
Abstract
Despite decades of research and billions in global investment, there remains no preventative or curative treatment for any neurodegenerative condition, including Parkinson’s disease (PD). Arguably, the most promising approach for neuroprotection and neurorestoration in PD is using growth factors which can promote the growth and survival of degenerating neurons. However, although neurotrophin therapy may seem like the ideal approach for neurodegenerative disease, the use of growth factors as drugs presents major challenges because of their protein structure which creates serious hurdles related to accessing the brain and specific targeting of affected brain regions. To address these challenges, several different delivery systems have been developed, and two major approaches—direct infusion of the growth factor protein into the target brain region and in vivo gene therapy—have progressed to clinical trials in patients with PD. In addition to these clinically evaluated approaches, a range of other delivery methods are in various degrees of development, each with their own unique potential. This review will give a short overview of some of these alternative delivery systems, with a focus on ex vivo gene therapy and biomaterial-aided protein and gene delivery, and will provide some perspectives on their potential for clinical development and translation.
Keywords
GROWTH FACTOR THERAPY FOR PARKINSON’S DISEASE: EXTRAORDINARY POTENTIAL, HUGE CHALLENGES
It stands to reason that, if one of the central pathological features of Parkinson’s disease (PD) is the dysfunction, degeneration and death of dopaminergic neurons in the brain [1], then a therapeutic intervention aimed at preventing, slowing or reversing this neuronal pathology would have a transformative impact on current symptomatic therapeutic offerings to patients [2]. One neuroprotective and neurorestorative approach that has extraordinary potential is the use of neurotrophic growth factors, such as glial cell line-derived neurotrophic factor (GDNF), which are inherently capable of promoting the growth and survival of dopaminergic neurons [3]. However, because growth factors are proteins, this presents huge challenges in traversing the blood brain barrier and specifically targeting the diseased brain region(s) [4]. Thus, unless the challenges of growth factor delivery to the brain are surmounted, this promising approach will never reach its full potential for the treatment of PD.
Of the different delivery systems that are under investigation, two frontrunners have emerged, and both have already progressed through preclinical development and evaluation onto clinical testing in patients with PD [4]. These are infusion of the growth factor protein directly into the target brain region via implanted cannulae [5–12], and injection of viral vectors encoding the growth factor gene into the target brain region [13–15]. Although the clinical trials of these approaches have met with mixed success—and this has been the subject of comprehensive analysis elsewhere [4]—the issue of delivery remains one of the major hurdles to clinical translation of growth factor therapy for PD [3]. This article will provide a short overview of some of the other delivery methods that are being developed in this context and, in particular, we will focus on the potential of two broad areas that are making exciting strides forward, namely ex vivo gene delivery, and biomaterial-aided protein or gene delivery (Fig. 1).
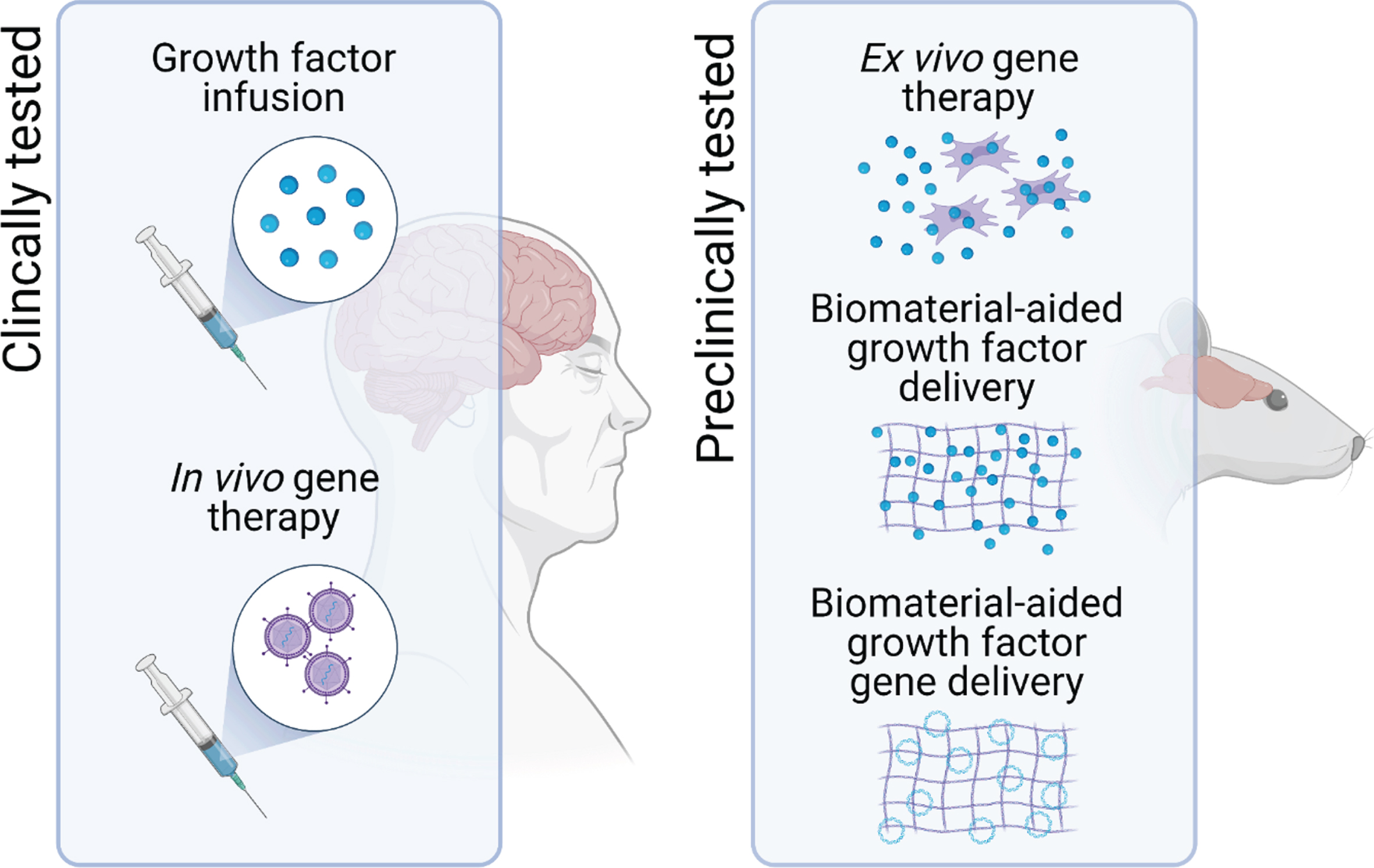
Potential delivery systems for neurotrophic growth factor delivery in PD. To assess the therapeutic potential of neurotrophic factor therapy, direct infusion of the growth factor protein into the target brain region and in vivo gene therapy have progressed to clinical trials in patients with PD. However, one of the major hurdles to the clinical translation of growth factor therapeutics for PD remains issues related to the delivery of these protein drugs. To address this, other delivery systems, including ex vivo gene therapy and biomaterial-aided protein and gene delivery are in preclinical development.
ALTERNATIVE DELIVERY SYSTEMS: EX VIVO GENE DELIVERY
Ex vivo gene therapy is the process by which cells are genetically engineered to produce therapeutic factors, such as neurotrophic growth factors, prior to their use as a therapy for patients [16]. In this approach, the cells themselves are then used as the delivery vehicles for the growth factors. Proponents of this approach suggest that its main advantage over the in vivo gene therapy approaches that have already reached clinical trials for PD are that, because the genetic engineering occurs ex vivo, the gene vector is not injected directly into the patient’s brain and the engineered cells can be subjected to rigorous preclinical evaluation prior to administration to the patient. Notwithstanding this suggestion, it must be emphasised that the safety of in vivo gene therapy for PD has been shown in several clinical trials (reviewed in [17]).
As with all emerging therapeutic approaches, there are a plethora of considerations that need to be explored before ex vivo growth factor gene delivery can be tested in patients with PD [16]. These are summarised in Table 1 and include the choice of gene vector, the nature of the cell donor, the type of cell and the route of administration.
The key considerations facing ex vivo growth factor delivery for PD
References: For more detail on the considerations facing the development, evaluation and clinical translation of ex vivo gene therapy for PD, please see this excellent review by Svendsen and colleagues [16].
Vectors
A range of gene vectors can be used for ex vivo gene therapy including viral vectors, plasmid vectors, and more recently developed gene editing technologies, and each of these has its associated advantages and drawbacks. Regarding potential for clinical translation, the vector will need to be safe, particularly in terms of the risk of insertional mutagenesis/oncogenesis as well as offering control over gene expression in instances where the patient might experience unwanted consequences of excessive/uncontrolled growth factor production. The selected vector will also need to be efficacious in terms of its ability to engineer the selected cell type and to drive long term expression of the growth factor gene.
Donors
The cell donor is also an important consideration, particularly in terms of using cells from the patients themselves (autologous) versus using cells from different donors (allogenic), but also in terms of the ethical acceptability of the cell source with adult cells being more ethically acceptable than those derived from embryonic or fetal sources.
Cells
The type of cell used for ex vivo gene therapy is of critical importance for clinical translation. The cells should be readily available, and amenable to in vitro expansion and genetic engineering. From a safety perspective, there should be no risk of tumorigenicity from the implanted cells, and ideally from a safety perspective, they should be autologous so that immunosuppression is not required. With regard to efficacy, the cells used should be able to survive for many years in the brain in order to provide sustained growth factor delivery to the site of degeneration.
Route
The route of administration for the cells is also an important consideration. Systemic delivery may seem ideal but this has consequences for reaching the target brain region and has increased potential for off-target effects. The obvious alternative is intracerebral, either into the ventricles (less damaging, but more remote) or into the target site (more direct, but potentially more damaging).
Taking these considerations into account, several innovative approaches to ex vivo growth factor gene delivery are emerging. Studies by Clive Svendsen and colleagues have used human neural progenitor cells for successful ex vivo delivery of GDNF in rodent and nonhuman primate models of PD [18, 19], and a recent study by the same group [20] used a doxycycline-regulated plasmid vector to drive controllable GDNF expression in induced pluripotent stem cell (iPSC)-derived neural progenitors in the mouse brain. The vector construct was capable of stable integration into the progenitor genome and could regulate GDNF expression in the brain over multiple doxycycline cycles. Moreover, the use of iPSCs as the source of cells opens the possibility of an ethically-sound, autologous approach to ex vivo growth factor gene therapy, and their differentiation into neural progenitors improves both their safety in terms of tumorigenesis as well as their efficacy in terms of long-term ability to survive in the brain. Using iPSC-derived neural progenitors does require direct transplantation into the target site but this seems like a small cost to pay for all of the potential benefits of this innovative approach.
Another intriguing approach that may allow for systemic delivery of the engineered cells harnesses the inherent ability of circulating macrophages to home to, and gain entry to, sites of damage, neuroinflammation and degeneration in the brain [21]. Several studies have now shown that macrophages or hematopoietic stem cells (HSCs) with a macrophage specific promotor can be engineered to overexpress growth factors (including GDNF and neurturin) [22–28]. When administered intravascularly or intrathecally, these cells accumulate at sites of degeneration in the brain, produce GDNF and ameliorate parkinsonism in several rodent models of PD.
ALTERNATIVE DELIVERY SYSTEMS: BIOMATERIAL-AIDED GROWTH FACTOR DELIVERY
Another alternative delivery system for growth factor delivery in PD that has seen exponential research and development over the past 15 years is in the use of biomaterial-based systems to aid protein or gene delivery [29–31]. Biomaterials are materials that are engineered to interact with biological systems primarily for therapeutic purposes. Their potential application to PD therapeutics is vast and has been reviewed extensively elsewhere [31]. For growth factor delivery specifically, biomaterials have potential to aid in the delivery and maintenance of growth factor proteins or genes in the brain.
Biomaterial-aided growth factor protein delivery
One approach that has been the subject of intense research is using polymeric biomaterials as intracerebrally-injectable microcarriers to protect encapsulated growth factor proteins and release them slowly over time within the diseased region of the brain [32]. Although numerous studies have shown that intracerebral injection of microencapsulated growth factors including GDNF [33–39] and vascular endothelial growth factor (VEGF) [34, 40] can improve parkinsonism in both rodent [34–42] and primate [33] models of PD, the main limitation of this approach is that the growth factor release in the brain is rapid and not sustained, a major issue if biomaterial-aided growth factor therapy is to provide meaningful benefit in the decades-long pathogenesis of PD in patients. One potential solution to this could be the use of highly charged microscale depot systems that provide strong electrostatic attraction between the therapeutic protein(s) and the microcarrier [43]. Not only does this result in slower release of the therapeutic protein, but it also has the potential to be refillable or reloadable, although this too is limited as each refill would require intracerebral injection of the growth factor.
Whilst intracerebral infusion of growth factors represents the most direct way to bypass the blood-brain barrier, intranasal delivery represents an exciting alternative delivery route to the midbrain, via the olfactory system and trigeminal nerve [44–46]. This is another delivery method where biomaterial systems can aid with delivery of the growth factor to the brain. In particular, using cationic lipid-based nanoparticles can protect the encapsulated growth factor(s) and increase electrostatic interactions at the olfactory epithelium to increase uptake to the brain [44–46]. Although several studies have shown that intranasal administration of the GDNF protein itself can ameliorate parkinsonism in animal models [47, 48], encapsulation of the protein within lipid nanoparticles [48–50], especially those functionalized with the cell-penetrating peptide TAT [50], significantly improves the outcome. Although ease of administration is a clear plus with intranasal delivery, this route of administration has been shown to increase GDNF expression throughout the whole brain [51], a potential limitation to clinical translation in terms of off-target effects.
Biomaterial-aided growth factor gene delivery
In general, despite some potential advantages in safety and production, non-viral gene vectors have lagged behind their viral counterparts, and non-viral gene delivery to the brain, whether via intracerebral or systemic routes, has proven particularly challenging [52]. Systemic administration would represent a significant clinical advantage over intracerebral administration required for the in vivo gene therapy approach used for viruses. Although there has been some success in using Trojan horse liposomes [53] for systemic GDNF gene delivery in PD models [54, 55], in general, brain uptake is typically low and without regional targeting [29].
An exciting recent advancement which could serve to overcome these drawbacks, has been to harness the potential of focused ultrasound to disrupt the blood brain barrier thereby improving brain access and targeting of circulating therapeutics [56–58]. Indeed, liposomes [59–63] and other biomaterial particles [64–66] have been shown to protect and improve brain penetrability of both growth factor protein [60, 65] and gene therapies [59, 66] after focused ultrasound in animal models of PD. The first clinical trial of focused ultrasound for blood brain barrier opening in PD is currently running (NCT03608553) and time will tell if this approach is both safe and efficacious.
CONCLUSION
Despite many decades of intensive research, there remains no disease-modifying neuroprotective or neurorestorative therapy for PD. Many consider that the most promise lies with growth factor therapy, but significant challenges have to be surmounted in order to translate these protein drugs to an effective and safe therapeutic option for patients. Direct infusion of the growth factor proteins to, and in vivo gene therapy within, the affected brain region(s) are still the only approaches that have reached clinical trial, and they remain the most promising solution. However, recent developments in ex vivo gene therapy (particularly in engineering controllable gene vectors and in harnessing patient-derived, neurally reprogrammable adult cells) and in biomaterial-aided protein and gene delivery (especially related to intranasal delivery and delivery through the ultrasound disrupted blood brain barrier) bring alternative growth factor delivery systems ever closer to clinical trial.
Footnotes
ACKNOWLEDGMENTS
Our research in this field is funded by the Michael J Foundation for Parkinson’s Research (Grant Number: 17244), Science Foundation Ireland (Grant Number: 19/FFP/6554) and the European Union Horizon 2020 Programme (H2020-MSCA-ITN-2015) under the Marie Sklodowska-Curie Innovative Training Networks (Grant Number: 676408).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.