
Abstract
Background:
Emerging evidence has indicated the positive effects of repetitive transcranial magnetic stimulation (rTMS) on patients with Parkinson’s disease (PD) for the treatment of mild cognitive impairment (MCI).
Objective:
Investigating whether combining virtual reality (VR) training with rTMS can further enhance cognitive improvement induced by rTMS treatment.
Methods:
We randomly assigned 40 patients with PD and MCI into three groups, namely the rTMS-VR group (n = 13), rTMS group (n = 11), and sham rTMS group (n = 16). rTMS was administered as 10 consecutive sessions of intermittent theta burst stimulation (iTBS) over the left dorsolateral prefrontal cortex. In the rTMS-VR group, VR training was administered immediately after each rTMS session. Cognitive function was measured using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) and Montreal Cognitive Assessment (MoCA) at baseline, immediately after intervention, and at 3-month follow-up.
Results:
Compared with the rTMS group, the rTMS-VR group exhibited significantly more improvements in total and delayed memory scores of the RBANS and the visuospatial/executive function score of the MoCA after intervention (p = 0.000∼0.046) and the delayed memory score of the RBANS at 3-month follow-up (p = 0.028).
Conclusion:
The integrated rTMS-VR protocol achieved a superior outcome in global cognitive function, more effectively enhancing working memory and visuospatial executive function than did the rTMS protocol alone. The combination of VR and rTMS can be an effective regimen for improving the cognitive function of patients with PD.
INTRODUCTION
Parkinson’s disease (PD) is a common neurodege-nerative disease characterized by motor dysfunction and early cognitive impairment in some patients. Major cognitive impairment affects executive function, visuospatial perception, abstract thinking, memory, and speech fluency, which can severely reduce the quality of life [1, 2]. Mild cognitive impairment (MCI) is observed in 19%–38%of patients with PD [3]. The risk of dementia is five times higher in patients with PD than in the healthy population [4]. Although some pharmacological and physical therapies may improve cognitive functions [5–7], their effects are usually limited. Therefore, the development of cognitive intervention strategies, such as noninvasive neurostimulation (e.g., repetitive transcranial magnetic stimulation (rTMS) [8, 9]) and virtual reality (VR) [10], has attracted the attention of researchers.
The pathophysiology of cognitive impairment in PD remains unclear. Changes in the levels of neurotransmitters such as acetylcholine and dopamine can be a possible mechanism [11]. rTMS, a novel noninvasive treatment, could ameliorate cognitive dysfunction in patients with PD [8, 9]. Theta burst stimulation is a newly developed patterned rTMS protocol that exerts a long-lasting neuromodulatory effect [12]. Prefrontal intermittent theta burst stimulation (iTBS) could improve the working memory [13] and executive function [14] of healthy individuals. However, studies investigating the translational effects of rTMS on the cognitive function of patients with PD have reported mixed results because of the heterogeneity of the stimulation protocol (e.g., targeted brain area, stimulation intensity, and total treatment sessions). Table 1 lists the published studies of rTMS for the cognitive rehabilitation of patients with PD. A meta-analysis indicated that multiple sessions of rTMS over the dorsolateral prefrontal cortex (DLPFC) substantially improved the global cognitive and executive functions of patients with PD [8]. To enhance the efficacy of iTBS, we previously applied 10 consecutive sessions of iTBS over the left DLPFC of patients with PD and MCI [15]. Compared with the sham group, the intervention group exhibited significant improvements in global cognitive function.
Studies on rTMS and VR for cognitive function of patients with PD
rTMS, repetitive transcranial magnetic stimulation; VR, virtual reality; RCT, randomized controlled trial; PMd, dorsal premotor cortex; DLPFC, dorsolateral prefrontal cortex; PD, Parkinson’s disease; MCI, mild cognitive impairment; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; MoCA, Montreal Cognitive Assessment.
VR is a technological tool involving the use of a three-dimensional computer-generated environment for detecting the actions and positions of the user while providing a sense of presence within the environment [16]. Interactions with virtual objects allow the user to perceive multisensory feedback (e.g., visual, auditory, and kinesthetic) resembling that received in real life. Compared with traditional cognitive training, VR provides a more engaging experience with the inclusion of cognitive tasks and realistic settings simulating daily activities [17]. VR could effectively improve the cognitive function of patients with mild cognitive impairment or dementia [18–20], stroke [21], multiple sclerosis [22], traumatic brain injury [23], and attention-deficit hyperactivity disorder [24]. Cognitive enhancement through VR training can potentially promote neuroplasticity and activate functional connectivity [25]. Rehabilitation with VR could improve the gait, motor function, activities of daily living (ADL) [26], and executive and visuospatial abilities of patients with PD [27] (Table 1).
Emerging evidence has indicated the potential therapeutic effects of rTMS in combination with exercise training for motor rehabilitation [28–31]. Studies have reported that the priming effects of rTMS in terms of increased cortical excitability may enhance the effects of subsequent exercise training, leading to increased motor recovery in patients with stroke [31] and multiple sclerosis [28]. The integration of noninvasive brain stimulation (NIBS) and VR was evaluated in different clinical contexts [32, 33]. Compared with exercise or transcranial direct-current stimulation (tDCS) alone, VR wrist exercise following tDCS resulted in higher and more sustained corticospinal excitability in patients with stroke [34]. These results indicate that the combination approach can promote rehabilitation outcomes. Compared with patients with Alzheimer’s disease (AD) receiving sham treatment, those receiving concurrent rTMS and traditional cognitive training exhibited significantly improved performance in several cognitive tasks [35]. Mancuso et al. proposed and discussed the concept of the integration of rTMS and VR for the cognitive rehabilitation of patients with MCI [36]. The underlying rationale is based on the Hebbian theory of neuroplasticity [37], according to which synaptic reinforcement can be induced through the simultaneous activation of the same neural networks. According to this theory, VR training can provide multisensory simulation that may enhance the Hebbian plasticity elicited by rTMS. Stimulation of the prefrontal cortex by rTMS may activate and enhance the efficiency of neural circuits responsible for executive function and memory, which are also involved in the accomplishment of VR cognitive tasks [36]. The integration of rTMS and VR can modulate impaired neural circuits in a complementary manner, thus exerting beneficial effects on cognitive rehabilitation [36].
Considering that both VR and rTMS can improve cognitive function by addressing the neuronal and behavioral aspects of cognition effects, the integrated approach may allow a more sensitive rehabilitation of the cognitive symptoms of patients with PD. Based on the positive results of the combination of NIBS and VR treatment for motor and cognitive functions, we hypothesized that the integration of VR training into rTMS can enhance cognitive improvement induced by rTMS in patients with PD and MCI. Although the effects of rTMS on patients with PD and MCI have been explored, its effect is yet to be confirmed when compared with the widely studied VR-based treatment. Therefore, we conducted an rTMS-based randomized controlled trial (RCT) by including a sham rTMS group. We investigated the short- and long-term effects of the integrated protocol with a VR-complemented rTMS training system on the cognitive function of patients with PD.
MATERIALS AND METHODS
Design
This was a randomized controlled, single-blind study. The randomization order was computer generated and concealed in sequentially numbered opaque envelopes by an independent statistician. A total of 48 patients were randomly assigned to an rTMS-VR (n = 16), rTMS (n = 16), or sham (n = 16) group. Every participant received sham or real stimulation over the left DLPFC for 10 sessions across 10 consecutive weekdays. For VR cognitive training, we employed the HTC Vive (HTC Corporation, Taipei, Taiwan) head-mounted VR display system. The rTMS-VR group were administered a 40-min VR program immediately after each iTBS intervention. In terms of the dropout rate, three patients withdrew from the rTMS-VR group due to a medical condition, five patients withdrew from the rTMS group (three because of family issues and two because of COVID-19 concerns), and no patient withdrew from the sham group (Fig. 1).

Study flowchart.
Participants
Patients with PD and cognitive impairment who visited the outpatient clinic of a tertiary medical center were surveyed. The patients were screened for study eligibility based on their subjective cognitive impairment. Inclusion criteria were as follows: 1) having an established diagnosis of PD based on the Parkinson’s UK Brain Bank Society criteria for idiopathic PD [38] provided by a neurologist specialized in movement disorders; 2) receiving a stable dosage of medication for PD throughout the study period; and 3) having cognitive impairment fulfilling the diagnostic criteria for PD and MCI, which was defined using the Movement Disorder Society Task Force Level II criteria [1] as follows: I) a gradual decline in the cognitive ability reported by the patient or informant or observed by the clinician; II) performance approximately 1 to 2 standard deviations below appropriate norms, as observed in either two impairment tests in one cognitive domain or one impairment test in two cognitive domains in a formal, comprehensive neuropsychological test [1]; and III) cognitive deficits that do not significantly interfere with functional independence. Exclusion criteria were as follows: 1) a diagnosis of dementia or other degenerative brain disease; 2) metallic intracranial devices, pacemakers, or other electronic devices in their bodies; 3) an unstable medical condition; 4) a history of seizure; and 5) concurrent use of antidepressants or neurostimulators. The rTMS protocol used in this study was in accordance with safety guidelines for rTMS applications [39].
Of the 72 participants assessed for eligibility, 14 did not meet the inclusion criteria and 10 declined to participate (Fig. 1). This study was approved by the Institutional Review Board of Taipei Veterans General Hospital, and all patients provided written informed consent before participation.
Intervention
Determination of the resting motor threshold
We applied rTMS by using the Magstim Rapid2 stimulator, which was connected to a Dantec Keypoint Focus electromyography machine (Natus Medical Incorporated, CA, USA) to record motor-evoked potential signals. The amplified (100–1 mV/div) and bandpass-filtered (20–2000 Hz) signals were digitized at a sampling rate of 20 kHz. The patients were asked to sit relaxed in a chair with their eyes open. The figure-of-eight coil was systematically placed (for mapping) on a 1-cm scale over the motor cortex until the largest consistent motor-evoked potential response was recorded from the contralateral first dorsal interosseous muscle. The resting motor threshold for this muscle was defined as the minimal intensity that elicits a motor-evoked potential of at least 50 mV in 5 of the 10 consecutive sessions [1]. The measurement procedure was identical to that described in our previous study [40].
Stimulation protocol
Each participant received one session of iTBS every week day for 2 consecutive weeks for a total of 10 sessions. The DLPFC is a key structure involving the cognitive corticostriatal network, and decreased activity in the prefrontal cortex is associated with low cognitive performance in patients with PD and MCI [41]. Based on this rationale, we localized the stimulation site at the left DLPFC as the F3 point of the international 10/20 electroencephalography recording system. The iTBS intensity was set at 90%of the resting motor threshold. The iTBS treatment consisted of three pulses of 50-Hz bursts repeated at 5 Hz (2 s on and 8 s off) for a total of 190 s (600 pulses). For sham stimulation, we used a placebo coil (Magstim) that delivered < 5%of the magnetic output with an audible click on discharge. None of the participants had undergone rTMS before; hence, they were not aware whether they were receiving real or sham rTMS.
VR cognitive training protocol
The HTC Vive display system [42] was used to provide the virtual environment. This fully immersive VR system is equipped with a head-mounted display, room tracking units (infrared cameras), and two controllers allowing user interaction with the virtual environment similar to that in real life. Head rotation was tracked to detect head orientation and coordinately alter the view seen by users in the virtual environment. We designed VR-based scenarios by using the three-dimensional game engine Unity on a Windows platform.
These VR-based scenarios were designed based on ADLs, including shopping for groceries, using an ATM, and driving a car (Fig. 2). In the virtual supermarket, the participants were required to memorize items on a shopping list, navigate the supermarket to pick up items from shelves, and finally proceed to the checkout to calculate and pay the correct amount. At the virtual ATM, the participants were first required to memorize a set of passwords and an account number and to withdraw a certain amount of money displayed on the screen. In the car driving task, we provided an audio guide prompting the participants to recognize locations such as a school or restaurant. We then asked the participants to drive to a designated place and then drive back. In each scenario, the participants were asked to accomplish several cognitive tasks used to train memory, attention, visuospatial ability, and executive function, with progressive levels of difficulty (Table 6). To examine the executive function and visuospatial ability, we administered an additional trajectory tracking task that required the participants to trace the direction of the trajectory displayed on another screen (Fig. 2). In the rTMS-VR group, each participant received 40 minutes of VR cognitive training immediately after their daily iTBS session.
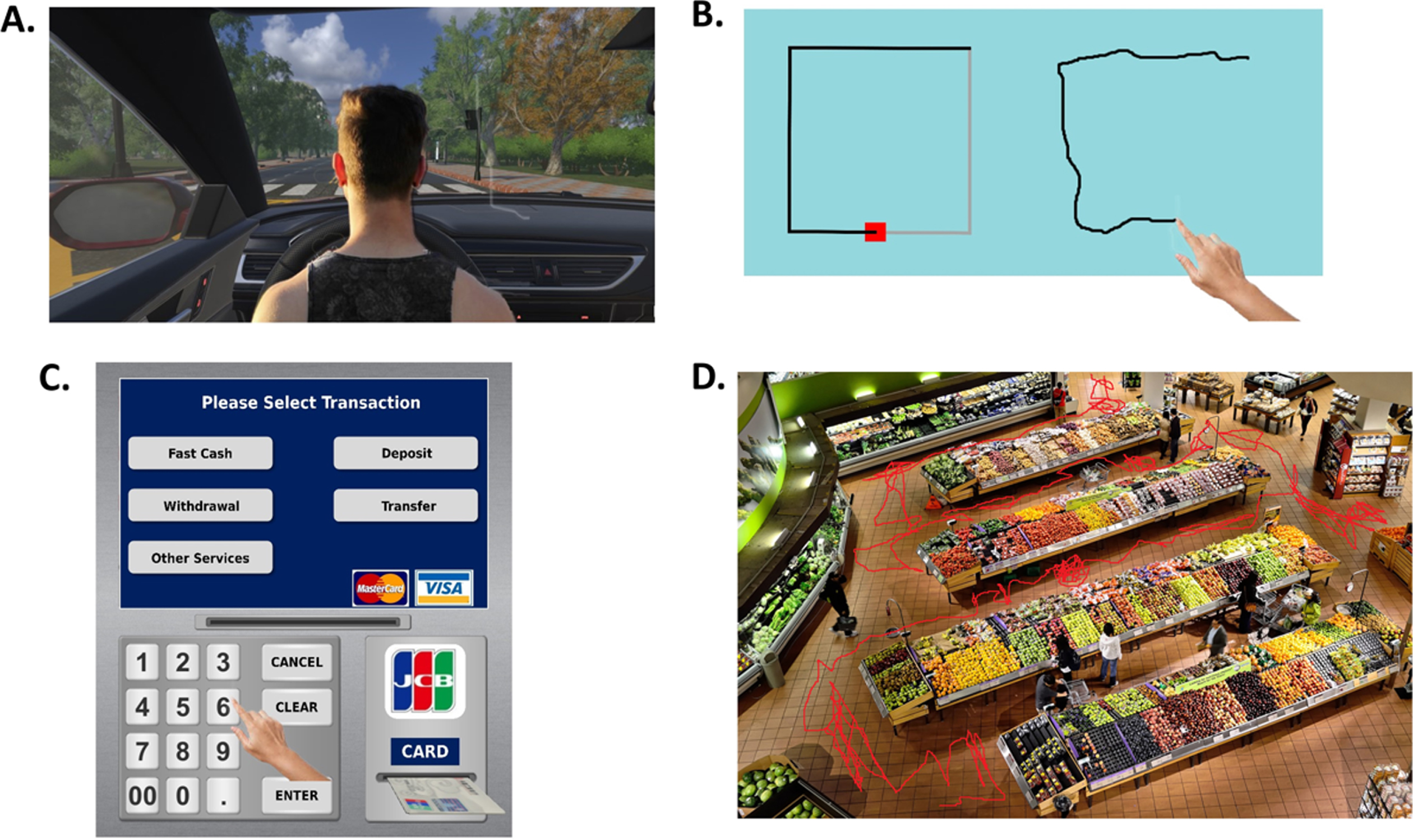
Illustration of the VR cognitive training protocol. A) Car driving: drive to a designated place and then drive back. B) Trajectory tracking: trace the direction of the trajectory displayed on the other screen. C) Virtual ATM: memorize a set of passwords and then withdraw cash of a specified amount from the ATM. D) Virtual supermarket: pick up items on a shopping list, calculate the total amount, and pay at the checkout. VR, virtual reality; ATM, automated teller machine.
VR cognitive training protocol with progressive levels of difficulty
VR, virtual reality; ATM, Automated Teller Machine.
Outcome measures
Assessment of cognitive and depressive status
A therapist blinded to the group allocation evaluated the cognitive and depressive status of all the patients prior to the first intervention session, 1 day after the completion of the protocol, and 3 months after the intervention. Assessment tools used in this study included the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS), Montreal Cognitive Assessment (MoCA) [43], and Beck Depression Inventory (BDI) [44].
The RBANS is a comprehensive assessment tool that generates five index scores for the following five neurocognitive domains: immediate memory, visuospatial abilities, language, attention, and delayed memory. The total score is calculated by summarizing the five index scores, with the average score ranging from 90 to 109 after adjustment for age; the lower the total RBANS score is, the lower is the cognitive function. The MoCA is an effective evaluation and screening test for cognitive impairment and examines the following cognitive domains: visuospatial/executive, naming, memory, attention, language, abstraction, and orientation. The scores range between 0 and 30, with high scores indicating high levels of cognitive function. For BDI scores, we used the following standard cutoff values: 1 to 10, normal; 11 to 16, mild mood disturbance; 17 to 27, moderate depression; 21 to 30, moderate depression; 31 to 40, severe depression; and 41 to 63, extreme depression.
Data analysis
We compared baseline assessments and biographic data among the groups by using one-way analysis of variance for continuous data and the chi-square test for categorical data. To determine improvements in RBANS, MoCA, and BDI scores, we employed the Wilcoxon signed-rank test for intragroup comparisons. We performed one-way analysis of variance (ANOVA) for the intergroup comparisons of changes in RBANS, MoCA, and BDI scores. For post hoc comparisons between the groups, the Bonferroni procedure was used for correction. The level of significance was set at p < 0.05. All statistical analyses were performed using SPSS version 22.
RESULTS
Demographic characteristics
Table 2 lists the patients’ demographic and clinical data. No significant difference was observed in the baseline RBANS, MoCA, and BDI scores and in the other clinical features among the groups. Moreover, no significant intergroup differences in motor impairment, ADL status, Unified Parkinson’s Disease Rating Scale scores, and medication doses were noted. During the experimental period, the patients did not experience seizures or other adverse effects. Two participants in the rTMS-VR group and one in the rTMS group experienced mild, dull skull pain in the rTMS area; the pain was relieved after the stimulation intensity was lowered by 1%to 2%of the maximal machine output. Because seven patients in the rTMS-VR group reported dizziness while using the head-mounted display, a semi-immersive mode without the head-mounted display was instead used.
Demographic data and clinical characteristics of all patients
LED, levodopa equivalent dose; UPDRS, Unified Parkinson’s disease rating scale; MBM, mentation, behavior, and mood; ADL, Activities of Daily Living; H-Y stage, Hoehn–Yahr stage; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; MoCA, Montreal Cognitive Assessment; BDI, Beck’s Depression Inventory; TMS-VR, transcranial magnetic stimulation-virtual reality; TMS, transcranial magnetic stimulation.
Group improvement
The rTMS-VR group exhibited significant increases in the total (p = 0.001), immediate memory (p = 0.034), and delayed memory (p = 0.003) scores of the RBANS and the total (p = 0.005), visuospatial/executive function (p = 0.01), abstraction (p = 0.046), and delayed recall (p = 0.01) scores of the MoCA after the intervention compared with the baseline levels. At 3-month follow-up, the changes in the total (p = 0.021), immediate memory (p = 0.017), and delayed memory (p = 0.006) scores of the RBANS and the total (p = 0.029), visuospatial/executive function (p = 0.023), and delayed recall (p = 0.028) scores of the MoCA remained significant compared with the baseline data (Table 3).
Mean RBANS, MoCA, and BDI scores in the TMS-VR group
RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; MoCA, Montreal Cognitive Assessment; BDI, Beck’s Depression Inventory; TMS-VR, transcranial magnetic stimulation-virtual reality; rTMS, repetitive transcranial magnetic stimulation. Significant differences between Post-rTMS and Pre-rTMS. *p≤0.05, **p≤0.01, ***p≤0.001. Significant differences between post-rTMS 3 months and pre-rTMS. #p≤0.05, # #p≤0.01, # # #p≤0.001.
The rTMS group demonstrated significant incre-ases in the total (p = 0.005), immediate memory (p = 0.016), language (p = 0.038), and delayed memory (p = 0.018) scores of the RBANS and the total (p = 0.005), language (p = 0.02), and delayed recall (p = 0.011) scores of the MoCA compared with the baseline levels. At 3-month follow-up, the changes in the total (p = 0.042), immediate memory (p = 0.042), and language (p = 0.042) scores of the RBANS remained significant compared with the baseline data (Table 4).
Mean RBANS, MoCA, and BDI scores in the TMS group
RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; MoCA, Montreal Cognitive Assessment; BDI, Beck’s Depression Inventory; TMS, transcranial magnetic stimulation; rTMS, repetitive transcranial magnetic stimulation. Significant differences between Post-rTMS and Pre-rTMS. *p≤0.05, **p≤0.01, ***p≤0.001. Significant differences between Post-rTMS 3 month and Pre-rTMS. # p≤0.05, ## p≤0.01, ### p≤0.001.
The sham group exhibited significant increases in the attention score (p = 0.025) of the MoCA compared with their baseline level (Table 5).
Mean RBANS, MoCA, and BDI scores in the sham group
RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; MoCA, Montreal Cognitive Assessment; BDI, Beck’s Depression Inventory; rTMS, repetitive transcranial magnetic stimulation. Significant differences between post-rTMS and pre-rTMS. *p≤0.05, **p≤0.01, ***p≤0.001.
We observed no significant differences in the BDI scores before or after the intervention among the three groups.
Intergroup comparison
Our results showed significant improvements in the post-intervention total (F [2,37] = 27.83, p < 0.001), delayed memory (F [2,37] = 9.48, p = 0.001) scores of the RBANS and total (F [2,37] = 22.25, p = 0.008), visuospatial/executive function (F [2,37] = 4.33, p =0.008), language (F [2,37] = 4.40, p = 0.021), and delayed recall (F [2,37] = 3.45, p = 0.045) scores of the MoCA among groups.
Compared with the sham group, the rTMS-VR group demonstrated significant increases in the post-intervention total (p < 0.001), delayed memory (p = 0.001) scores of the RBANS and total (p =0.012), visuospatial/executive function (p = 0.008) scores of the MoCA after correction for multiple comparisons (Fig. 3).
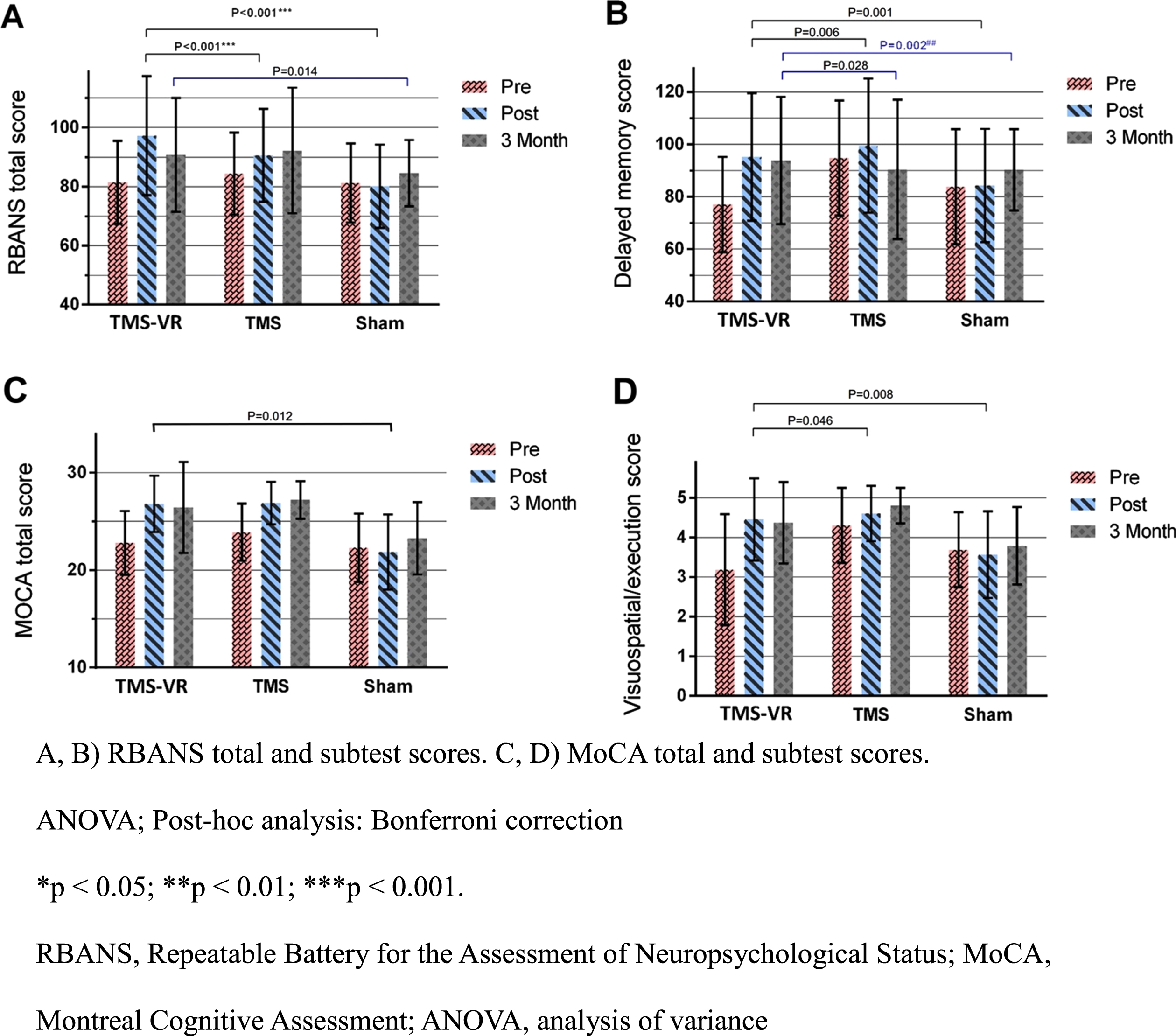
Intergroup comparisons for changes of RBANS, MoCA, and subtest scores post-intervention and at 3-month follow-up.
Compared with the sham group, the rTMS group exhibited a significant increase in the postintervention language (p = 0.024) score of the MoCA after correction for multiple comparisons.
Compared with the rTMS group, the rTMS-VR group revealed significant increases in the total (p < 0.001), delayed memory (p = 0.006) scores of the RBANS and the visuospatial/executive function score (p = 0.046) of the MoCA (Fig. 3).
At 3-month follow-up, we noted significant differences in the improvements of total (F [2,37] = 4.89, p = 0.016), delay memory (F [2,37] = 8.16, p = 0.002) scores of the RBANS and visuospatial/executive function (F [2,37] = 3.69, p = 0.039) score of the MoCA among groups.
Compared with the sham group, the rTMS-VR group demonstrated significant increases in the total (p = 0.014), delayed memory (p = 0.002) scores of the RBANS (Fig. 3).
Compared with the rTMS group, the rTMS-VR group revealed a significant increase in the delayed memory score of the RBANS (p = 0.028) (Fig. 3).
We observed no significant differences in BDI scores among the three groups.
DISCUSSION
This RCT demonstrated that the patients with PD and MCI exhibited improvements in their cognitive function in multiple domains when they engaged in a VR cognitive training program immediately after rTMS modulation. In addition to rTMS-related cognitive enhancement, the rTMS-VR group benefitted more from the VR program in terms of global cognition, delayed memory, and visuospatial executive function. Furthermore, the differential effects of delayed memory persisted for at least 3 months. With the early recognition of MCI in PD, cognitive decline could be attenuated with this intensive novel program.
Cognitive impairment in PD is associated with a pattern of subcortical deficit [45] that is characterized by executive dysfunction as a major presentation observed in the early stage. With disease progression, the additional involvement of memory, attention, and visuospatial ability can be identified. A functional neuroimaging study revealed that striatal dopamine depletion and insular dopamine receptor loss were associated with executive deficits in PD with MCI [46]. Another cohort study of patients with PD and MCI demonstrated lower dopamine uptake in the caudate nucleus and decreased recruitment in frontostriatal circuitry on functional magnetic resonance imaging (fMRI) during a working memory task [47]. rTMS of the prefrontal cortex could induce the release of endogenous dopamine in the human caudate nucleus and restore dopaminergic depletion within the frontostriatal network [48]. Therefore, we applied rTMS over the left DLPFC to improve the cognitive function of patients with PD and MCI through modulating the frontostriatal dopaminergic pathway.
Although studies have applied rTMS for attenuating the cognitive decline in PD, they have reported mixed results. The divergent results could be attributable to the heterogeneity of the stimulation protocol (i.e., variations in in paradigm, stimulation intensity, and treatment frequency) [49–51]. Two RCTs applied separate six-session iTBS with an 80%active motor threshold over the left DLPFC in patients with PD and reported significant enhancement in overall cognition after the intervention. However, no significant difference between the iTBS and sham groups was noted [49, 50]. By contrast, another RCT found that the application of 20-Hz rTMS over the bilateral DLPFC for 2 weeks did not improve cognitive function in patients with PD and MCI [51]. Overall, the effects of rTMS on cognitive enhancement may depend on the stimulation site, intensity, frequency, and number of treatment sessions. Compared with participants in the aforementioned RCTs, those recruited in our study received 10 consecutive sessions of iTBS of a higher intensity and demonstrated more significant results, implying that the dose and intensity of the stimulation affect the strength of the effects on cognitive function. A meta-analysis reviewing 14 studies published up to 2019 revealed that high-frequency rTMS over the DLPFC with multiple sessions exerted a positive effect on global cognitive function in PD [8]. Consistent with these findings, our study demonstrated significantly improved executive function in the rTMS group compared with the sham group.
Our study results indicated that iTBS over the left DLPFC significantly improved the patients’ performance in memory tasks. Immediate and delayed memory are both forms of short-term memory, which is a component of working memory that requires maintenance and manipulation of information. The working memory process is mediated by several cortical and subcortical structures including the frontoparietal network, caudate nucleus, and thalamus [52, 53]. As part of the frontoparietal network, the DLPFC is largely implicated in tasks that demand the executive retrieval of stored information [54]. The underlying mechanism related to memory enhancement involves the neuromodulatory effects of increased frontostriatal functional connectivity synchronization [55], frontoparietal theta synchronization, and parietal gamma band power [13] elicited by rTMS over the DLPFC.
A VR cognitive training program provides real-time augmented and multisensory feedback that may induce changes in neuronal plasticity through a reinforced learning process, leading to cognitive recovery [27]. Through realistic life-like multisensory experiences, VR scenarios can make participants feel immersed and interactive, which positively affects the sense of presence and memory of the environment [56]. In addition, an individual’s observation of their actions during VR training may activate the mirror neuron system, which overlaps with motor, language, and cognitive neural circuits [57], thus contributing to performance awareness and cognitive enhancement [58]. The plausible mechanisms of VR-related neuroplasticity include the rebalance of cholinergic and dopamine systems [59], enhancement of cerebral blood flow, and release of neurotrophic factors [20]. An fMRI study reported that significantly improved visuospatial function after VR cognitive training was related to increased frontal–occipital connectivity [25]. Another RCT including patients with MCI reported that improved verbal memory and executive function in a VR group was correlated with decreased activation in the prefrontal cortex, indicating increased neural efficiency following VR training [60]. A comprehensive review reported that executive and visuospatial abilities benefited the most from VR-based cognitive rehabilitation [20]. For patients with PD, Maggio [26] revealed that VR led to more significant cognitive improvements, especially in executive and visuospatial abilities, compared with traditional cognitive training.
rTMS may exert a priming effect that enhances the neuroplasticity of the targeted neural network [31], thus increasing its susceptibility to the concurrent or subsequent rehabilitation training. A large RCT including patients with AD demonstrated that a 6-week course of daily concurrent rTMS and computerized cognitive training significantly improved performance in cognitive tasks compared with sham treatment [35]. However, evidence regarding the therapeutic effects of combined rTMS and VR for patients with PD and MCI remains insufficient. This integrated rehabilitation approach has been proposed for patients with MCI [36] and food addiction [61]. The mechanisms of rTMS and VR affecting cognition involve the modulation of cortical excitability through neuroplasticity [62]. rTMS may first activate and promote the efficacy of the prefrontal cortex, thus facilitating the accomplishment of the following VR tasks [36]. The strength of the integrated approach lies in the joint target of both the neural and behavioral aspects of cognition, which are presumably more effective than those in a single intervention [61]. Based on the current scientific knowledge and Hebbian theory [37], we speculated that conditioning the brain with rTMS followed by a VR program can consolidate the remodeling process, thus resulting in additional cognitive benefits.
This study has several limitations that should be considered. First, we recruited a small sample size of participants due to the relatively low numbers of patients with PD visiting the physical medicine and rehabilitation clinic and willing to undergo the 10-day treatment, which may reduce the strength of our results. Second, we did not include an additional intervention group with VR-sham rTMS but the sham rTMS group instead because this study investigated the additional therapeutic effects of VR training integrated with rTMS-based treatment. The effect of VR training on cognitive facilitation has been widely studied with more convincing results compared with that of rTMS. Third, because the stimulation site was not static due to patients’ movements, we did not apply concurrent rTMS and VR training. Future studies should focus on developing appropriate VR equipment that can be applied with rTMS simultaneously and further explore the effects of different intervention time points on cognition.
In conclusion, this randomized, sham-controlled, double-blind trial reported that the integration of VR cognitive training into rTMS treatment could improve the global cognition, memory, and visuospatial executive function of patients with PD. Conditioning the brain with rTMS followed by a VR program could constitute a powerful regimen for cognitive restoration. Cognitive impairment in the early stage of PD predisposes patients to the progression of dementia, further degrading their ADL. In this study, we provided a safe and effective noninvasive intervention to attenuate cognitive decline in patients with PD. rTMS combined with VR training remains a novel intervention, and additional large-scale studies with long-term follow-ups are warranted to confirm the clinical utility of this cognitive rehabilitation.
Footnotes
ACKNOWLEDGMENTS
The authors thank Hsin-Yi Huang and Wei-An Wang for their contribution to this research.
This work was supported by the MOST (108-2314-B-075-047).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.