
Abstract
Alpha-synuclein deposits are detectable in skin biopsies of patients with Parkinson’s disease and other synucleinopathies like multiple system atrophy by immunohistochemical staining. As they are easily to obtain, they appear a promising tool for the pre-mortem histopathological confirmation of the disease and as a potential outcome measure in studies targeting alpha-synuclein aggregates. Good sensitivity, specificity, and practicability are the most important requirements of a biomarker. The review gives an overview on all three aspects, addresses methodological problems and the lack of standardized procedures as a major problem and gives an outlook on the future of skin biopsy as a potential diagnostic tool in synucleinopathies.
INTRODUCTION
Diagnosis of idiopathic Parkinson’s disease (iPD) is often difficult, especially at early stages of disease. Diagnosis is mostly based on clinical symptoms, comprising the motor symptoms tremor, rigor, akinesia and postural instability [1]. Research in the last decade has focused on the search of a feasible biomarker for iPD that allows a reliable diagnosis of the disease. As iPD has proven to be a multisystemic neurological disease with not only involvement of the brain but also neurons and nerve fibers of the peripheral nervous system, the latter has come into focus as it is easily accessible pre-mortem. Since the detection of Lewy bodies in neurons of iPD patients by F. H. Lewy in 1912 [2], this has been the gold standard of post-mortem neuropathological confirmation of the disease. In 1997, Spillantini et al. identified aggregated alpha-synuclein to be the major component of Lewy bodies [3]. Since then, immunohistochemical detection of alpha-synuclein deposits has been the neuropathological hallmark of iPD. Only in the last decades, alpha-synuclein deposits were detected in neurons and neurites of the peripheral nervous system (Fig. 1), rendering the detection of alpha-synuclein aggregates in tissues of the PNS a potential pre-mortem biomarker of the disease [4]. Alpha-synuclein deposits have so far been detected in nerve fibers of the enteric nervous system, submandibular gland and skin biopsies [5–14]. Studies detecting phosphorylated alpha-synuclein (p-alpha-syn) in biopsies of salivary glands of patients with iPD reported high specificity (100%) and sensitivity (56–100%) in submandibular glands [9, 15–17]. A relevant number of unilateral biopsies of the submandibular gland did not contain salivary gland tissue [16] but better tissue acquisition was achieved in bilateral submandibular biopsies or in biopsies of minor salivary glands [18, 19]. Studies on biopsies of gastrointestinal tissue included different biopsy sites and sensitivity and specificity very much varied between studies [5, 20–23]. Skin biopsy seems to be a feasible tool as it is minimally-invasive, repeatable and the procedure does not require any special expertise. P-alpha-syn, that in contrast to native alpha-synuclein is highly specific for synucleinopathies, can be detected by immunohistochemical staining of skin sections [13, 14]. Even though the potential use of skin biopsy as a histopathological biomarker has been addressed in an increasing number of studies, it is still not an established tool in the diagnosis of iPD. In this review, four basic requirements of a biomarker in PD are addressed: Sensitivity, specificity, practicability and detection of prodromal stages of disease.
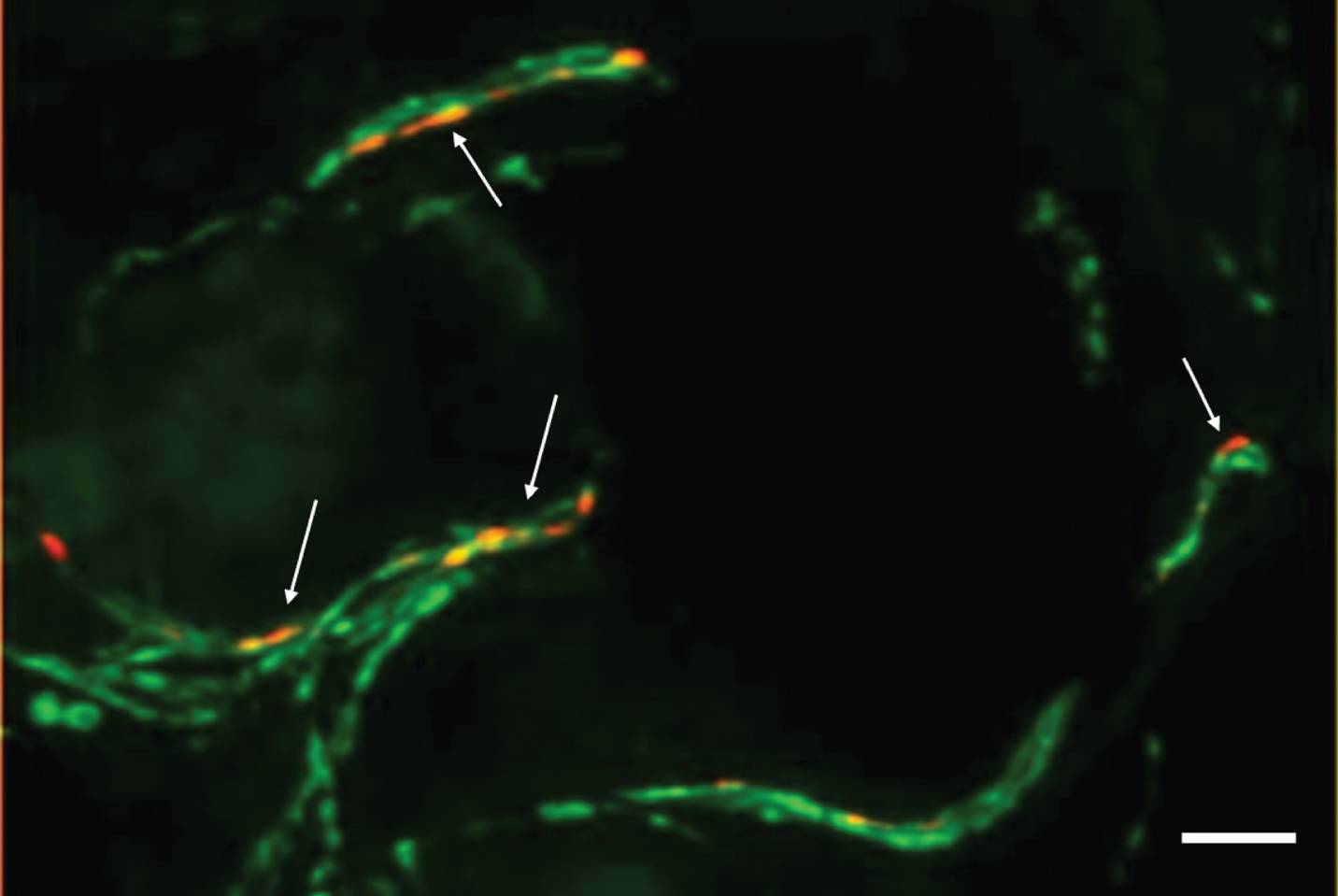
Photomicrograph of a double-immunofluorescence staining with anti-phospho-alpha-synuclein (red, Covance, 1:500) and anti-protein-gene-product 9.5 (axonal marker, green, Zytomed Systems, 1:1000) of a skin biopsy of a patient with iPD. The biopsy was fixed with 4%paraformaldehyde prior to cryopreservation and 20-μm-sections were cut. Arrows indicate intraaxonal phospho-alpha-synuclein depositions. In samples of controls, no p-alpha-syn-positive depositions would be visible. Bar = 20μm.
METHODS
Pubmed was searched for the terms “skin biopsy”, “alpha-synuclein” and “Parkinson”/”RBD” and the results were checked for relevance. All pre-mortem studies on patients with Parkinson’s disease and/or iRBD that analyzed alpha-synuclein deposition within dermal nerve fibers were included.
Is dermal p-alpha-syn deposition a sensitive marker of PD?
First promising results on the use of p-alpha-syn detection in skin biopsies as a biomarker were obtained by Ikemura et al. when studying autopsy samples with a sensitivity of 70%for iPD and specificity of 100%compared to patients without CNS Lewy body pathology [12]. However, a subsequent analysis of pre-mortem biopsy samples of PD patients only resulted in a low sensitivity of 10%[11]. Only in the last decade, further studies on cutaneous p-alpha-syn deposition with a high specificity of 100%compared to controls and a sensitivity of 55%to 100%were published [13, 25] (Table 1). Besides these studies with a moderate to high sensitivity of dermal p-alpha-syn detection there were also studies that did not succeed in detection of p-alpha-syn in skin biopsies or only with a very low sensitivity [26, 27] (Table 1). The use of different protocols of biopsy procedure, fixation, immunostaining and neuropathological assessment were discussed as possible reasons, disclosing the need of methodological studies comparing different protocols [25, 29]. Whereas inter- and intra-laboratory reproducibility of analysis of skin sections was successfully demonstrated [30], studies comparing fixation and staining procedures are scarce [25, 29]. Recently, the Systemic Synuclein Sampling Study (S4), a multi-center observational study compared different staining procedures on paraffin-embedded tissue resulting in the establishment of an optimized protocol for paraffin sections [31]. They reported a sensitivity of 24.1%for skin biopsies that is much lower compared to former studies [32]. However, when taking a closer look at published studies (Table 1), the highest sensitivity was mostly reported in studies using cryosections. Unfortunately, systematic comparison of biopsy procedures in the S4 study was restricted to formalin-fixed paraffin-embedded tissue that indeed appears to be more feasible in clinical practice [31], but may result in lower sensitivity (Table 1). Although systematic comparison of formalin-fixed paraffin-embedded and freshly-fixed cryoconserved tissue is lacking, it becomes evident that in the majority of studies reporting a moderate to high sensitivity, skin biopsies were cryoconserved following the recommendations that were long ago established for the use of skin biopsies in the diagnosis of peripheral neuropathies [33, 34] and that are based on comparison of different fixatives for neuronal markers in skin biopsies and experience from studies establishing skin biopsy as a diagnostic tool for small fiber neuropathy [35, 36]. Furthermore, cryosections with a thickness of 10–50μm allow the analysis of nerve fibers in their length whereas paraffin sections with a thickness of 2–5μm only contain few fibers that cannot be studied in length and make it difficult to discriminate between specific staining and artefacts [37]. A very recent study focusing on optimal thickness of sample sections of skin biopsies for detection of dermal p-alpha-syn deposits confirmed these observations [38]. However, a very recent study reported a higher sensitivity of 70%in iPD subjects by using double-staining of p-alpha-syn and PGP9.5, an axonal marker of formalin-fixed-paraffin-embedded tissue, demonstrating that a moderate to high sensitivity can also be obtained when using paraffin sections [39]. Double-staining with an axonal marker, pretreatment of sections with protease and alkaline phosphatase and evaluation of additional sections in subjects with a low number of PGP9.5-positive nerve fibers were discussed as relevant points to increase sensitivity, but again direct comparison with other protocols is lacking [39]. Another aspect that may have a direct effect on sensitivity is the choice of the best site of biopsy. Different biopsy sites were studied (see Table 1) and paravertebral (mostly C7/8) sites and the leg are the biopsy sites that were most often chosen. However, large studies systematically comparing different biopsy sites are lacking. There is some evidence of a proximal-to-distal gradient of p-alpha-syn positivity in patients with iPD [13, 40]. A recent study reported a distal-to-proximal gradient in patients with MSA whereas in an earlier study the proximal leg was mostly affected in patients with MSA [40, 41]. Both studies suggest that the distribution of p-alpha-syn in MSA may be different to iPD but larger studies are needed.
Overview on studies on the detection of alpha-synuclein in dermal nerve fibers of patients with synucleinopathies by immunohistochemistry or RT-QuIC using skin biopsies of living subjects
Double-immunofluorescence=double-labeling with an axonal marker (mostly PGP9.5). (Sens., sensitivity; Spec., specificity; PD, Parkinson’s disease; HC, healthy control; n-alpha-syn, native alpha-synuclein; p-alpha-syn, phosphorylated alpha-synuclein; MSA, multiple system atrophy; ET, essential tremor; PAF, pure autonomic failure; (i) iRBD, isolated REM sleep behavior disorder; PFA, paraformaldehyde.
Is dermal p-alpha-syn deposition a specific marker of PD?
Studies using antibodies that specifically recognize p-alpha-syn unequivocally reported a specificity of 100%compared to controls [13, 32]. Diffuse or granular p-alpha-syn staining that could be removed by pre-treatment with alkaline phosphatase and protease was also reported in controls, but discrete p-alpha-syn was restricted to patient samples [39]. Using an antibody against native alpha-synuclein, Wang et al. reported higher immunoreactivity in skin biopsies of patients with iPD compared to controls, but native alpha-synuclein was also detectable in dermal nerve fibers of healthy subjects [42]. Native alpha-synuclein was equally detected in dermal ann-exes’ innervation of patients with synucleinopathies and controls in other studies [24, 40]. In contrast, ant-ibodies specifically directed against aggregated alp-ha-synuclein (5G4) or the use of protein K digestion have also been described to allow differentiation between biopsies of patients with iPD and controls [31, 44]. However, dermal p-alpha-syn deposition is not a specific marker of iPD but was also described in other synucleinopathies: In multiple system atrophy, p-alpha-syn was predominantly detected in somatosensory nerve fibers, in contrast to iPD where mainly autonomic fibers are affected [40, 41]. In pure autonomic failure and dementia with Lewy bodies, p-alpha-syn can also frequently be found in dermal autonomic nerve fibers [24, 46].
Can dermal p-alpha-syn deposition detect prodromal stages of disease?
Prodromal stages of iPD are difficult to diagnose as there are no specific markers. Studies on prodromal stages of iPD often focused on isolated REM sleep behavior disorder (iRBD) which is one of the most specific early symptoms of a synucleinopathy with a conversion rate of more than 80%[47, 48]. Dermal p-alpha-syn could be detected in patients with iRBD and p-alpha-syn deposition correlated with other markers of prodromal PD like olfactory dysfunction, reduced dopamine transporter density measured by FP-CIT-SPECT or the likelihood ratio of prodromal PD based on the MDS criteria [49–51]. These findings give evidence that dermal p-alpha-syn deposition may be a marker of disease progression at prodromal stages. P-alpha-syn deposition was detectable in patients with normal FP-CIT-SPECT, thus indicating that it probably is a very early marker of a synucleinopathy [49, 50]. However, it needs to be taken into account that these data are based on patients with iRBD only. Studies focusing on dermal p-alpha-syn in iRBD-negative prodromal stages are needed but so far lacking because prodromal stages are difficult to diagnose.
Is the use of skin biopsy a feasible tool for the diagnosis of PD?
Practicability of skin biopsy for the diagnosis of iPD is frequently discussed. It is cheaper and more broadly available compared to FP-CIT-SPECT. When comparing it with biopsies of gastrointestinal tissue that require endoscopic procedures or biopsies of the submandibular gland it is more easily to perform and skin biopsy is mostly well-tolerated by the patients [52]. However, processing and cryoconservation of biopsies requires laboratory equipment. Due to the low number of p-alpha-syn deposition, step sections and/or analysis of multiple biopsy sites are necessary and are rather time-consuming. Evaluation of skin sections at the microscope needs to be done by experienced examiners and is also time-consuming [31]. For these reasons, high-throughput biochemical procedures that allow objective and repeatable measurement of a large number of samples in a short time are needed. The most promising approach at the moment is RT-QuIC, an aggregation assay that was developed for the detection of prions in Creutzfeldt-Jakob disease [53]. As prion-like seeding activity can also be found in alpha-synuclein, small amounts of dermal alpha-synuclein become detectable by RT-QuIC [54]. Several studies detecting alpha-synuclein aggregates in cerebrospinal fluid of patients with iPD, dementia with Lewy bodies and iRBD showed promising results [54–56] and the first studies using RT-QuIC in skin lysates seem promising [57, 58]. However, larger studies including prodromal stages of iPD are needed to evaluate the use of dermal RT-QuIC as an early biomarker in iPD.
Where will the way of skin biopsy lead us?
More than ten years have passed since detection of p-alpha-syn in skin biopsies of patients with iPD. Numerous studies have confirmed the involvement of autonomic nerve fibers in alpha-synuclein pathology and improved protocols allow to detect p-alpha-syn with very good specificity and moderate to high sensitivity even at prodromal stages of disease [13, 50]. Nevertheless, skin biopsy is far from being an established diagnostic tool in PD. Immunofluorescence staining of serial section and the need of multiple biopsy sites to obtain a good sensitivity seem to be the major difficulties that hinder skin biopsy from getting an established biomarker in clinical routine. Most recently, RT-QuIC, a biochemical aggregation-based assay was studied as an efficient and more feasible method for the analysis of alpha-synuclein deposition in skin biopsies but also other tissues including CSF [54–58]. At the moment, RT QuIC appears a promising methodological approach for the detection of alpha-synuclein aggregates outside the brain but is still at an early stage of research. Future studies need to specify its sensitivity, specificity and reproducibility. Different tissues and biofluids need to be studied in comparison by immunohistochemistry as well as RT-QuIC to find the most appropriate biomarker for the future.
CONFLICT OF INTEREST
The author reports no conflicts of interest.