
Abstract
Background:
Multiple observational studies have yielded controversial results regarding the association between Parkinson’s disease (PD) and periodontitis.
Objective:
This systematic review and meta-analysis was conducted to ascertain their bidirectional relationship.
Methods:
A literature search for relevant studies was performed in PubMed, EMBASE, the Cochrane Library, and Web of Science databases from inception to December 19, 2022. Effect sizes (ES) with 95% confidence intervals were pooled under the random-effects model. Then, leave-one-out sensitivity analysis and contour-enhanced funnel plot were applied to assess the stability of the results.
Results:
A total of 34 studies and 24 studies were included for systematic review and quantitative meta-analysis, respectively. Pooled ES indicated that periodontitis was not significantly associated with PD risk (HR = 1.13, 95% CI 0.88–1.45, n = 3; OR = 1.94, 95% CI 0.55–6.90, n = 7), while the Mendelian randomization study revealed no association between PD and periodontitis risk (coefficient [B] = –0.0001, standard error = 0.0001, p = 0.19). Furthermore, PD patients exhibited higher levels of periodontal pocket depth (SMD = 1.10, 95% CI 0.53–1.67), clinical attachment level (SMD = 1.40, 95% CI 0.55–2.26), plaque index (SMD = 0.81, 95% CI 0.22–1.39), and Oral Health Impact Profile-14 score (SMD = 0.91, 95% CI 0.33–1.49) compared to healthy controls.
Conclusions:
Our meta-analysis identified no bidirectional association between PD risk and periodontitis risk, though the prevalence of periodontitis and poorer oral status was higher in PD patients.
INTRODUCTION
Parkinson’s disease (PD) is a progressive neurodegenerative disorder manifested by bradykinesia, resting tremor, rigidity, and postural instability, affecting millions of elderly adults globally. Between 1990 and 2016, the age-standardized prevalence, disability-adjusted life-years rates and mortality of PD have skyrocketed in almost every region worldwide, increasing the heavy global financial burden [1, 2]. Despite the specific pathogenesis remaining elusive, inflammatory and immunological factors have been suggested to participate in its underlying mechanisms [3, 4].
Periodontitis is a chronic inflammatory disease of the oral cavity that is triggered by the formation of dental plaque biofilm [5]. Advanced periodontitis is a leading cause of loss of teeth and supporting structures, affecting approximately 10–15% of the global population [6]. According to the data from the 2009–2012 National Health and Nutrition Examination Survey, its overall prevalence among Americans over 30 years was estimated to be as high as 46% [7, 8]. It has been observed that the prevalence of total periodontitis rises from the 30–34 age group to the aged 65+ age group [7]. The progression of age, coupled with reduced dexterity, results in the accumulation of dental plaque, leading to more frequent and severe periodontal inflammation [9], which may elevate the longitudinal risk of periodontitis. Moreover, periodontitis has been reported to be correlated with several systemic diseases, such as diabetes mellitus, cardiovascular diseases [10], Alzheimer’s disease (AD) [11], and cancer [12].
Various articles have reported the high prevalence of periodontitis and poor oral health in individuals with PD. For instance, a nested case-control study reported that the prevalence of periodontal diseases attained 48.73% in a cohort of 4765 PD patients [13]. In a cross-sectional case-control study, periodontitis was detected in 98 out of 104 PD patients [14]. Several factors could potentially explain the link between the prevalence or risk of periodontitis and PD. As is well documented, polypharmacy, cognitive impairment, motor dysfunction, and the subsequent deducing dental care elevate the risk of dental caries and periodontal disorders [15]. Sialorrhea, a commonly observed symptom of PD, is also hypothesized to promote periodontitis and other oral diseases, attributable to hypersalivation altering the composition of oral microbiota (like K. oralis) in PD cases and facilitating local inflammation in the oral cavity [16]. Additionally, the prevalence of sialorrhea has been reported to increase with age and disease duration in PD patients [17], insinuating that it may mediate the impact of age and PD duration on periodontitis risk. Similarly, gender is also considered a key factor in the development of sialorrhea, thereby influencing periodontitis risk, which can be supported by the finding that males with PD were twice more likely to develop sialorrhea compared to females [18]. Hyposmia, characterized by a reduced sense of smell in PD patients [19], which deteriorates significantly with age [20] and is often accompanied by taste dysfunction, contributes to prolonged mealtimes and inadequate chewing [15], thus the increasing risk of periodontal diseases. Moreover, since female gender might be a contributing factor for dysphagia [15, 21], another plausible explanation for the effect of gender on periodontitis risk is that dysphagia may result in acid reflux, which could trigger perimylolysis tooth erosion and potentially increase the periodontitis risk [22]. In addition, Fukayo et al. [23] reported that female PD patients brushed their teeth more frequently than male patients and tended to have a lower decayed, missing and filled teeth (DMFT) index than the male group, indicating that the alterations in dental care behavior may also be a reason for gender influencing periodontitis risk.
Despite numerous articles investigating the association between PD and periodontitis, their findings have been contradictory. While certain large-sample observational studies have noted that periodontal inflammatory disease is correlated with an elevated risk of developing PD [24, 25], other studies have yielded conflicting results. For example, a Mendelian randomization (MR) study revealed no convincing genetic association between the two diseases [26]. Meanwhile, the bidirectional relationship between PD and periodontitis has not been systematically assessed.
Therefore, we sought to systematically review studies focusing on PD and periodontitis and perform a meta-analysis to comprehensively investigate the bidirectional association between the two diseases and summarize the oral status of PD patients.
METHODS
Literature search
A systematic literature search of PubMed, EMBASE, the Cochrane Library, and Web of Science was performed for studies published until December 19, 2022 using the following keywords: Parkinson’s disease, parkinsonism, periodontitis, and periodontal disease. The detailed search strategies for PubMed search are provided in the Supplementary Material.
Eligibility criteria
Studies were considered eligible for inclusion if they investigated the relationship between PD and periodontitis or the oral status of patients. Besides, we also reviewed the reference lists of the related articles and screened for potentially relevant conference abstracts. The exclusion criteria were as follows: 1) reviews, case reports, letters, comments, or other types of articles; 2) studies of animal or cell models; 3) studies without quantitative data. Regarding duplicate publications reporting the same cohort, the study with the largest sample size was included.
Data extraction
Two reviewers (Y.Q.C. and K.L) independently extracted the following data from included studies: 1) study characteristics (the first author, publication year, study design); 2) population parameters (sample size, country, age, gender); 3) assessment of PD and periodontitis or oral status (scale of diagnosis, disease duration, clinical parameter values); 4) hazard ratios (HR), odds ratios (OR), standardized mean differences (SMD), and their corresponding 95% confidence intervals (CI). If both unadjusted and adjusted effect sizes were available, data on the latter were collected.
Any discrepancies were resolved by arbitration with a third reviewer (D.H.Y.).
Quality assessment
The methodological quality of all eligible studies in the systematic review was independently assessed by Y.Q.C. and K.L. The Newcastle Ottawa Scale (NOS), consisting of three parameters of quality: selection, comparability and exposure or outcome assessment, was used to assess the quality of the cohort studies and case-control studies. Meanwhile, the quality of cross-sectional studies was assessed using the Joanna Briggs Institute (JBI) checklist. The quality assessment of the MR study was based on the STROBE-MR Checklist [27].
Outcomes
The co-primary outcomes of our study were the risk of PD in patients with periodontitis and the risk of periodontitis in PD patients. Secondary outcomes were periodontal clinical parameters values including periodontal pocket depth (PPD), clinical attachment level (CAL), plaque index (PI), and the percentage of bleeding on probing sites (BoP %), all of which examined the prevalence of periodontitis in PD cases. Besides, based on the enrolled studies, we also pooled other oral hygiene parameters to assess the oral status and oral health of PD patients.
Statistical analysis
We performed a quantitative meta-analysis of the studies included in the systematic review to merge results for the outcomes reported with the same metrics in more than two studies. All statistical analyses were conducted via R software (version 4.1.0). Effect sizes (ES) were calculated as hazard ratios (HR), odds ratios (OR), and standardized mean differences (SMD), along with their corresponding 95% confidence intervals (CIs). Heterogeneity was determined with the Cochran Q statistic and the I2 statistic, with the significance level set at a 2-tailed value of p < 0.05 and I2 >50% indicating significant heterogeneity. Given the presence of heterogeneity, the study estimates were combined under the random-effects model. Leave-one-out sensitivity analysis was carried out to assess the stability of the combined results. Contour-enhanced funnel plot [28] and the Duvall and Tweedle trim-and-fill approach [8] were used to evaluate potential publication bias.
RESULTS
Literature search
The literature search yielded 2,708 studies, and three additional publications were identified by reviewing reference lists. After excluding duplicates, a total of 1,985 unique titles and abstracts were screened. Subsequently, the full text of 52 potentially eligible articles was reviewed. Following a thorough assessment, 18 studies were excluded: four studies using the same data from another publication, four studies reporting dementia or cognitive impairment as the outcome, and ten conference abstracts did not report quantitative data. Therefore, 34 studies were included in the systematic review. Concerning studies with data on control groups, a quantitative meta-analysis was performed on 24 studies (involving 7,720,793 participants) reporting the same outcomes. The process of study identification is illustrated in the PRISMA flow chart [29] in Fig. 1.
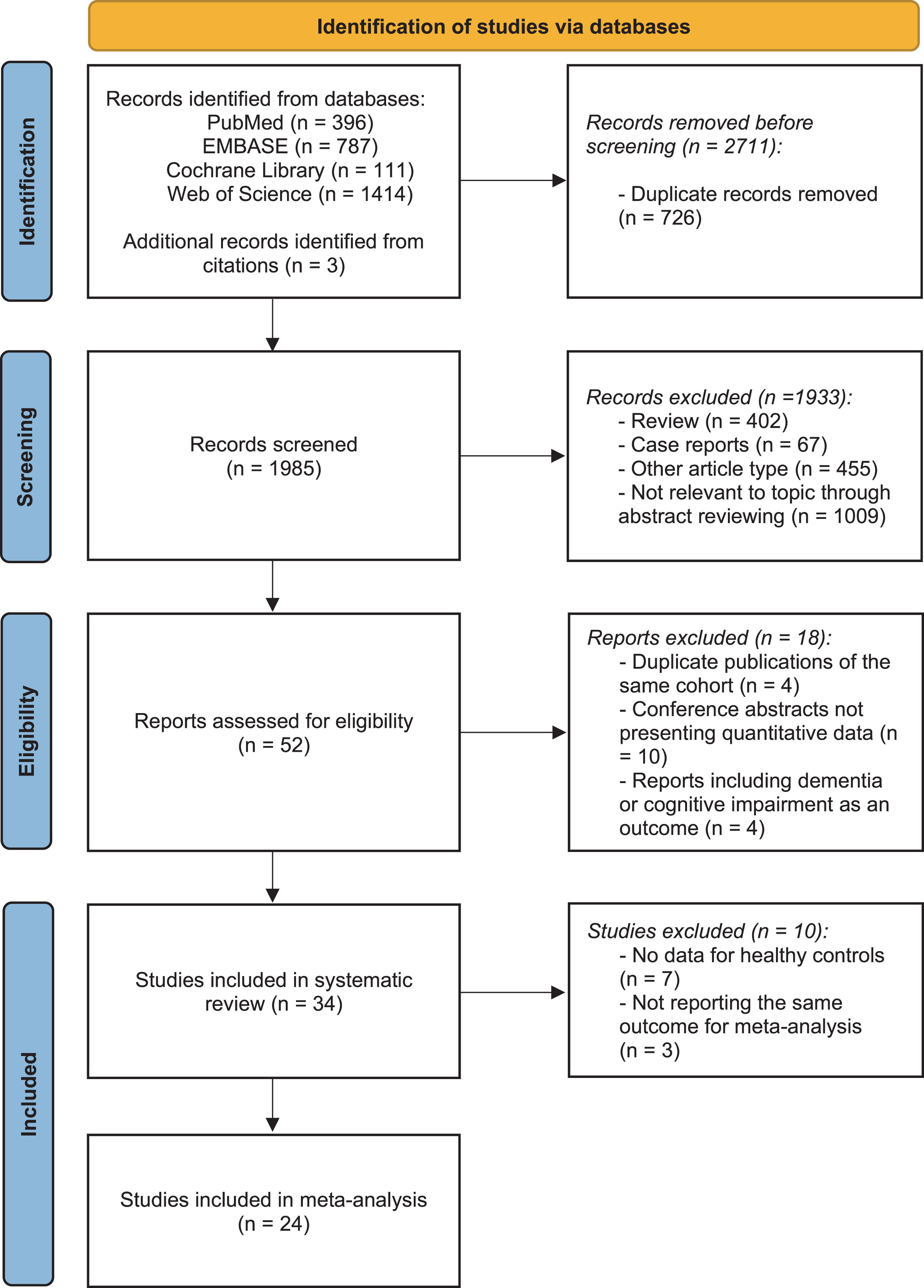
PRISMA flow diagram delineating study identification.
Study characteristics and quality assessment
The characteristics of 34 studies included in the systematic review are summarized in Table 1. The included studies comprised six cohort studies, sixteen case-control studies, eleven cross-sectional studies, and an MR study. The majority of the studies assessed the severity of PD using Hoehn and Yahr (H&Y) stage, United Parkinson’s Disease Rating Scale (UPDRS), or Movement Disorder Society-sponsored United Parkinson’s Disease Rating Scale (MDS-UPDRS). However, the diagnostic criteria and clinical periodontal examination protocols for periodontitis and oral status varied and were inconsistent among the studies. Due to a lack of data on healthy controls and the heterogeneity of outcomes, three cohort studies, fifteen case-control studies, five cross-sectional studies, and the MR study were eventually included in the meta-analysis.
Characteristics of included studies in the systematic review
PD, Parkinson’s disease; ES, effect size; HR, hazard ratio; OR, odds ratio; PDD, periodontal pocket depth; CAL, clinical attachment level; PI, plaque index; BoP%, the percentage of bleeding on probing sites; OHI, oral hygiene index; OHIP-14, Oral Health Impact Profile-14; DMFT, decayed, missing, and filled teeth index; UPDRS, United Parkinson’s Disease Rating Scale; MDS-UPDRS, Movement Disorder Society-sponsored United Parkinson’s Disease Rating Scale.
Table 2 presents the detailed quality score of each included study. All six cohort studies and the majority of the case-control studies (13 out of 16 studies) were deemed to be of high methodological quality (low risk of bias), with a NOS score of ≥7 (Table 2A, B). Likewise, the ten cross-sectional studies were also of high quality, according to the JBI checklists (Table 2C). Additionally, the detailed checklist items of the Mendelian randomization study according to the Reporting of Observational Studies in Epidemiology Using Mendelian Randomization (STROBE-MR) Checklist are listed in Table 2D.
Methodological quality assessment of included studies
Y, Yes; N, No; U, Unclear. *Q1: Was the sample frame appropriate to address the target population? *Q2: Were study participants sampled in an appropriate way? *Q3: Was the sample size adequate? *Q4: Were the study subjects and the setting described in detail? *Q5: Was the data analysis conducted with sufficient coverage of the identified sample? *Q6: Were valid methods used for the identification of the condition? *Q7: Was the condition measured in a standard, reliable way for all participants? *Q8: Was there appropriate statistical analysis? *Q9: Was the response rate adequate, and if not, was the low response rate managed appropriately?
Association between periodontitis and risk of PD
The overall HR for the 3 cohort studies (involving 7,298,955 participants) was 1.13 (95% CI 0.88–1.45, p = 0.3436, I2 = 96%; Fig. 2A), demonstrating substantial evidence that periodontitis is not associated with the incidence of PD. In line the results of cohort studies, the combined OR, including 4,844 participants from six retrospective studies and one Mendelian randomization study [26] also showed an overall null effect (OR 1.94, 95% CI 0.55–6.90, p = 0.3040, I2 = 81%; Fig. 2B) for the association between periodontitis and the risk of PD.
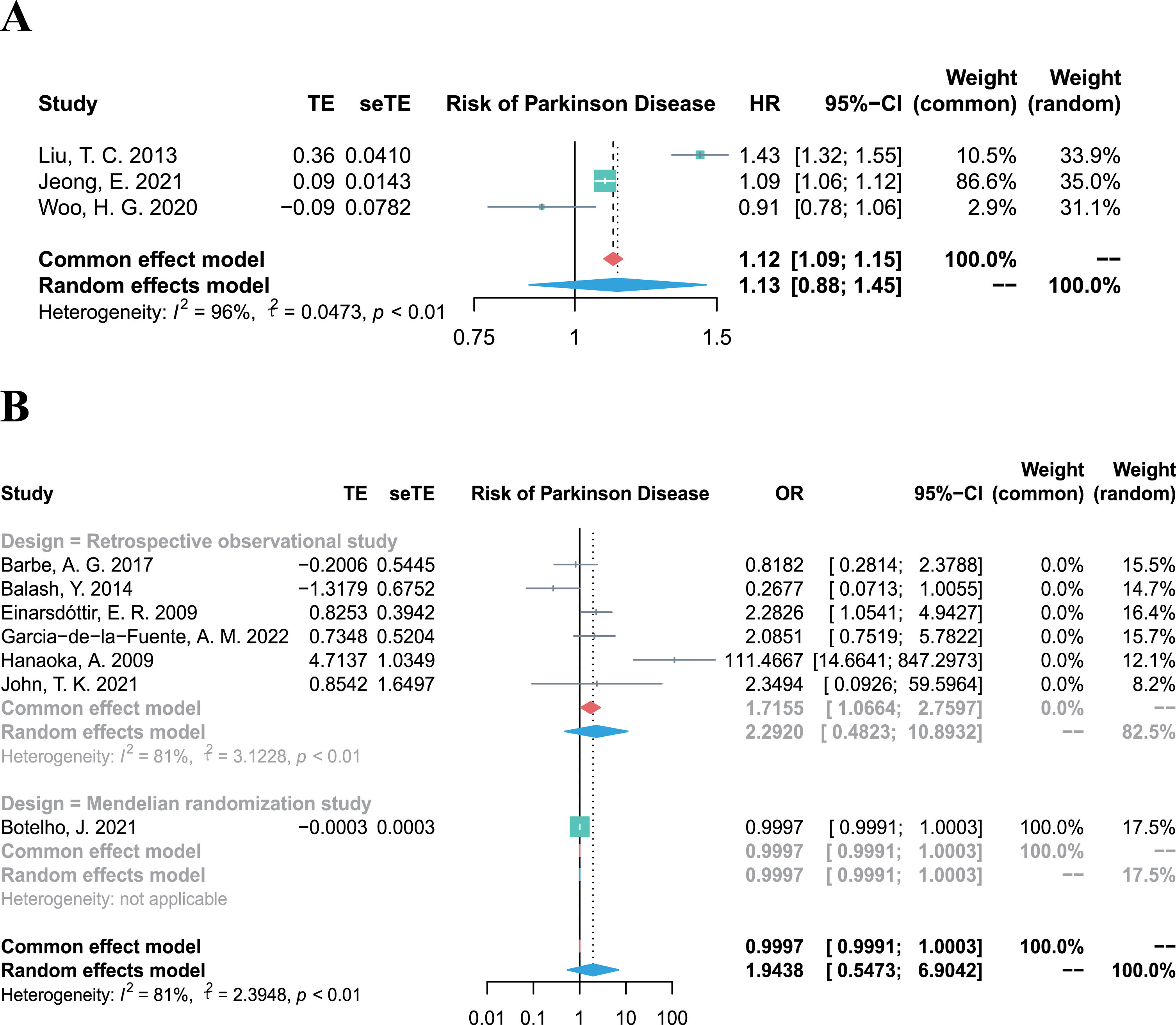
Forest plots of meta-analysis for the association between periodontitis and risk of Parkinson’s disease, combining the HR of three cohort studies (A), and combining the OR of six retrospective studies (B).
Association between PD and risk of periodontitis
The bidirectional Mendelian randomization study was the only study that investigated the relationship between PD and the risk of periodontitis, and found no significant genetic association between them when analyzing the data from genome-wide association studies involving 417,508 participants (coefficient [B] = –0.0001, standard error [SE] = 0.0001, p = 0.19) [26].
Association between PD and prevalence of periodontitis
Owing to the diverse and heterogeneous outcomes in the included studies, periodontal clinical parameter values were integrated to evaluate the prevalence of periodontitis and the periodontal status of PD patients. The pooled PPD in PD patients was significantly higher than that in control groups (SMD = 1.10, 95% CI 0.53–1.67, p = 0.0002, I2 = 85%; Fig. 3A). Similarly, the CAL of PD patients was significantly higher (SMD = 1.40, 95% CI 0.55–2.26, p = 0.0013, I2 = 92%; Fig. 3B) compared to control groups, and the PI of PD patients was also significantly higher (SMD = 0.81, 95% CI 0.22–1.39, p = 0.0072, I2 = 87%; Fig. 3C). Besides, although the BoP % was higher in PD groups than that in control groups, there was high heterogeneity and no statistically significant difference (SMD = 0.80, 95% CI –0.65–2.25, p = 0.2803, I2 = 96%; Fig. 3D). Above all, PD patients exhibited higher values of periodontal clinical parameters, indicating a higher prevalence of periodontitis among PD cases.
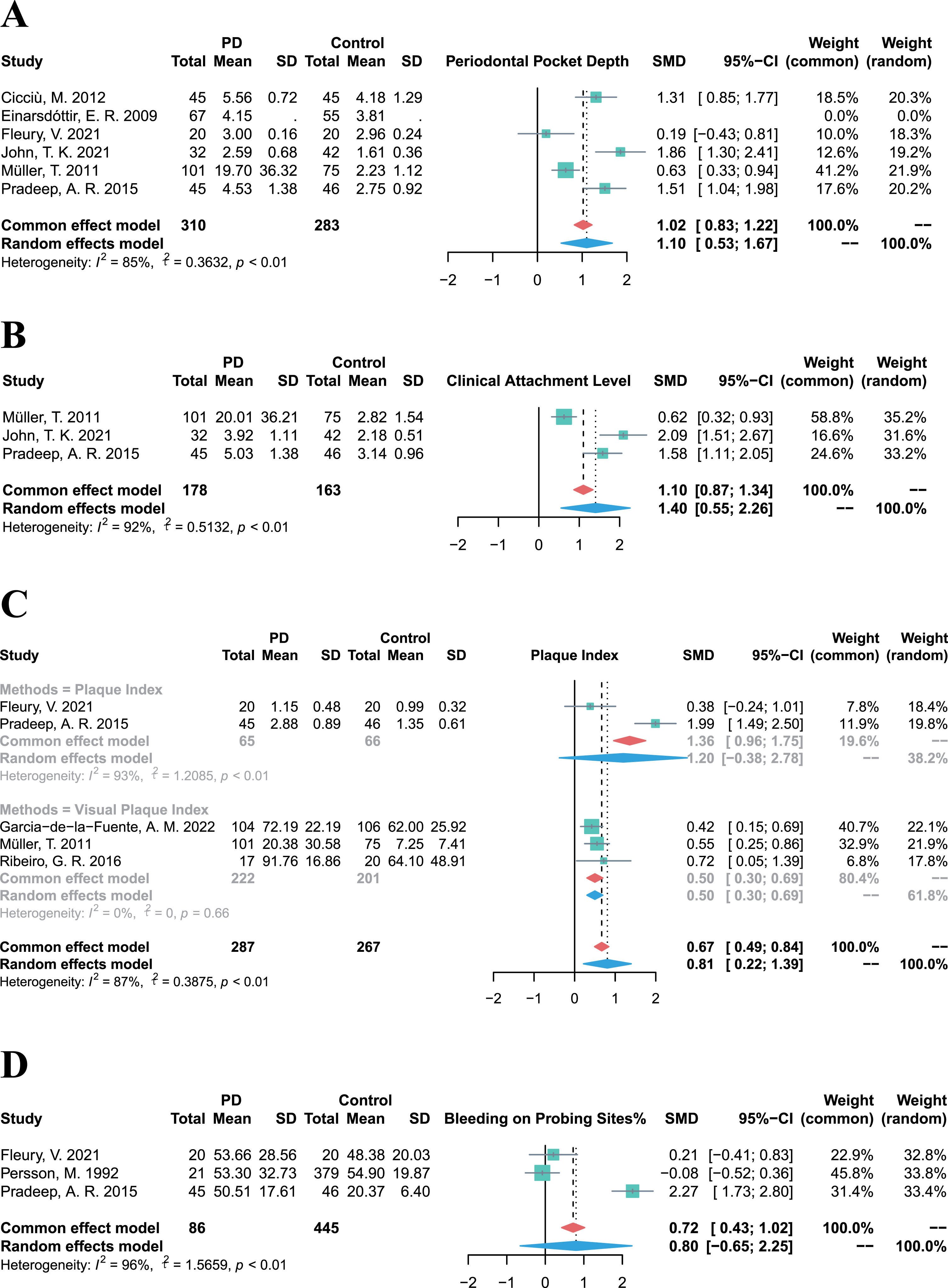
Forest plots of meta-analysis for PPD (A), CAL (B), PI (C), and BoP% (D) in patients with Parkinson’s disease.
Oral status in PD
Nevertheless, considering PD patients are likely to present poor oral hygiene in clinical practice, we also conducted meta-analysis on additional clinical parameters of oral hygiene status and summarized the oral manifestation of PD patients in Table 3. PD patients experienced an unfavorable oral health-related quality of life, as evidenced by significantly higher scores on the Oral Health Impact Profile (OHIP-14) in the PD group (SMD = 0.91, 95% CI 0.33–1.49, p = 0.0022, I2 = 80%). Compared to controls, PD patients had a higher prevalence of xerostomia (OR = 3.60, 95% CI 2.79–4.65, p < 0.0001, I2 = 26%), in accordance with their declining salivary flow rate (SMD = –0.43, 95% CI –0.80– –0.05, p = 0.0260, I2 = 76%). While PD patients suffered from significantly higher tooth mobility (OR = 6.67, 95% CI 1.73–25.68, p = 0.0058, I2 = 69%), they also had a tendency to experience edentulism (OR = 1.44, 95% CI 0.65–3.20, p = 0.3644, I2 = 73%) and exhibit a higher number of loss teeth (SMD = 0.34, 95% CI –0.26–0.94, p = 0.2644, I2 = 89%), decayed teeth (SMD = 0.28, 95% CI –0.09–0.65, p = 0.1417, I2 = 81%), and a higher DMFT index (SMD = 0.10, 95% CI –0.50–0.70, p = 0.7397, I2 = 91%), although these differences were not statistically significant. Overall, the prevalence of poorer oral health tended to be higher in PD patients. The relevant forest plots are displayed in the Supplementary Material.
Overview of the oral status and dental manifestation of patients with Parkinson’s disease
ES, effect size; SMD, standard mean difference; OR, odds ratio; CI, confidence interval; OHIP-14, Oral Health Impact Profile-14; DMFT, decayed, missing, and filled teeth index.
Sensitivity analysis
The leave-one-out sensitivity analysis revealed that no single study altered the pooled effect of HR and OR (Fig. 4A, B), proving the robustness of our results, which demonstrated no significant association between periodontitis and the risk of PD. Additional results of the sensitivity analyses on other outcomes (PPD, CAL, PI, and BoP%) are provided in the Supplementary Material.
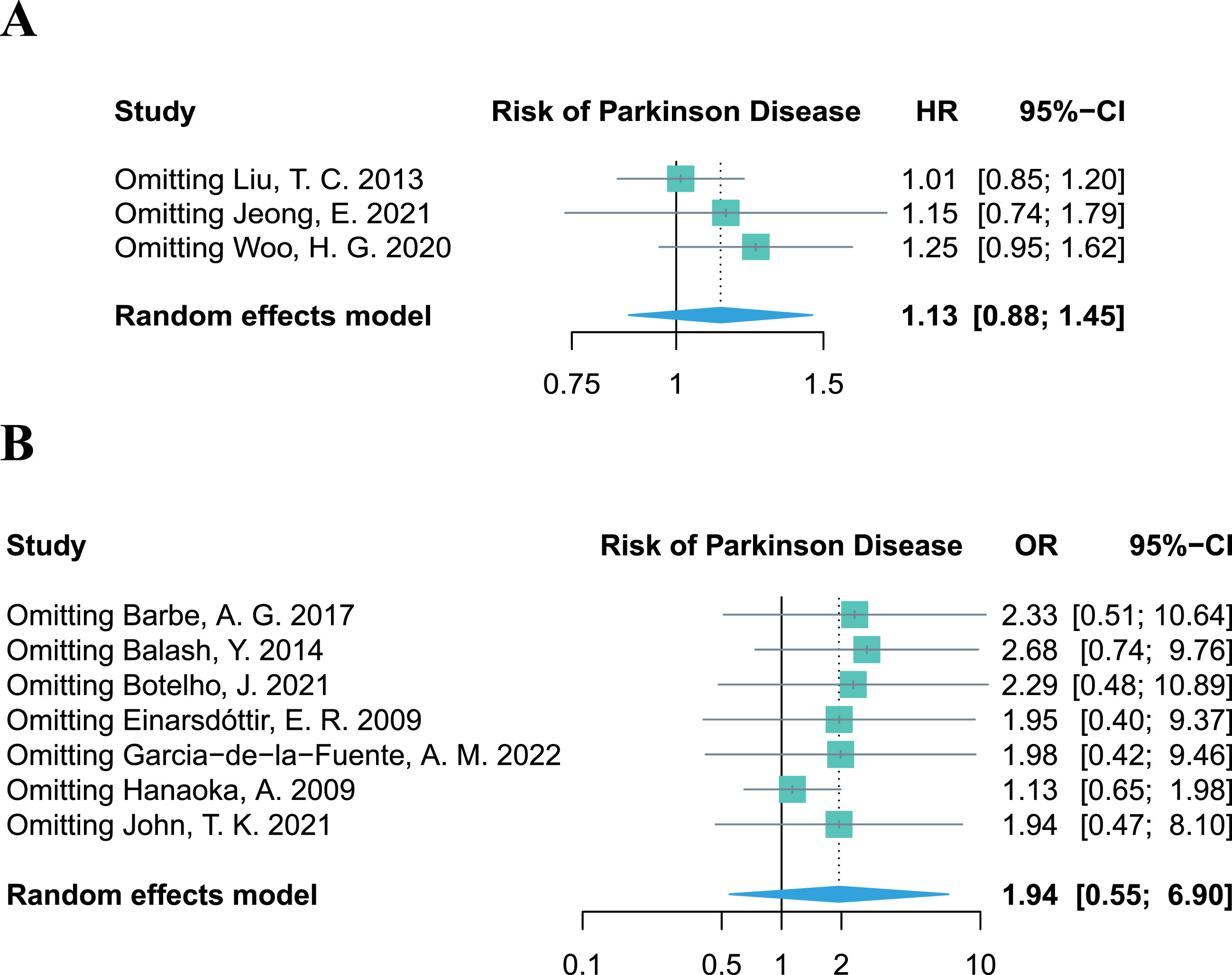
Leave-one-out sensitivity analysis of studies focusing on periodontitis and the risk of Parkinson’s disease.
Publication bias assessment
Due to the limited number of included studies for each outcome in the meta-analysis, a contour-enhanced funnel plot was only performed for the seven retrospective studies regarding periodontitis and the risk of PD. Asymmetry of the funnel plot was observed. In the contour-enhanced funnel plot (Fig. 5), the hollow dots filled by trim-and-fill approach depicted that one filled study was situated in sky-blue areas indicating high statistical significance (p < 0.01), whereas another filled study was located in white areas of no statistical significance. This discrepancy demonstrates that the potential publication bias may stem from the study conducted by John et al. [30]. However, even after excluding this study in the leave-one-out sensitivity analysis, the combined OR remained statistically insignificant (OR = 1.94, 95% CI 0.47–8.10, p = 0.3614; Fig. 4B), which further supports the stability of our results.
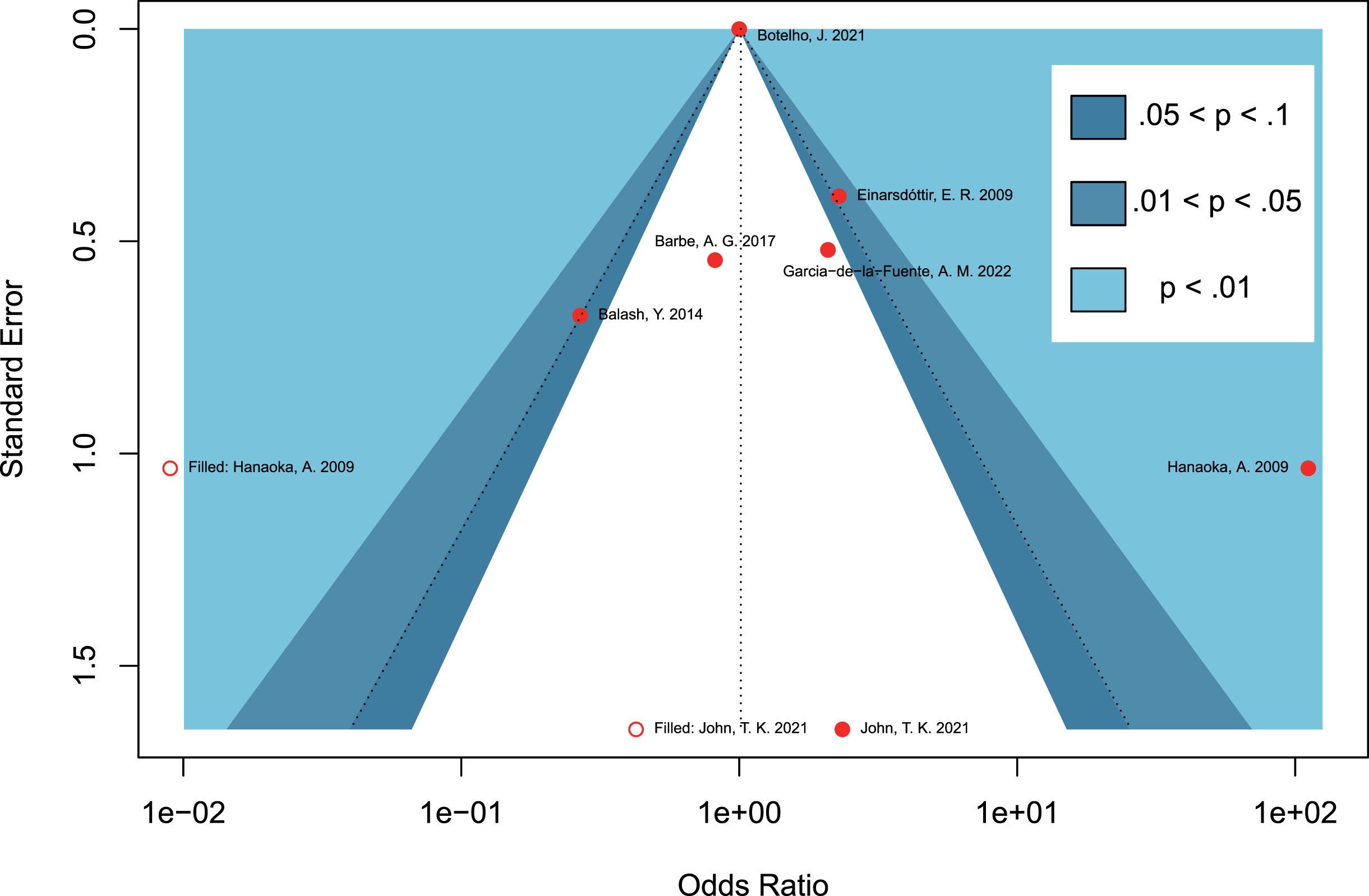
Contour-enhanced funnel plots assessing the potential publication bias on studies concerning periodontitis and the risk of Parkinson’s disease.
DISCUSSION
The principal findings of our meta-analysis imply that patients with periodontitis do not tend to have a higher risk of developing PD, and that PD patients might not confer a higher risk of periodontitis. Nonetheless, it was observed that PD patients presented a higher prevalence of periodontitis and other periodontal diseases, as well as poorer oral hygiene.
Our findings, which demonstrate no association between periodontitis and PD risk, are in agreement with a prospective cohort study recruiting 15,528 patients [31]. This study illustrated that the risk of PD was not significantly associated with dental plaque whether in males (pooled HR = 1.23, 95% CI 0.81–1.86, p = 0.3309, I2 = 0%) or in females (pooled HR = 0.86, 95% CI 0.56–1.31, p = 0.4788, I2 = 0%). However, due to the heterogeneity of the outcomes (the presence of dental plaque but not confirmed periodontitis), this study was only included for the systematic review but not in the quantitative meta-analysis.
Previous studies have stressed the significant role of periodontitis in the pathogenesis of PD, demonstrating that periodontitis triggers the systemic translocation of bacteremia and inflammatory mediators, resulting in the breakdown of the blood-brain barrier and activation of microglia, eventually driving in necrosis and apoptosis of dopaminergic neurons and contributing to the mechanism of PD [32, 33].
In contrast to these viewpoints, we posit that the subsequent inflammatory processes may play a dominant role in the progression of PD, rather than periodontitis itself, with periodontitis serving as one of the numerous initiating factors of inflammation. Our hypotheses are supported by the following evidence.
As was reported in one of the included studies [16], although there were no differences in dental or periodontal parameters between 20 PD patients and 20 healthy controls, the elevated pro-inflammatory cytokine levels, such as interleukine-1β and tumor necrosis factor-α, were still observed in the gingival crevicular fluid of PD cases compared with controls. This reflected the presence of active peripheral inflammatory responses in the oral cavity of PD patients, irrespective of the presence of periodontitis, thus partially corroborating our assumptions.
Furthermore, a study [34] enrolling 37 PD patients reported an increase in the number of various inflammatory cells, including leukocytes, basophils, and segmented neutrophils, in PD cases complicated by periodontitis. Intriguingly, another study involving 51 PD participants described the levels of circulating high-sensitive C-reactive protein were increased in the periodontitis group, whereas the lymphocyte levels were elevated in the group without periodontitis [35]. However, these studies did not include a periodontitis control group without PD, which prevented the investigation of whether the rising levels of inflammatory cells and parameters were primarily attributed to PD or periodontitis itself. Thus, further studies are required to clarify the mediating role played by inflammatory factors in these two diseases.
Apart from that, previous research has emphasized the essential role of inflammation in the development of PD. It has been suggested that systemic inflammation events could induce neuronal death and contribute to the progression of neurodegenerative diseases [36]. Specifically, activated glial and peripheral immune cells could mediate neuroinflammatory processes which are deleterious to neurodegeneration and stimulates the death of dopaminergic cells [3]. Besides, inflammation appears to be the bridges connecting several chronic diseases with PD. For example, there are shared inflammation dysregulated pathways linking diabetes with PD [37]. Additionally, chronic kidney disease promotes PD development by exacerbating inflammation and oxidative stress via excessive activation of immune response caused by metabolic toxins [38]. Hence, further studies should be undertaken to investigate the extent to which inflammation plays a role in the progression of PD.
Intriguingly, it is worthwhile noting that our results regarding causal inference between PD and the periodontitis risk were primarily inferred from the MR study, since it was the sole study in the literature examining their association. However, MR study could only assist in confirming their weak association with genetic liability. As documented in the MR study, MR may be powerless in the presence of a strong environmental interaction and may not be able to elucidate the influence of a disease on the occurrence of another disease during a specific period of lifetime, thereby resulting in potentially inaccurate conclusions [26]. In line with this perspective, the result of the lack of association between PD and the risk of periodontitis should be interpreted with caution. Considering the higher prevalence of periodontitis and worse oral cavity health among PD patients, we speculate that it is the several environmental factors that mediate the spurious weak association between PD and periodontitis risk, and that these factors cannot be evaluated at the genetic level using an MR study. For instance, motor deficits in PD patients might be an influencing environmental factor. Indeed, the manifestation of motor impairment, hypokinesia, and involuntary movements in PD patients hinder their capability to maintain their daily oral hygiene, ultimately giving rise to poor oral health prognosis and deterioration in their quality of life [39]. Meanwhile, insufficient dental management induced by cognitive impairment may also be an environmental factor placing PD patients at risk for dental caries and periodontal diseases [15], as neglect of oral cavity disorders by PD cases, their caregivers and their professional physician has been reported [40]. Furthermore, other common symptoms of PD patients, like hyposmia, taste dysfunction [19], dysphagia [21], and masticatory disturbance [41], would contribute to longer meal times and more inadequate mastication, inducing a reduction in food intake quantity and quality, thereby causing nutritional imbalance and deterioration of oral health disorders in PD [15]. Last but not least, fluctuations in eating habits, such as preference for soft sticky foods [42] or sweets [43], would also conduce to the formation of cariogenic environments and subsequently lead to the occurrence of periodontal diseases [15]. In a nutshell, the aforementioned non-negligible environmental factors may potentially account for the high prevalence of periodontal diseases and poor oral health of PD patients, and more studies are necessitated to explore their effect.
The association between the risk of periodontitis and another degenerative disease, AD, has yielded inconsistent conclusions as well. In addition to a longitudinal study determining no statistical differences in several periodontal parameters between AD patients and healthy controls during 3 years of follow-up [44], no significant association between AD and periodontitis risk (RR = 1.4, 95% CI 0.9–2.1) was also reported by another study including 174 AD patients [45]. However, a population-based cohort study recruiting 8,640 individuals demonstrated an inverse association between AD and periodontitis risk (HR = 1.667, 95% CI 1.244–2.232, p = 0.0004) [46]. Hence, the relationship between AD and the risk of periodontitis also remains paradoxical and requires further investigation. Likewise, since our result on the weak association between PD and periodontitis risk may be biased and unreliable in our study, their casual association remains to be further investigated and clarified by additional well-designed and large-scale observational studies.
Our study possesses several strengths. To the best of our knowledge, this is the first systematic review and meta-analysis to comprehensively evaluate the bidirectional association between periodontitis and PD. Moreover, integrating the evidence from a Mendelian randomization study enhances the robustness and persuasiveness of our findings, since MR is widely recognized as providing higher-quality evidence compared to conventional observational studies by utilizing genetic variation as an instrumental variable to detect causality. Furthermore, contrary to previous theories, our intriguing findings provide no compelling evidence to support a bidirectional correlation between the incidence of the two diseases, neither in clinical manifestation nor in genetic liability [26], which may challenge traditional hypotheses concerning their potential relationship. Lastly, our study demonstrated that PD patients indeed suffer from poor oral hygiene, which has implications for guiding the management of dental diseases and improving oral care among PD patients.
Some potential limitations of our study should also be acknowledged. First of all, high heterogeneity was detected in our results, which can be chiefly attributed to variations in diagnostic criteria for periodontitis and measurements of outcomes. The lack of consensus on the definitions of periodontitis, discrepancies in periodontal examination methods, and the heterogeneity in dental conditions pose challenges in estimating the actual prevalence of periodontitis [47] while these factors were also an important source of high heterogeneity in our results and the asymmetry of the funnel plot. Thus, caution should be exercised in interpreting our results due to the existing heterogeneity. However, sensitivity analysis and contour-enhanced funnel plots supported the stability of our findings, reinforcing the credibility of our results. Secondly, as previously mentioned, the weak association between PD and the risk of periodontitis may be unreliable and should be interpreted with caution. This is primarily due to only one MR study addressing this topic while large-scale cohort studies focusing on the risk of periodontitis in PD patients with long-term follow-up are scarce, which also prevented an accurate reviewing and assessment of the incidence of periodontitis in PD cases. Finally, despite the limited number of included studies, grey literature databases comprising unpublished articles were not searched, given the uncertainty in their level of evidence quality. Despite these limitations, our study comprehensively evaluated the association between PD and periodontitis and provide profiles of the oral status of PD patients, which could aid dentists and specialist physicians in formulating considerate dental care strategies for PD patients to optimize their overall quality of life.
Conclusion
Our meta-analysis demonstrated that there might be no bidirectional association between periodontitis risk and PD risk, while PD patients tend to suffer from poor oral health.
Footnotes
ACKNOWLEDGMENTS
We appreciate the efforts of all the authors for this article. We also thank Home for Researchers editorial team (www.home-for-researchers.com) for language editing service.
FUNDING
This study was supported by the National Natural Science Foundation of China (No. 82302081) and the Fundamental Research Funds for the Central Universities (No. 226-2023-0067).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The datasets generated during and/or analyzed during the current study are available upon reasonable request from the corresponding author.