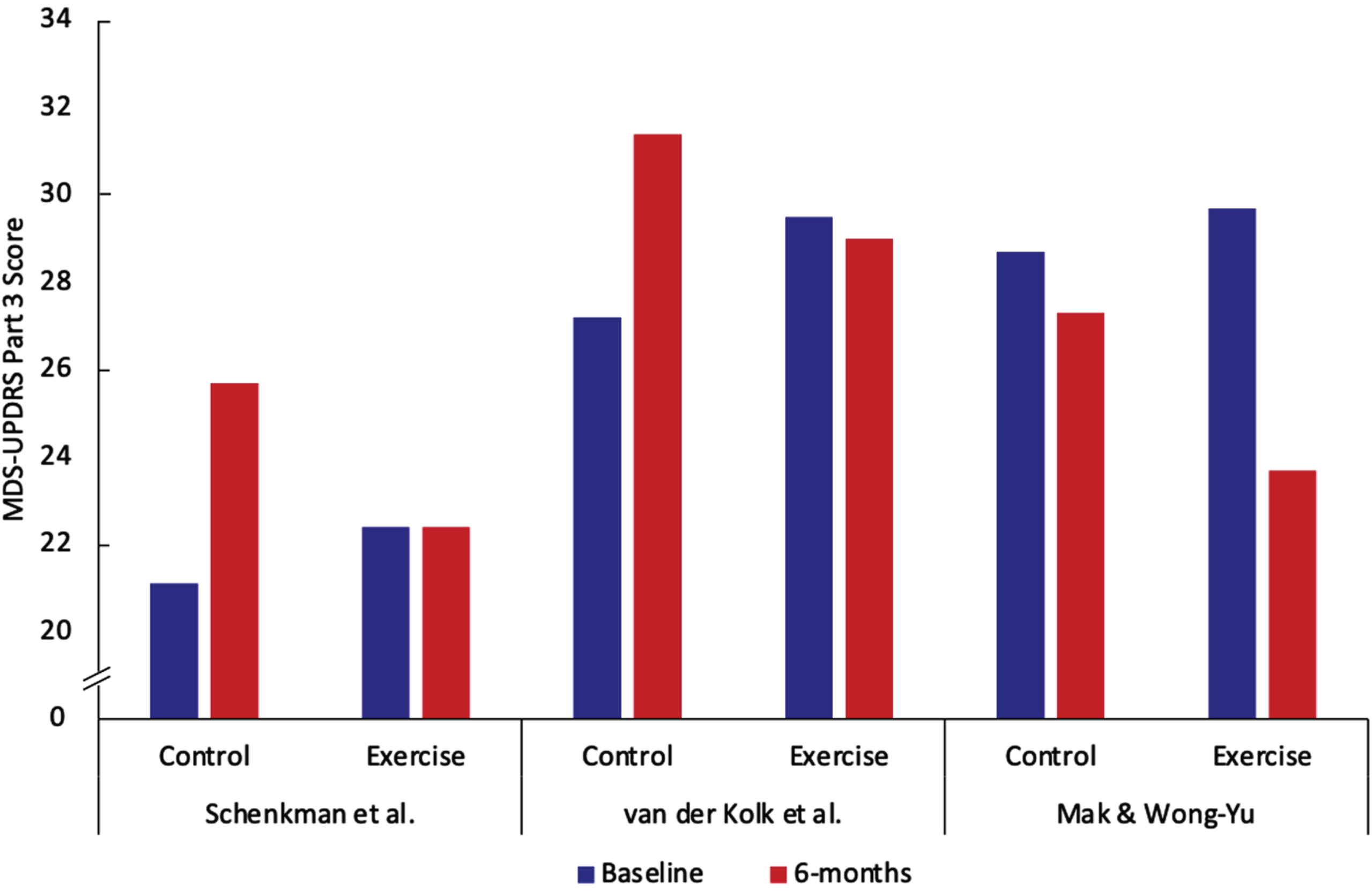
The first component of the exercise prescription is aerobic/endurance exercise [3]. In addition to potentially slowing disease progression, high intensity aerobic exercise increases overall cardiorespiratory fitness [5] which is a key vital sign [9]. There have been three studies conducted which all suggest that high-intensity (approximately 80–85% of peak heart rate) aerobic exercise has the potential to slow disease progression as well as reduce the signs and symptoms of the disease [5–7]. The data in Fig. 1 demonstrates that in all three studies there was at least a 4-point difference on the Movement Disorders Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) over 6 months between moderate- and high-intensity exercise. Modes of exercise varied between the three studies and included treadmill exercise [5], stationary cycling [6], and a brisk walking and balance program [7].The phase 2 clinical trial by Schenkman et al. was conducted in people who were early enough in their PD course that they did not yet need dopaminergic replacement therapy [5]. Any participants who later needed to go on medication after enrolling in the study were still tested for study outcome measures in the off-medication state. The studies by van der Kolk et al. and Mak et al. were conducted on PwPD who had already started medication and thus were further along in their disease course. Participants in the van der Kolk study were tested in the off-medication state while those in the Mak et al. study were tested in the on-medication state. PwPD in the Mak et al. study had greater motor impairment at baseline as evidenced by MDS-UPDRS part III scores on-medications being similar to the scores off-medications in the van der Kolk et al. study and higher MDS-UPDRS part III scores than the drug-naive participants in the study by Schenkman et. al. The Mak et al. study demonstrated the largest reduction in MDS-UPDRS part III of all three studies (a reduction of 6 points) in the high intensity group over six months (Fig. 1). The reason for this larger degree of symptomatic benefit may be due to the multimodal nature of the intervention that Mak et al. employed or the fact that participants with greater motor impairment may have been more likely to show improvements. Because all three studies showed a slower rate of change of the MDS-UPDRS part III in the high-intensity group despite methodologic differences (differences in disease duration and medication-status for testing), the conclusion that high-intensity exercise provides a slower rate of change is robust. A phase 3 trial on drug-naïve participants with testing conducted in the off-state is underway; this trial will definitively address whether exercise is disease modifying [10].
There is also an extensive preclinical body of research that provides possible mechanistic underpinnings for the benefit of aerobic exercise in PD [11–13]. Although each of the three high intensity aerobic studies referred to above used walking, running, or cycling [5–7], these findings likely apply to other forms of aerobic exercise performed at high intensity. Examples include but are not limited to cycling (outdoors), rowing, stair climbing machines, elliptical machines, and swimming [14]. It is important to stress that achieving 80% of peak heart rate can be hard using elliptical machines and swimming. Measuring heart rate during swimming is also more complicated than for other activities.
Resistance exercise/weight training
The second component of the exercise prescription is progressive resistance exercise, also known as weight/strength training. Studies have shown reductions in the symptoms of PD, improvements in physical function [15–18], and improvements in several aspects of cognition because of weight training programs [19–21]. An important point to stress here is that aerobic exercise and progressive resistance exercise have very different molecular and biological effects and, as such, both forms of exercise are equally important and essential [22, 23]. While high-intensity aerobic exercise training may be disease-modifying, resistance training likely allows the maintenance of function by increasing muscle mass and power, which are closely associated with mobility [24]. Resistance exercise also increases bone density [25]. There is also extensive evidence that muscle weakness should be avoided since it is associated with a higher all-cause cardiovascular and cancer risk [26] and this probably applies to PwPD.
Flexibility exercise
The third component of the exercise prescription is flexibility as loss of flexibility can lead to the inability to perform the other components of the exercise prescription and limits range of motion. Stretching exercises are encouraged [27]. Many PwPD benefit from performing flexibility exercises when they wake up to alleviate rigidity/stiffness caused by several hours of limited movement. Flexibility exercises can be performed as an activity alone to alleviate muscle rigidity/stiffness, as part of a warm-up and cool-down, or as part of activities such as yoga and Pilates. It is generally agreed that dynamic stretching is recommended before exercise or activity and static stretching is recommended after exercise. Further details of types of stretching, FITT principles and volume principles can be found on pages 158–161 of ACSM’s Guidelines for Exercise Testing and Prescription Eleventh Edition [27]. The flexibility component of the exercise prescription needs further systematic research in PwPD since it is the least studied of the four components.
Neuromotor exercise
The fourth component of the exercise prescription is balance, agility, and multi-tasking together known as neuromotor exercise. As the disease progresses, posture, gait, and balance become progressively more impaired. As such balance and mobility exercises and activities are required to counteract this. Examples of activities that help balance, mobility and multi-tasking are dancing, tai chi, yoga, table tennis, multimodal training, Nordic walking, aquatic training, exercise gaming, Qigong, Pilates, and circuit training which involve exercises targeting posture and balance [27, 28]. The underlying premise behind all these activities is that they require considerable involvement of the nervous system. As such they have the potential to improve cognition [29] and be beneficial for brain plasticity [30].
CURRENT GUIDELINES FOR THE PD EXERCISE PRESCRIPTION
Aerobic exercise and resistance training form the basis of the PD exercise prescription (PD ExRx); both can be prescribed in clear parameters specifying the frequency, intensity, time, and type (FITT) of exercise as specified in Table 1.
The exercise prescription for Parkinson’s disease
FITT, Fitness, Intensity, Time, Type; HRmax, maximum heart rate; PD, Parkinson’s Disease; 1RM, one repetition maximum.
In addition, the PD ExRx must include recommendations to engage in activities that enhance flexibility, as well as balance/agility/multi-tasking (neuromotor). These latter activities are not so easily prescribed within the traditional parameters of frequency, intensity, time, and type but suggestions are provided in Table 1. It is very important to point out that there is significant evidence that dose does matter for the neuromotor component. A rigorous meta-analysis showed exercise can prevent falls in community-dwelling older people [31]. Exercise programs that challenge balance and are of a higher dose have larger effects [31]. The analysis also showed promise for PwPD and cognitive impairment. In addition, it has been shown that the amount of walking and dual tasking can be increased with PwPD when systematically progressed over a ten-week period [32]. Future studies conducted over at least 6 months and preferably longer are needed to work out the dose guidelines for neuromotor exercise. The prescription presented here is consistent with that developed by the American College of Sports Medicine (ACSM) [33] and the Parkinson Disease Foundation which provides an easy to read one page summary [34]. It is also consistent with a very extensive review of best physical therapy practice as summarized in Table 1 of the clinical practice guidelines from the American Physical Therapy Association [35].
It is important to inform PwPD that many activities also provide health related benefits and can provide greater enjoyment and motivation for some people (e.g., tango-dancing, boxing, and ping-pong). Table 2 outlines the differences between exercise, activities, and traditional rehabilitation therapy. It is important to counsel PwPD that activity classes alone are complementary but not sufficient to fulfill the entire exercise prescription. Many people need additional encouragement and guidance to develop an intense aerobic and resistance program. This approach is consistent with that advocated by Fox and colleagues who reviewed different components of physical interventions and found benefits for PwPD [36].
The difference between exercise, activities, and therapies
We suggest weighting the dosage of the exercise prescription differentially based on personal need, disease stage and, to some extent, personal preference. For people early in their disease without evidence of frailty or imbalance, and desiring to slow down the disease, the emphasis should be on high-intensity aerobic exercise (e.g., 3–4 days a week of aerobic; 2 days of resistance; 1 day of neuromotor). For people who are showing signs of frailty, the emphasis should be on a higher dose of resistance training (e.g., 2–3 days a week of aerobic; 3 days of resistance; 1 day of neuromotor). For people with balance deficits who are at high risk of falling, neuromotor exercise should comprise a greater proportion of the prescription and should be paired with periodic physical therapy. People looking to maintain function should have a balanced plan of all prescription components that does not overwhelm them but rather facilitates compliance.
WHAT WE TELL PEOPLE WITH PARKINSON’S IN OUR CLINIC
Persuading people to take part in activities and exercise is one of the hardest challenges facing medicine. It is well established that a physician advising a patient to obtain the recommended number of minutes of exercise per week is ineffective in achieving that goal. In fact, walking with a doctor has even been suggested as one solution [37]. A detailed review of the literature on successful behavioral interventions is currently being conducted [38]. It is important to educate PwPD who are struggling to stay active, that several epidemiological studies have shown that increased activity, in general, is beneficial. It can prolong life expectancy and improve the quality of life in people with PD [39, 40]. It is also the case that maintaining muscle strength predicts longevity [41]. In other words, some activity is much better than no activity, but there are compelling reasons to follow the guidelines for the exercise prescription as we have outlined.
We suggest discussing the following strategies with PwPD who are eager to begin an exercise program or need encouragement to maintain it.
GENERAL CONSIDERATIONS FOR EXERCISE
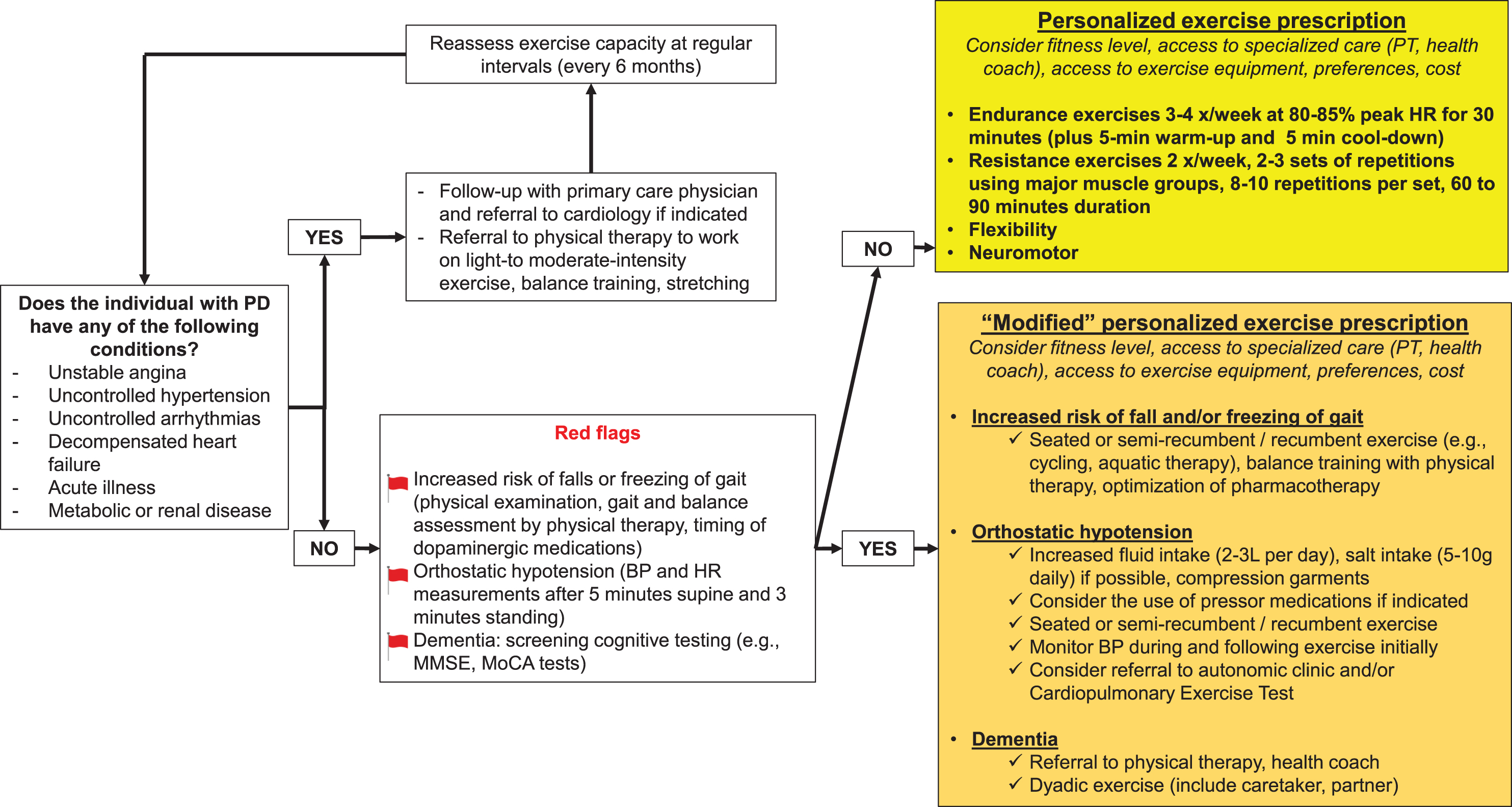
Exercise prescription flowchart for people with Parkinson’s disease.
PD SPECIFIC CONSIDERATIONS FOR EXERCISE
There are at least four other considerations unique to PD and exercise:
CONCLUSION
If a pill could be created that mimicked the effects of exercise, everyone would take it. The emerging field of exercise mimetics is clear witness to this fact [50]. The scientific evidence and the overwhelming and compelling testimony of PwPD make it clear that exercise should be first-line therapy for people with early PD with the goal of creating a lifestyle change. Exercise should continue to be part of the treatment regimen as the disease advances and additional treatments are required. Some physicians have even gone so far as to suggest that the purpose of prescribing medication is to enable people to exercise and take part in activities. This is an opinion with which we concur. This is especially the case since consistent exercise may reduce hospitalization risk [51].
We look forward to the future in which the guidelines that are being developed and revised are used to create a personalized exercise prescription for individuals with PD [52], based on evidence-based data which is accumulating rapidly. The personalized prescription would be crafted on: 1) an initial assessment of medical needs by a physician, and 2) an initial assessment of physical and functional ability by a physical therapist or neuromotor trained specialist along with consideration of: fitness level, goals of the person, disease severity, motor fluctuations, cognitive impairment, balance, agility, and mobility, access to specialized care (PT, neuromotor specialist, health coach or lifestyle navigator), access to exercise equipment (home, fitness center), and exercise and activity preference.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
The research reported in this publication was supported by the National Institute of Neurological Disorders and Stroke of the National Institutes of Health under Award Numbers U01NS113851 and K23NS123506. Research is also supported by the National Institutes of Health’s National Center for Advancing Translational Sciences, Grant Number UL1TR001422. It is also supported by a generous philanthropic gift in honor of Howard Gilbert and a gift from the JCS Family Foundation.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.