
Abstract
Background:
Parkinsonian syndromes are heterogeneous chronic neurodegenerative disorders associated with both motor and non-motor symptoms. The symptoms have major psychosocial effects on the quality of life of patients and can be a burden for caregivers. So far, several questionnaires have been developed to assess quality of life in Parkinsonism, but none of these include the positive sides on well-being such as personal and social resilience factors.
Objective:
The aim of this study is to develop a digital framework for a longitudinal assessment of quality of life during the progression of Parkinson’s disease.
Methods:
The CHAPO model (Challenges and Potentials) has been established in a vast study by Wagner et al. to assess the quality of life of older people. This model includes environmental and individual factors, life chances, and life results, such as individual life evaluation, from a subjective as well as an objective point of view. Therefore, it has been adapted in several development steps to include the specific aspects that affect quality of life in Parkinsonian syndromes. The development process included 6 steps: definition, refinement, operationalization, piloting/debriefing, adjustment, and integration.
Results:
The development of the CHAPO-PD model has been completed and it represents the first main result of this study.
Conclusion:
By taking a holistic understanding of quality of life into account, we expect to detect previously unrecognized factors, which correlate to the subjective well-being of Parkinson’s disease patients, and aim to use these findings to improve the health care structures for patients with Parkinson’s disease and related disorders.
Keywords
INTRODUCTION
The term “quality of life” (QoL) was coined by the English economist Arthur Cecil Pigou in a 1920 publication, going on to become thoroughly implemented as an important concept in philosophy and politics. A wide variety of concepts of QoL have been developed in other disciplines since then as well. In medicine, QoL—closely related to the notion of well-being—has been increasingly considered an important aspect of human health. For example, the Constitution of the World Health Organization (WHO) defines health as “A state of complete physical, mental, and social well-being, not merely the absence of disease” [1].
Parkinson’s disease (PD) is one of the most common neurodegenerative disorders [2] and can be an extremely hefty burden for patients, families, and caregivers. Due to neural degeneration and loss of dopaminergic cells in the substantia nigra, impaired motor functioning (tremor, rigidity, bradykinesia, postural instability) and a variety of non-motor symptoms [3, 4] often progressively lead to increased support needs as well as deterioration in the patient’s QoL [5, 6].
Maintaining and improving patients’ QoL is one of the primary objectives of care for patients with chronic diseases. To date, management of PD has been focused on symptomatic improvement through pharmaceutical and physical therapies, and therapeutic success is primarily evaluated by assessment of QoL [7].
Existing QoL questionnaires currently recommended by the International Parkinson and Movement Disorder Society (MDS) (for an overview, see [8]), which are sensitive enough for a longitudinal assessment [9], infer QoL from the frequency and severity of the disease. However, objective living conditions can be assessed differently at the subjective level with regard to their individual significance for lifestyle and, e.g., not everyone subjectively perceives a good quality of life in objectively positive living conditions. Thus, particular methodological challenges exist especially in the authentic recording of the subjective, QoL-relevant aspects from the patient’s perspective [10]. In recent years, however, there have been increasing scientific efforts to consider QoL from a holistic point of view [11–14], which has been applied to a variety of patient groups. This change is attributed to the notion that individual assessment of QoL is affected by a complex interplay between a person’s physical health, psychological state, personal beliefs, social relationships, and their relationship to salient features of their environment, as compared to their goals, expectations, standards and concerns [1, 15]; QoL points to the relationship between an individual’s state as it is versus how it should be. Such a formulation is considered comprehensive and is occasionally referred to as “Holistic Quality of Life,” [1, 16].
For a holistic evaluation of QoL the WHO established the WHOQOL-100 and the WHOQOL-BREF (Best Available Techniques Reference) as questionnaire tools, which focus mainly on a subjective app-roach to QoL [1]. Due to a worldwide demographic change attributed to an ageing population, the specific aspects of older adults’ QoL have moved to the forefront of scientific interest, resulting in the development of the WHOQOL-OLD tool, which has been tailored for elderly adults above the age of 60 [17]. Although PD patients tend to affect elderly adults, those purely quantitative tools were not specifically designed for chronic, multifaceted PD and cannot sufficiently reflect the subjective, QoL-relevant aspects from the patient’s perspective. Depending on the severity of the disease, for instance, or the circumstances of life and the personality, the QoL-relevant aspects vary and can change fundamentally in disease progression. Therefore, a purely quantitative method of measurement cannot adequately capture the holistic quality of life from the patient’s perspective. Thus far, the various established studies measuring QoL with regards to elderly people in Germany and abroad have been limited only to certain regions, specific age ranges, or other specific sample-limiting factors. To address this deficit a comprehensive German study of elderly people from diverse backgrounds was conducted [18], resulting in the creation of the Challenges and Potentials (CHAPO) model as a framework for quantitatively assessing QoL in older people and generalizing the results. The CHAPO model was designed to be accessible for use in research and to be evaluated using qualitative data analysis. By combining quantitative and qualitative elements, this framework links the subjective data through open-ended questions, e.g., the desired future and objective data through uniform instruments for assessment, which can then be adapted to more specific demographic characteristics, e.g., the very old or those over the age of 80 years. This model considers environmental and individual factors along with their reciprocity, life chances, and life results such as individual life evaluation from a subjective as well as an objective point of view [18], and considers the ethical dimension of a fulfilling life. The model is based on Veenhoven’s [19] concept of “the four qualities of life,” distinguishing on the one hand between “life chances” (e.g., opportunities) and “life results” (e.g., personal evaluation of the individual’s life), and “outer” and “inner qualities” on the other [18]. The CHAPO model improves upon this foundation by proposing an explicit focus on goals and values as regards both personal resources (e.g., personal values, individual conditions) and environmental resources (e.g., societal standards, environmental conditions). In addition, it is designed to clearly delineate qualities of person-environment interaction (e.g., life conduct, activity, everyday interaction) on the life results level, enabling more flexibility to integrate functional [20] and eudemonic [21] concepts of QoL appearing to be of particular relevance to the very old or persons with chronic diseases and increased vulnerability. Figure 1 gives an overview of the CHAPO model.
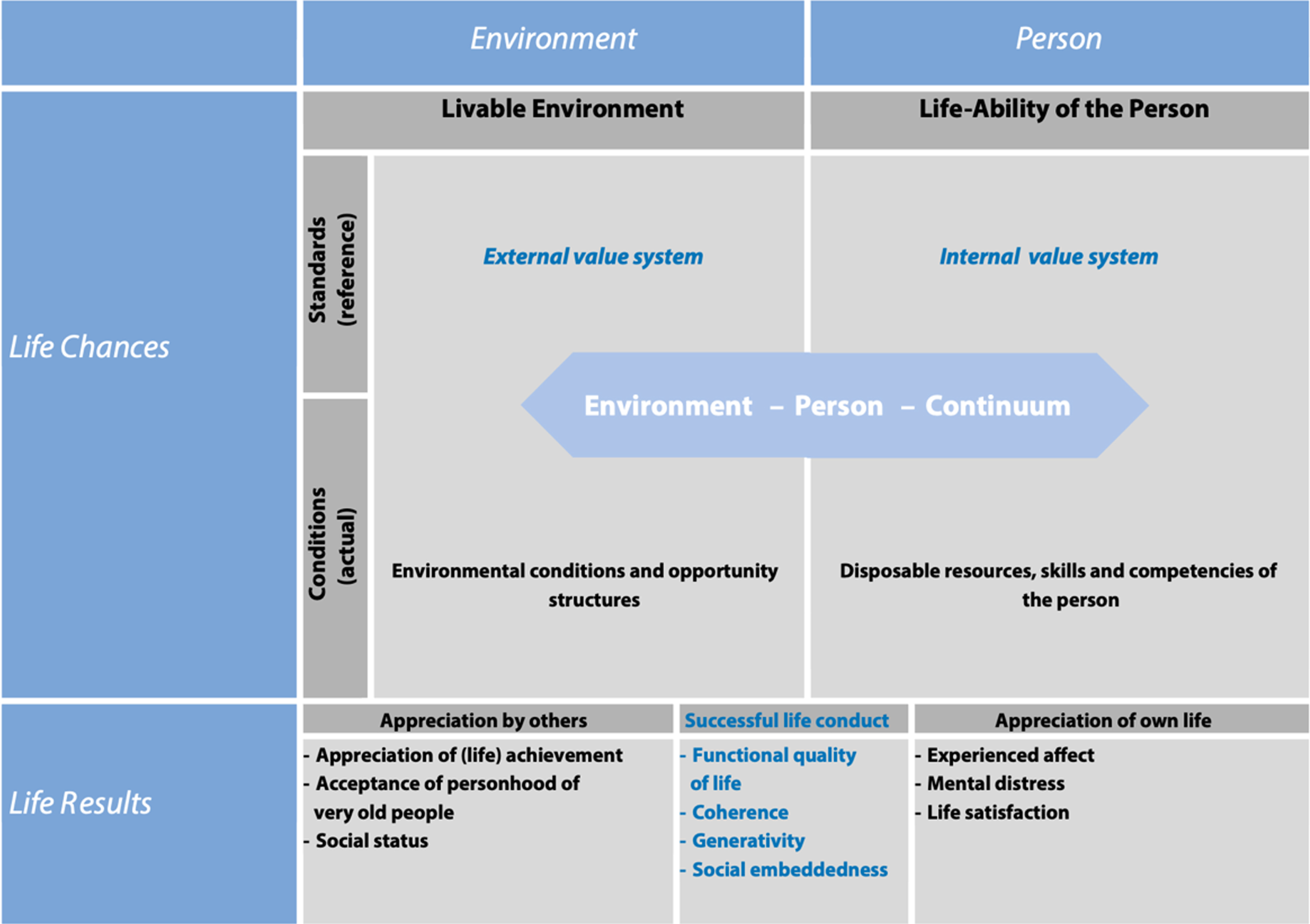
The challenges and potentials (CHAPO) model of quality of life in very old age [18].
To the best of our knowledge, to date no comprehensive approach to QoL in PD patients has been investigated. In order to enable such a sophisticated evaluation, we aim to present the development steps of CHAPO-PD model, or “Challenges and Potentials model of Quality of life in Parkinson’s Disease,” a newly developed questionnaire tool to assess the QoL in PD patients. By linking qualitative and quantitative aspects, the concept enables the subjective view of the patients to be at the center of this model, and thus the collected objective and subjective data plausibly reflect the patient’s QoL. According to the findings of Reuther et al. we expect this new disease-related approach to be sensitive enough for longitudinal assessment [9] as well as to detect unknown factors, which correlate with the subjective well-being of PD patients.
The CHAPO-PD model can be considered as highly innovative because, unlike other QoL questionnaires for PD patients, it relies heavily on inter-disciplinary cooperation to record comprehensive, multidimensional influences on QoL in addition to disease-specific factors. The digitalized version, described the last of 6 development steps within the following “Methods” section, will enable an assessment independent of location and without transmission errors, even in the advanced stages of PD. The model could be further considered for a longitudinal assessment for therapy control, as well as a basis for the development of novel, multimodal therapy concepts in order to maintain QoL and to improve healthcare structures for PD patients and their caregivers [22, 23].
METHODS
The CHAPO model has been established in a vast study by Wagner et al. to assess the QoL of the elderly, including environmental and individual factors, life chances, and life results from a subjective as well as an objective point of view [18]. It has been adapted to include the specific aspects that affect QoL in parkinsonian syndromes within the CHAPO-PD model. The development process included 6 steps: definition, refinement, operationalization, piloting/debriefing, adjustment, and integration. The first two steps of CHAPO-PD’s development process consisted of an item definition (1) and item refinement and (2) by discussing all elements in an expert panel. Next, the assessment tools were chosen and operationalized step by step (3). This was followed by a piloting and cognitive debriefing (4) process in order to assess the model’s feasibility in healthy control groups and PD patients, which led to the adjusted final version (5) of the CHAPO-PD framework that was integrated into an electronic questionnaire platform (6). In the following segment, the stages of the development process are expounded upon in more detail.
Item definition
An expert panel, comprised of a movement disorder specialist, a psychologist, a social scientist, a neuropsychologist, an ethicist, and a gerontologist, identified relevant items and questions to cover the CHAPO dimensions based on current PD literature and personal experiences. The existing CHAPO model has been used to structure the domains of PD-related QoL assessment in both objective and subjective indicators such as living conditions, disposable resource, and self-evaluations of the individual’s quality of life.
Item refinement
A working group, including the movement disorder specialist, the ethicist, and the gerontologist of the expert team that developed the CHAPO model, discussed the suggested items from the previous step and refined the categories to affect a holistic assessment of QoL. After each refinement, the results were presented to the expert group and, if any new changes were observed by them, the working group performed another refinement process.
Operationalization
The suggested items were allocated to potential instruments (e.g., questionnaires, psychometric tests) by the working group next. Again, the version was presented to the expert panel and recommended changes were made based on the consensus of the group. After including recommendations from two rounds of comments and evaluations, no further changes were recommended by the panel and the first version of the CHAPO-PD was finalized.
Piloting and cognitive debriefing
Piloting and cognitive debriefing of CHAPO-PD, which entails the active testing of a questionnaire among representatives of the target population in order to determine whether respondents understand the questionnaire as intended, has been approved by the local ethics committee of the University Hospital of Marburg (Study number: 124/19). All participants were recruited from the Department of Neurology at the University Hospital of Marburg in Marburg, Germany, and within the PD healthcare network Parkinson Network Alliance in Marburg (PANAMA), and gave written informed consent prior to participation. In order to build a capable collective for piloting and cognitive debriefing, only participants without dementia and depression were included. To this end, depression was assessed by Beck’s depression inventory [24] (BDI, depressive symptoms ranging from 0–63 points: 0–13: no depression, 14–19: mild depression, 20–28: moderate depression, and 29–63: severe depression) and participants with dementia both among the healthy controls and the PD patients were excluded from our study by examination of the Montreal Cognitive Assessment (cognitive screening test: ranging from 0 to 30 points, 30 to 26 points were considered as normal cognitive function, 25 to 21 points as mild cognitive impairment, and below 21 points as suspicious for dementia, performed in the clinical “on state”) [25, 26]. Additionally, healthy controls and patients were asked to provide general information about their backgrounds and demographics.
As the intention is to utilize the CHAPO-PD model to measure the QoL of each PD patient, patients with PD according to MDS criteria [4], living both in private homes and institutional settings, as well as proxy informants, were asked to participate. Patients suffering from known atypical Parkinsonism were explicitly not excluded.
To characterize the participating PD patients, they were each additionally examined using Part III of the MDS-UPDRS (which monitors, evaluates, and rates motor function according to standardized criteria) as well as the Hoehn and Yahr scale [27] (a standardized tool for measuring progression of parkinsonian symptoms and subsequent degree of disability). To assess QoL, patients were provided with a copy of the Parkinson’s Disease Quality of Life Questionnaire 8 (PDQ-8) [28]. During the study design the study group discussed using the PDQ-39 or the PDQ-8 and decided to the more concise PDQ-8 because of the almost identical psychometrics and increased compliance due to reduction of items.
A multi-stage process of group discussions as a modified Delphi procedure [29] was chosen for piloting and cognitive debriefing of CHAPO-PD. The Delphi method is a multi-stage qualitative survey procedure. The aim of the Delphi method is to bring together the knowledge of several experts in order to derive the final version of CHAPO-PD. The expert discussions were recorded and further transcribed. First, consistency and workflow were tested in ten healthy controls within a group discussion. After this first demonstration, the order of tests was reevaluated according to the flow of the interview, placement of critical questions, and texts introducing the different sections of the questionnaire. This led to a second, refined version of the CHAPO-PD framework. Using this, eight PD patients without dementia were recruited for the initial assessment of this refined model. The feasibility, understandability of questions, total duration, and placement of questions, were assessed in group discussions in order to confirm that the framework is appropriate and comprehensive relative to the intended construct and use. This led to the third and final version of the CHAPO-PD framework.
Final adjustment
In this step, the third version of the CHAPO-PD framework was tested in another eight PD patients, following the same procedural progression as with the first and second versions described in the preceding segment. After the second round of group discussion a saturation was observed, rendering a third round redundant and unnecessary.
Input into an electronic questionnaire platform
The final version of the CHAPO-PD framework was integrated into an electronic questionnaire platform, and data, such as cognitive and motor tests, are collected and recorded using a digital application as well. With this digitalization, persons with PD will have the opportunity to complete the survey in a standardized manner throughout the course of their disease, while this paper-free testing will be able to be conducted from the comfort of the home environment. The first PD patients for a longitudinal assessment of CHAPO-PD are currently being recruited.
RESULTS
The CHAPO-PD tool has been successfully tested for practicability in a group of healthy controls and PD patients without dementia during its development. Revisions to the model leading to the final version have been summarized in Fig. 2, while the results from the drafting process are presented in the following segment.
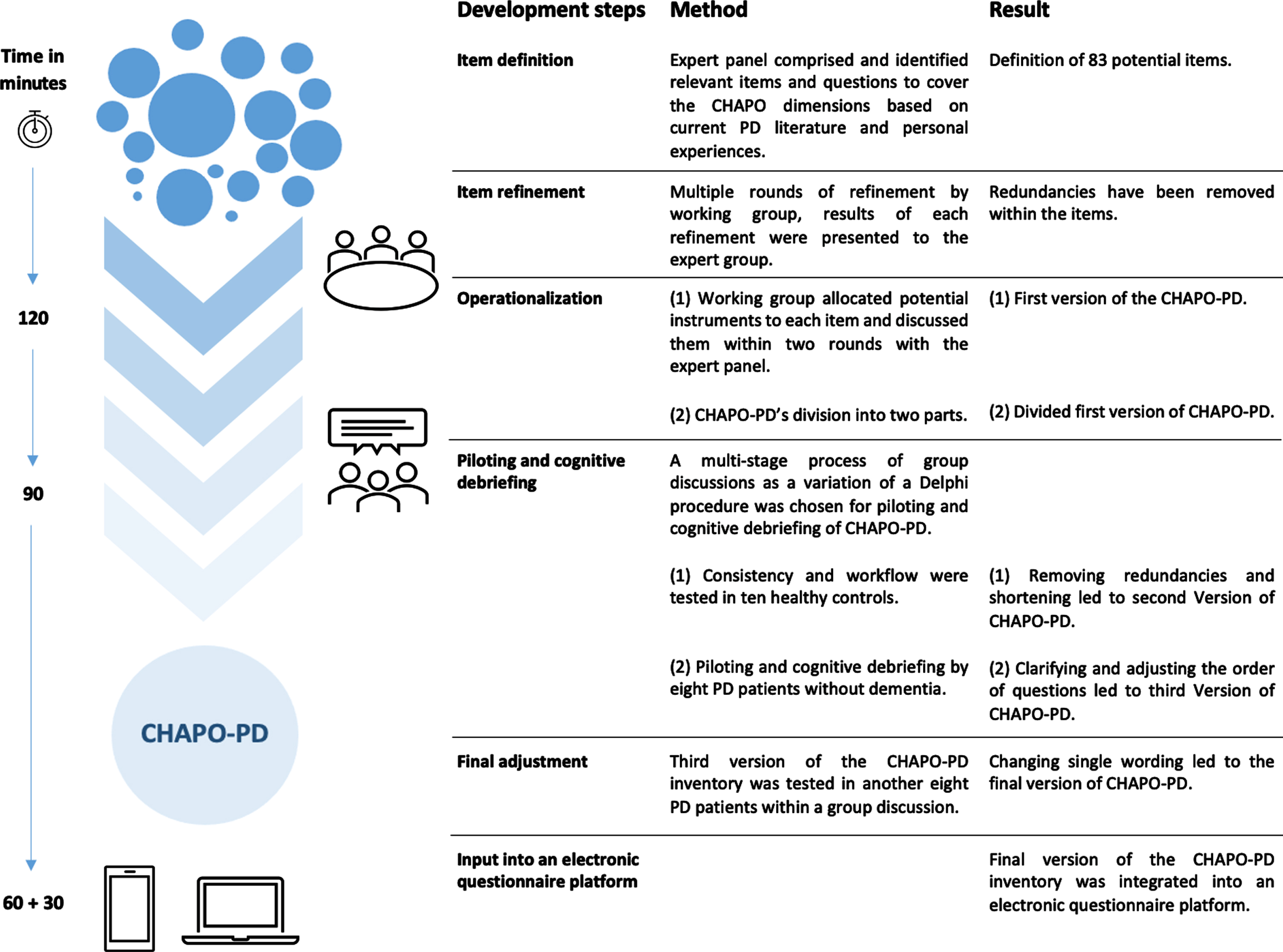
Development of CHAPO-PD.
The first step (item definition) resulted in a list of 83 potential items; these items were refined until the expert panel detected a saturation in items after three working rounds (these items are summarized and further elaborated on in Table 1). Following this, the working group performed a first operationalization of the defined items. This step demonstrated that the answering process was estimated to take about 120 min. Based on this version, the working group refined the CHAPO-PD instruments by detecting and removing redundancies in the questionnaires and tests to shorten the questionnaire tool and make it more user-friendly. The instruments were reviewed by two researchers in order to verify that all suggested domains, as defined in the previous step, were included in the new operationalized model. A first draft of the CHAPO-PD model was created and sent to the expert panel for comments and feedback. In order to facilitate the implementation of this detailed assessment as a tool in standard care in the future, the expert panel agreed to shorten the scope of the questions to 90 min without losing any of the suggested domains. Moreover, the expert panel decided to divide the working document into two functional parts—one portion of the CHAPO-PD form to be filled in by the physician or the study nurse, the other to be self-administered by the patient or with assistance from a caregiver. Pilot testing was performed next. Demographic and clinical characteristics of the participants are displayed in Table 2. None of the PD patients presented as having atypical parkinsonism, though patients suffering from known atypical parkinsonism were not excluded from this study. After the first round of review questions were clarified or adjusted in their order as found appropriate by the panel; the length of the questionnaire remained unchanged. Aside from a single wording revision, after completing a second round of group discussion in the fifth step of the drafting process no further criticisms or concerns were raised by the participants. In general, participants evaluated the tool as “innovative” and a “positive and patient-centered approach of care.” One participant summarized: “It depends on the individual and not on the symptoms of the disease whether one feels a good quality of life. The disease should not dominate life, this should be other aspects of life.” Through pilot testing, the design of the CHAPO-PD model has been refined and completed. After integrating the model into an electronic questionnaire platform, the model was retested in terms of its administration time. The questions take up to 60 min to be self-administered (also with assistance by a caregiver) and up to 30 min to be completed by a physician or study nurse.
Defined items within the development of CHAPO-PD model
Patient and control characteristics of the participants in piloting and cognitive debriefing process of CHAPO-PD model
DISCUSSION
The change in QoL has been described and investigated in PD patients as well as in various other diseases. Existing QoL questionnaires infer QoL from symptom frequency and severity of the disease, but in recent years there has been an increasing scientific effort to take a more holistic view of QoL, which has been applied to a variety of patient groups. We developed CHAPO-PD to create a new questionnaire tool to satisfy the specific needs of PD patients within the scope of a comprehensive understanding of QoL.
The CHAPO-PD model offers a new perspective on the disease and the changes in QoL associated with it by using a standardized assessment tool to record the individual well-being of a patient in various aspects of life. Although it is well understood that PD is associated with changes in QoL resulting from the development of motor and non-motor symptoms, the effects of the disease on an individual’s perception of his or her social relationships, ability to work, financial status, and fulfilling life conduct have not yet been systematically studied. As a disease-related adaptation of the CHAPO model, the CHAPO-PD model considers the distinctive needs of PD patients. The important aspects of QoL and the way in which QoL can be ascertained were formulated on the basis of statements made by PD patients, caregivers, and health professionals. In contrast to questionnaires used so far, CHAPO-PD does not only consider loss of QoL due to severity of symptoms, but also offers an assessment of patient satisfaction with motor functionality and effects of treatment. In addition, resilience, defined as coping as well as positive factors in PD, can be evaluated within the scope of a QoL assessment for the first time.
The inclusion of a multidisciplinary expert panel in the development process and the supplementation of the existing CHAPO model by established PD-questionnaires is seen as a strength of the CHAPO-PD model. Though further testing is needed, the result is a comprehensive questionnaire tool whose feasibility and cognitive debriefing were tested in healthy controls and PD patients without dementia. Despite its strengths, our methodological approach also has its limitations. First, Wagner et al. originally developed and deployed their CHAPO model to assess the QoL of very old people and inclusion of patients in Western Germany. Qualifiers for QoL in older people may differ in East Germany and abroad. Second, PD patients with dementia were excluded from the feasibility study, whose QoL should also be considered within the framework of this questionnaire tool. Third, the integration of the CHAPO-PD framework into an electronic questionnaire platform, will enable a paper-free assessment from the home environment on the one hand, but may limit participation on the other.
CHAPO-PD may offer a valuable contribution to the daily clinical practice immediately, however. In response to a large aging population and the increasing prevalence of PD, new healthcare solutions that enhance functionality and QoL in PD patients simultaneously will be needed [30]. In-depth interviews with patients, relatives, caregivers, and healthcare professionals, revealed that patients were most concerned about the impact of PD on their daily lives and that healthcare professionals acting as a single point of contact are the most suitable to address and solve the PD patients’ concerns [31]. As medical consultations are typically time restricted, patients are often at risk of not being able to address and discuss all of their concerns during the course of a visit [32, 33]. In clinical practice, the CHAPO-PD could be used supplementally in order to provide a comprehensive overview of the change over time in QoL throughout the course of the disease and treatment. By offering additional valuable information, the model can help health professionals to efficiently assess the completeness and quality of medical services provided and strengthen the doctor-patient relationship by improving the doctor’s understanding of the degree of impairment of QoL in the patient. During the period time being observed, CHAPO-PD can help to identify changes in the individual’s need for support and allow the multidisciplinary treatment team to ensure the best possible and most comprehensive health care. Additionally, the digital platform will enable the questionnaire tool to be answered outside of the examination room, allowing the time saving assessment to be carried out before or even without personal medical contact. Besides that, this tool could be used in cost-effectiveness studies to estimate the relation between costs and benefits of certain interventions with respect to signs and symptoms in PD and QoL outcomes. As Rubenstein et al. indicated, for example, patients receiving pramipexole experienced higher costs, but additional positive quality-adjusted life years were gained in long term observation [34].
Ways to further improve the CHAPO-PD model in the future have already been planned. As each supplemental PD-questionnaire of the CHAPO-PD model has its own scoring rubric, a consolidated rating system will be developed that represents the objective assessment of micro- and macro-social conditions, the subjective assessment of well-being, and both the subjective and objective evaluations of health status, so that results can be interpreted and visualized as change in QoL within the digital platform. The questionnaire’s total administration time (approx. 90–120 min) may also be reduced by decreasing the total number of questions, as long questionnaires are problematic for some older adults with low vision, physical disability or serious illness; thus the duration of the scale is an important factor influencing the subjectively perceived quality of the investigation as well as patient compliance. It is for these reasons that a shortened version of the CHAPO-PD could be of importance when incorporating it into routine care or a larger longitudinal study. Moreover, the translation of the model into languages other than German will be useful to compare the QoL of PD patients from different populations and countries, particularly in the modern, globalized milieu.
In conclusion, we expect that the newly developed CHAPO-PD model will enable a holistic, longitudinal assessment of QoL in PD patients, and consequently that an improvement in individual patient care can be achieved in the long term.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank all experts who have contributed with their expertise relevant to the development of the CHAPO-PD model.
CONFLICT OF INTEREST
Franziska Thieken declares no conflicts of interest.
Lars Timmermann received payments as a consultant for Boston Scientific, honoraria as a speaker on symposia sponsored by UCB, Desitin, Boston Scientific and Abott, within the last year until March 2020. The institution of L.T., not L.T. personally, received funding by the German Research Foundation, the German Ministry of Education and Research, and the Deutsche Parkinson Vereinigung. Neither L.T. nor any member of his family holds stocks, stock options, patents, or financial interests in any of the above-mentioned companies or their competitors.
Professor Timmermann is member of the oversight Guidelines Commission of the German Neurological Society. He is participating in the Guideline of Treatment of Parkinson Syndromes. He will be the official delegate of the German Neurological Society in the EU medical devices commission and has been selected to become delegate of the German Neurological Society in the AWMF (German National Institute for Medical Guidelines).
Keywan Sohrabi declares no conflicts of interest.
Christiane Woopen declares received fees for lectures from a number of different pharmaceutical companies, but with no connection to PD.
Björn Schmitz-Luhn declares no conflicts of interest.
Anna Janhsen declares no conflicts of interest.
Carsten Eggers received in the last 12 months payments as a consultant, as a speaker, or as co-/author from Abbvie Inc. and Philyra Inc.