
Abstract
Background:
To improve Parkinson’s disease (PD) care, interdisciplinary and patient-centered treatment is mandatory. A key problem in many healthcare systems is the limited and unspecific communication among different healthcare professionals. Optimal collaboration between various professionals involved is indispensable. Parkinson’s Network Münsterland + (PNM +) is an interdisciplinary network of medical and non-medical experts involved in the treatment of PD patients in Germany.
Objective:
The aim of this evaluation was to analyze the network structures of PNM+ as well as communication and collaboration between PNM + partners.
Methods:
A mixed methods approach was applied consisting of a social network analysis, a validated questionnaire on team effectiveness and semi-structured interviews focusing on perceived barriers and supportive aspects of PNM + .
Results:
Quantitative and qualitative data suggested increased collaboration between professionals within PNM + . The reciprocity of connections was 0.522 in the network of professional contacts. Regular exchanges in terms of interdisciplinary panel meetings and working groups stimulated knowledge transfer, leading to greater specialization of general neurologists and therapists in PD. The progressive density of the network from 0.136 to 0.279 illustrates the growing cooperation of PNM + partners. Interviewed partners requested more patient-specific collaboration but expected this to happen as the network evolved. Overall, PNM + has already improved both diagnosis and therapy thanks to knowledge transfer. Structured treatment recommendations helped to improve communication between healthcare professionals.
Conclusion:
PNM+ stimulated exchange between different healthcare professionals involved in the treatment of PD patients. This overcomes specific barriers within Germany’s highly fragmented healthcare system, such as the lack of communication between these disciplines.
Keywords
INTRODUCTION
Parkinson’s disease (PD) is the second most common neurodegenerative disorder [1]. It is characterized by a progressive course, which includes both motor and non-motor symptoms [2]. Currently, over 6 million people worldwide are living with PD [3]. The incidence of PD is expected to increase over the next 10 years [4]. Additionally to pharmacological treatment options, non-pharmacological therapies such as physiotherapy, occupational therapy, and speech and swallowing therapy play an important role [5].
Today, multidisciplinary network approaches, including all healthcare professionals that are closely involved in a community-care setting, are believed to contribute to optimal care for chronic neurological disorders [6]. First available evidence suggests that integrated care models have the potential to effectively address the specific needs of PD patients and can improve their health-related quality of life compared to standard care [7].
A care network can be described as a composition of social relations among different service providers in the healthcare system. Network relations presume that coordination among service providers is based on mutual benefit, reciprocity, and confidence [8]. The solidarity within a network brings about positive effects on the treatment coordination. At the same time, improved coordination can lead to lower resource utilization within the healthcare system and enhanced health-related quality of life [9, 10].
The Netherlands was one of the first countries to implement a nationwide PD network: ParkinsonNet manages a multidisciplinary approach, patient-centered, and coordinated care. Its key components are evidence-based treatment guidelines, a focus on non-pharmacological therapies, regular training of participating network partners, supporting neurologists in referrals to therapists, and improved communication through a shared platform [11]. Internationally, there is a growing trend to implement regional PD networks [12, 13].
In the case of PD, care concepts have developed dynamically recently [14, 15]. The German Society for Parkinson and Movement Disorder (DPG) has initiated a nationwide network structure that aims to facilitate regional differences in areas of Germany [16]. The challenge is to provide PD outpatient care within a healthcare system that has traditionally focused on general neurologists or general practitioners in the outpatient setting and acute hospital admissions. Moreover, the healthcare landscape in Germany is dominated by a fragmented system of diverging processes and reimbursement mechanisms leading to inadequate cooperation and barriers between service providers [17].
A problem repeatedly identified in PD treatment is insufficient communication between healthcare professionals, e.g., physicians and therapists, especially between outpatient and inpatient care [18]. Today, several initiatives exist in Germany to build care networks for PD patients [15]. Parkinson’s Network Münsterland + (PNM+) is an already established interdisciplinary network with a particularly wide variety of medical and non-medical professions involved in the treatment of PD patients: neurologists, physiotherapists, occupational therapists, speech-language pathologist, psychologists, PD nurses, healthcare and nursing staff, PD assistants, staff of medical supply stores, and pharmacists. In addition to the professionals, PD patients and their relatives also take a part in the network. The network currently comprises a total of 156 members and 70 institutions. The network was founded according to the principles of a bottom-up approach. All network partners contributed to the main components of the network equally [19].
The aim of the study was to evaluate the connectedness among healthcare professionals involved in PD treatment, to explore perceived team performance and to identify barriers and facilitators of the interdisciplinary and cross-sectoral collaboration two years after forming PNM+. It covers a wide spectrum of different healthcare professions to describe the level of interaction between all those involved in the care process, e.g., from the neurologist to the pharmacist to the employee of the medical supply store. It is the first analysis of its kind in such a highly fragmented healthcare system as Germany’s.
MATERIALS AND METHODS
Study design and population
The network is located in the Münsterland, a rural area in the north-west of Germany, with a population of approximately 1.6 million inhabitants. Currently, there are about 7,173 PD patients living in this area [20, 21] whose treatment is ensured by an outpatient setting with 112 neurologists and an inpatient setting with one university hospital, seven acute care hospitals, and two rehabilitation clinics [21–23].
A social network analysis was conducted using a sequential mixed methods design involving quantitative and qualitative methods. In this two-phase design, we performed quantitative data collection via an online survey first and qualitative data collection via semi-structured interviews second. For the evaluation, 79 healthcare professionals of PNM+, who played an active role in the establishment of the network, were recruited. We operationalized this active role as regularly, at least semiannually participating in the network in the form of written and/or oral PD-related contribution. These PNM+ partners were practicing healthcare professionals from various medical and non-medical professions, who were based in either inpatient or outpatient settings. The Medical Ethics Committee of the University of Münster approved the study protocol (2019–428-f-S).
Measures
Social network analysis
All 79 PNM+ partners were asked to complete a structured questionnaire [25] via online survey over a 2-month period; an email reminder was sent to non-responders. The questionnaire listed all names of the professionals in the network. PNM+ partners were asked to tick a response box for each name indicating whether they knew this person and another response box to point out whether they had yet been involved in professional contacts with this person. If neither was the case, they could tick the box for unknown. In analogy to a social network analysis of the Dutch ParkinsonNet [25], knowing each other was described as “knowing the face, having talked to each other, or having heard of”. Having professional contact was characterized as “having had professional contact about at least one patient with PD who you are treating (including referral letters, emails, telephone contact, team meetings)”. The questionnaire also consisted of questions regarding health profession, experiences in the treatment of PD patients, number of PD patients treated in one year and membership of PNM+.
Team effectiveness
Another part of the structured online questionnaire included questions about the perceived team effectiveness. All 79 PNM+ partners were asked to complete the questionnaire, which contained three subscales: effectiveness of teamwork, team processes and psychosocial team characteristics. The questionnaire listed 22 questions of the original “Integrated Team Effectiveness Instrument” [26] and the “Integrated Team Effectiveness Model” [27]. Every question could only be answered once and on a scale from “not true at all” to “completely true”.
Semi-structured interviews
For the qualitative part of the study, 15 PNM+ partners were asked to participate in telephone interviews of which 10 agreed and took part (20–33 min). From all partners those involved in diagnostic and/or therapeutic treatment of PD patients were selected. They were grouped based on their profession (neurology, neuropsychology, PD nursing, physiotherapy, occupational therapy, and speech-language therapy) and on their application area (outpatient/inpatient setting). Participants were drawn at random from the groups, respectively one from the outpatient and one from the inpatient setting.
PNM+ partners were asked about their motivation to participate, their initial expectations and experiences and ratings as well as the communication and collaboration within the network and ideas for improvement.
The interview guide was pilot tested, and all interviewees gave their written consent. All interviews were audiotape-recorded and transcribed verbatim. Please see the supplementary material for the interview guide and the coding system.
Data analysis
Social network analysis
The results from the online survey were entered into squared data matrices: one for “knowing each other” and one for “having professional contact”, with the partners in the rows and columns, and values in the cells to indicate presence (1) or absence (0) of a connection. After calculating the reciprocity, we replaced the missing values of non-responders with the information about the connection provided by other partners. If no replacement was possible, missing data was replaced with 0. We analyzed the network in terms of the density and reciprocity of its connections as well as the centralization within the network. All analyses were carried out separately for the network “knowing each other” (Net 1) and for the network “having professional contact” (Net 2). Both networks were analyzed according to the influence of the attributes setting (outpatient/inpatient), district and profession. UCINET6 [28] was used for social network analysis.
Team effectiveness
The response options of each question from the online survey were transformed in a 5-point-likertscale with 0 for “not true at all” to 5 for “completely true”. Negatively worded questions were mirrored. Afterwards a descriptive analysis was conducted, and an average overall team performance score was calculated, as well as an average for the subscale scores for effectiveness of teamwork, team processes and psychosocial team characteristics. The overall team performance score and subscales ranged between 0 and 5 points, with a higher score indicating a higher level of team performance. For the overall team performance, a sum score between 0 and 110 points was calculated. SPSS version 1.0.0.–1401 was used for the analysis.
Semi-structured interviews
To interpret the interview transcripts, qualitative content analysis according to Mayring [29] was used. Qualitative content analysis is a method for systematically describing the meaning of qualitative data. This is done by assigning successive parts of the material to the categories of a coding frame. In this case, the coding process was performed using the intercoder reliability to identify a final set of codes. In doing so, a thematic structuring and description of the material was enforced [29, 30]. MAXQDA© 2018 was applied.
Triangulation
A sequential explanatory mixed methods design was performed. For this, the social network analysis or respectively the analysis of integrated team effectiveness was conducted as quantitative part. This was followed by semi-structured interviews as a qualitative part to complete and explain the results (Fig. 1). Findings were not compared until the interpretation stage, giving equal weight to all types of data. The results of the quantitative and qualitative measurements were combined within the framework of triangulation. This way, findings from the social network analysis could for example be contextualized by comparing them to findings from the interviews.
Sequential explanatory mixed methods design (adapted from Nicolau et al., 2017 [42]).
RESULTS
Social network analysis
In total, 67 of 79 health professionals provided information on their connections within PNM+, representing an 85% response rate. Non-responders included five neurologists, two physiotherapists, four speech-language pathologist and one Parkinson nurse. Partners who participated in the survey had been members of PNM+ for an average of 12 to 24 months.
Ten different professions were represented in the network, with 27 speech-language pathologists comprising the largest group (Table 1). About half of the outpatient speech-language pathologists specialize in dysarthria, the other half in dysphagia. On average PNM+ partners were 45 years old. The majority of PNM+ partners worked in their profession for 5 to 20 years. Most had been working with PD patients for 10 to 20 years. Almost half of the partners work in outpatient settings (n = 38). The other half work in inpatient settings (n = 32) or in health care supply (n = 9). The majority (n = 38) is located in the city of Münster [M], followed by the district of Steinfurt [S] (n = 18) and the district of Warendorf [W] (n = 10) (Fig. 2).
Characteristics of the network
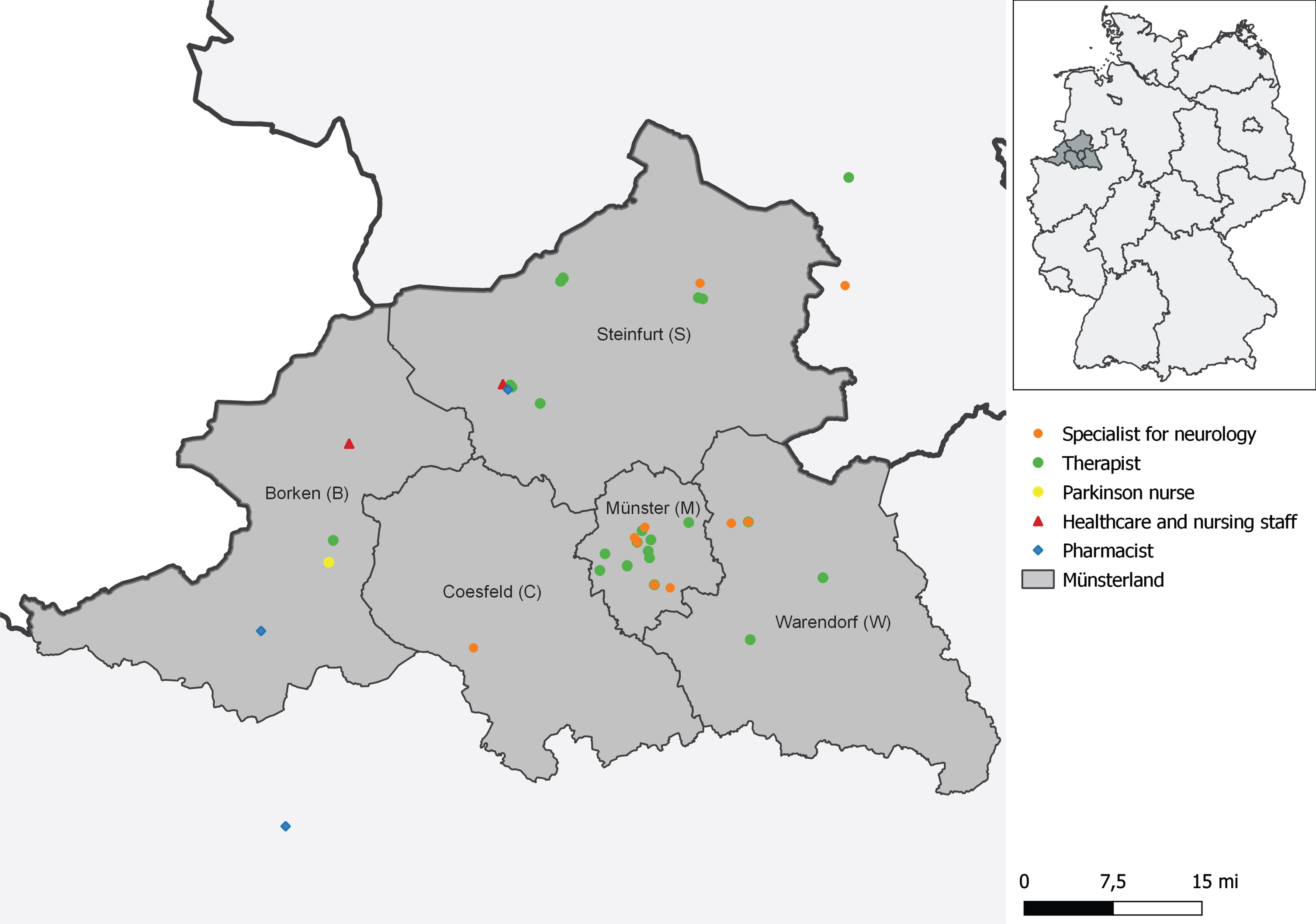
The geographical positioning of the Münsterland in the western part of Germany (map base by GADM) [31].
Net 1 has 1,741 connections out of 6,162 possible connections and a quite high reciprocity of 0.512. By contrast, the density of the network is rather low at 0.279 based on the definition of “knowing each other” and suggests that information tends to spread slowly in the network. At individual level, the network partners have a mean of 21.3 outgoing and incoming connections. Considering that each partner could have 78 connections, this number is rather low. In the current case, the out-degree graph centralization is 36.8% and the in-degree graph centralization 30.3%, this demonstrates the degree of inequality in our network (Table 2). Net 2 has 847 connections and a reciprocity of 0.522. The density of 0.136 is very low and suggests that information is distributed very slowly within the network. On average, the partners have 10.2 outgoing and incoming connections. This is even lower than in Net 1. In contrast to Net 1, Net 2 has a very high out-degree centralization (75.0%) and a much higher in-degree centralization (54.3%). Therefore, we assume that Net 2 is highly concentrated, few partners have a lot of influence and thus the impact as well as the opportunities in the network of the individual partners are distributed very differently. Both networks tend to be highly concentrated with a few central partners with high influence (Fig. 3).
Connectedness of Net 1 and Net 2
*Reciprocity: Relation between the number of connections that are reciprocal and the actual number of existing connections. If everyone would state to know each other the reciprocity would be 1 or 100%. †Density: Proportion of all possible connections that are present, if there is a complete network in which everyone is connected, the density would be 1 or 100%.‡Degree centrality: In terms of individual stakeholders, degree centrality describes the position within the network and the “power” of the individual healthcare professional. A distinction is made between the number of incoming (indegree) and outgoing (outdegree) connections. In relation to the whole network, this can show how centralized it is or how unequal the distribution of centrality is. Outdegree/Indegree centralization of the network expresses the degree of inequality or variance in the PNM+ as a percentage of a perfect star-shaped network of the same size. Outdegree/Indegree describes the average degree of inequality between stakeholders and refers to the average incoming and outgoing connections [41].
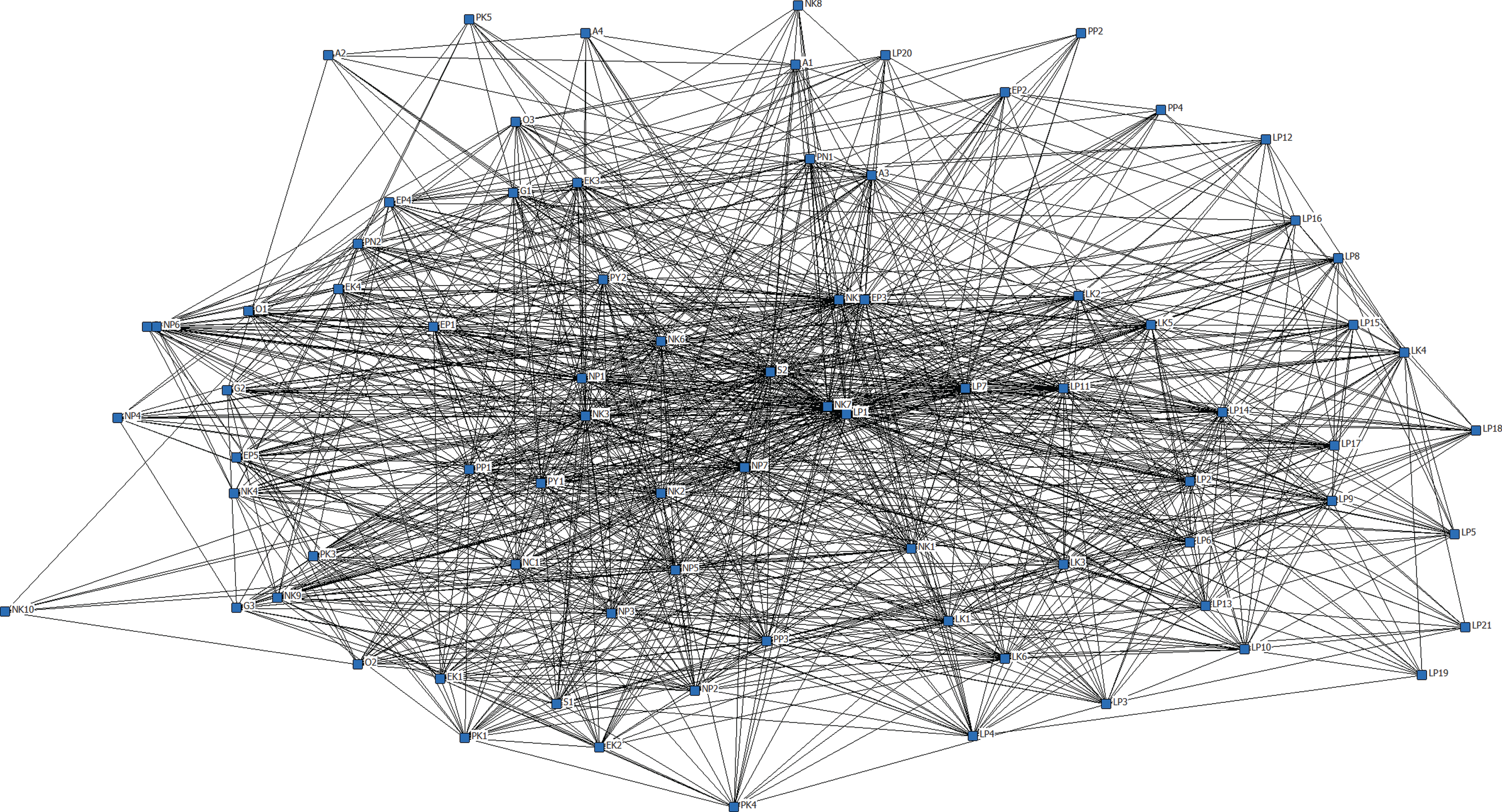
The total network of connections between healthcare professionals.
In Net 1 the density between the outpatient and inpatient settings is higher overall than in Net 2. It should be emphasized that the density (0.282) from the outpatient setting to the inpatient setting is higher than in the outpatient setting itself (Table 3). This suggests that the professionals from the outpatient setting were personally better acquainted with professionals from the inpatient setting than with professionals from the outpatient setting. Measured by the density of 0.625, neurologists collaborated well among themselves. Information on the density within the other professions can be found in the supplementary material. Starting from the neurologists, the density to the therapists varies between 0.181 to 0.288 and was rather low. From therapists to neurologists, the density varied between 0.305 to 0.392. This indicates that therapists are more likely to know neurologists personally than vice versa.
Attributes of setting and profession in Net 1 and Net 2
*The brackets indicate the density of the reversed connection.
Net 2 shows low density (0.124) in both inpatient and outpatient settings, indicating little to no exchange between outpatient and inpatient setting. In the inpatient setting, the density is 0.258, implying a relatively low professional exchange within the inpatient setting. In the outpatient setting, the density is even lower at 0.115. The professional exchange between neurologists and therapists was rather low, with a density between 0.105 and 0.131. In principle, there is a higher density when the professional exchange originates from the therapists. Except for the professional exchange between neurologists and physiotherapists, the density was higher on the part of the neurologists (0.124 vs. 0.085). Looking at the density for individual professions, it was comparatively higher than between professions, but also rather moderate with a peak value of 0.393 for neurologists. Assessed by the presence of density and not by its value, neurologists were in professional exchange with all other professions.
Team effectiveness
The team effectiveness questionnaire was completed by 66 partners (84.0%). PNM+ reached an average overall score of 70 out of 110 possible points. In terms of a score from 0 to 5 points PNM+ achieved 3.2 points on average, indicating a moderate perceived team performance. All three subscales ranged in a moderate value. With an average of 3 points, the subscale team process achieved the lowest score. The highest score, with an average of 3.4 points, was achieved in the subscale psychosocial team characteristics, followed by an average value of 3.3 in the subscale teamwork. Areas that were rated particularly well were knowledge enhancement through the Parkinson’s network (4.16 points), the respect and appreciation in the network (4.11 points) as well as the open communication (4 points) and the trust they have in the expertise of each other (4 points).
Semi-structured interviews
PNM+ partners stated their expectancies towards the network as a faster exchange with other professional groups as well as insights into their work. Both expectations were met, e.g., at the quarterly multidisciplinary panel meetings. The partners considered these meetings to be the most important platform for professional exchange within the network, allowing them to talk in depth about symptomatology and treatment methods with the aim of providing patient-oriented care.
Much of the work within PNM+ takes place in working groups. These are thematically (e.g., dysphagia) or disciplinary (e.g., speech therapy) formed. As one therapist (outpatient setting) explicated, these groups help him stay informed about innovative patient-centered care options.
Overall, therapists use the network on a more regular basis than physicians. Both physicians that participated in the interviews said they could not participate more intensively because they lack the time.
When questioned about if and how PNM+ had helped them, the partners mentioned instances of optimized care through increased interdisciplinary collaboration. They said that the network has enabled them to learn from each other and widen their horizons. E-learnings on PD treatment, that were provided during the Covid pandemic, were seen as very valuable by many respondents. When asked about less helpful aspects of the network, only two partners reported anything: One wished for psychotherapeutic treatment, the other for nutrition to play a more central role.
At the time of the interviews, communication within the network took place mainly with colleagues from the same discipline. More interdisciplinary interaction within the clinics than between inpatient and outpatient setting was reported. However, inpatient-outpatient communication was intensified by PNM+, as one therapist (clinical setting) stated. Most partners indicated that the network has already augmented communication and that this should be encouraged even more in the future. They were satisfied with the communication within the network.
Collaboration within the network was at the time of the study limited to general topics and less specific to patient cases. PNM+ partners expected the patient-oriented collaboration to be strengthened in the further development of the network.
When asked about their ideas for improvement, the partners mentioned further strengthened interdisciplinary communication, a greater exchange of knowledge and more patient-specific work. Some partners thought that these points will be put into practice once guideline-based recommendations for therapy are used. Others proposed to include other professional groups in the network, such as general practitioners.
Most network partners concluded that the network has increased communication and collaboration between different disciplines and helped to optimize both diagnosis and therapy of patients.
Triangulation
Social network analysis and team effectiveness as well as interview data suggest increased collaboration in the network compared to standard care. Simultaneously, data from the online survey on team effectiveness as well as the interviews confirm that the exchange stimulates knowledge transfer, which subjectively leads to greater PD specialization among general neurologists and therapists. So far, the exchange of knowledge during regular meetings has been on a general level and did not refer to specific patients. In addition, both team effectiveness and interview data indicated that team processes need to be improved. The interview data affirmed findings from the social network analysis: there was more communication within the same disciplines and clinics than interdisciplinary and between inpatient and outpatient setting. Nevertheless, the network has already enabled healthcare professionals, especially in the outpatient setting, to get to know each other better.
DISCUSSION
This evaluation examined the collaboration between healthcare professionals involved in the treatment of PD patients within a network approach. A special focus was put on the connectedness between neurologists and therapists as the largest professional groups in the network. The main findings of the study were 1) increased collaboration between professionals visibly due to the density of PNM+, caused by quarterly multidisciplinary panel meetings and working groups, and 2) improved communication associated with disease-specific knowledge growth reflected in structured therapy recommendations. When interpreting the results, it is important to keep in mind that we conducted a cross-sectional study, which is only a snapshot of a specific point in time and therefore participants compared their experiences with PNM+ to existing standard care.
Collaboration in PNM+ is facilitated through regular multidisciplinary panel meetings and corporate working groups resulting in high density of the network “knowing each other”. The density of the network “having professional contact” is not as high as of the network “knowing each other”. One reason might be the geographical distribution of partners making a professional collaboration more difficult, e.g., between PNM+ partners of the urban center of Münster and rural areas (Fig. 2). Experiences from the daily practice of PNM+ partners show that many PD patients prefer treatment close to home. As our study shows, professionals often have more connections within their own individual network close to home or geographical area. To overcome this shortcoming, PNM+ is currently working on telemedicine solutions that have been developed and strongly recommended for PD care in recent years [32].
Additionally, physicians are often accustomed to exchanging knowledge and discussing patients with other physicians. Such disease-specific exchange typically does not exist in Germany between neurologists and therapists or within therapists themselves due to the highly fragmented healthcare structure. The high participation level of therapists within PNM+ implies a great deal of interest in professional exchange and the need for corresponding structures. Our analyses have shown that the PD network structure enables therapists to initiate communication with neurologists to overcome this deficit of the German healthcare system. Collaborating in topic-specific working groups (e.g., patient education, non-motor symptoms, innovative technologies) has strengthened communication within professions as well as interprofessionally. Additionally, the network promotes exchange with professions outside of the focus of this study, such as pharmacists or employees of medical supply stores. As a conclusion, such working groups may be a suitable approach for highly fragmented healthcare systems to reduce communication barriers.
Even though international studies have shown that non-pharmacological therapies are effective in PD treatment [33–35], these therapies are infrequently prescribed in Germany [20, 36]. If they are prescribed, referrals do not contain any specific information. To remedy this situation, PNM+ partners developed guideline-based therapy recommendations in the form of so-called “Quickcards” [19]. Up to now, there are ten different Quickcards: dysphagia, dysarthria, sialorrhea, physical therapy, occupational therapy, assessments, medical aids, sleep disorders, medication lists, fitness to drive, and device-aided treatment strategies. These Quickcards have been developed with the know-how of all PNM+ partners [19, 37]. This increased the partners’ knowledge and expertise regarding the treatment of PD patients. The Quickcards also improve communication among all healthcare professionals regarding PD treatment.
PNM+ is oriented towards the Dutch model “ParkinsonNet”, which has revolutionized PD care [38], but also considers specific aspects of the German healthcare system and local needs. Like ParkinsonNet, different healthcare professionals are collaborating. The analysis of ParkinsonNet ten years ago included 104 partners. In the network “knowing each other” analysis showed 1,431 connections, a reciprocity of 0.630, a density of 0.142 and an outdegree centralization of 21.1% as well as an indegree centralization of 25.1%. The network “having professional contact” had 664 connections, a reciprocity of 0.479, a density of 0.006 and an out- and indegree centralization of 16.6% [25]. Due to its similarities, PNM+ also shows a similar number of connections and a similar degree of reciprocity, compared to the ParkinsonNet at the time of its first social network analysis, but with an even higher density. Furthermore, outdegree and indegree centralization in both networks (Net 1 and Net 2) is higher than in the ParkinsonNet analysis ten years ago. This might be an achievement of the PNM+ steering committee, which consists of the initiators and the speakers of the working groups that are most prominently represented in the network. Yet, a new ParkinsonNet analysis would surely show far better results due to its outstanding success in recent years [39].
In many aspects, the challenges of PD care are similar in the Netherlands and Germany: fragmentation, inadequate interdisciplinary collaboration, and a lack of timely access to therapies [6]. Nevertheless, ParkinsonNet and PNM+ can only be compared to a limited extent, as they are based on various healthcare systems, e.g., with different access to healthcare. In the Netherlands, treatment is provided by general practitioners as gatekeepers (primary care) and is supplemented by specialist care in hospitals (secondary care) [40]. In Germany, however, general neurologists work in their own medical office, like general practitioners. This highlights the fact that the specifics of each healthcare system or even certain regions within a country and its consequences for PD care should be analyzed in terms of their specific needs before a network can be implemented.
Due to missing reference values, standards, and specifics of each network, the results of a social network analysis must always be interpreted according to the setting in which the network is located. PNM+ enables an exchange between different healthcare professionals involved in the treatment of PD patients in the otherwise fragmented German healthcare system with separated care settings. The high participation rate in the presented evaluation underlines the exceptional motivation of PNM+ partners and the commitment in building a network that creates new structures to improve the treatment of PD patients. PNM+ continues to grow as more professions from PD care join. This shows that there is a need for networking between different stakeholders in PD treatment who share the ambitions of PNM+. Hence, it can be assumed that the results are transferable to all PNM+ partners, even though some are still underrepresented in the current analysis. One limitation is the limited generalizability of the results, which are restricted to health care professionals participating in an early-stage and disease-specific regional network. Another limitation is the degree of relationship of the PNM+ partners, which can vary from “knowing the face” to, “having talked to each other” to “having heard of”. This definition of “knowing each other” can make relationships seem closer than they really are. In the study, this was countervailed by triangulation, e.g., comparing interview results to social network analysis results. Future research should focus on longitudinal data and analyses of differences between Parkinson’s networks in different areas of Germany. Furthermore, patient reported outcomes should be measured to further anchor these networks in PD standard care.
Footnotes
ACKNOWLEDGMENTS
We thank all PNM+ partners for participating in both the online survey and the interviews. We acknowledge support from the Open Access Publication Fund of the University of Münster.
We state that procedures involving experiments or surveys on humans is in accordance with the ethical standards of the Medical Ethics Committee of the University of Münster and the Helsinki Declaration. No procedures involving experimentation on animal subjects were performed.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.