
Abstract
Parkinson’s disease is a neurodegenerative disorder mainly characterized by the degeneration of dopaminergic neurons in the substantia nigra. Degenerating neurons contain abnormal aggregates called Lewy bodies, that are predominantly composed of the misfolded and/or mutated alpha-synuclein protein. Post-translational modifications, cellular stress, inflammation and gene mutations are thought to trigger its pathological misfolding and aggregation. With alpha-synuclein pathology being strongly associated with dopaminergic neuronal toxicity, strategies aimed to reduce its burden are expected to be beneficial in slowing disease progression. Moreover, multiple sources of evidence suggest a cell-to-cell transmission of pathological alpha-synuclein in a prion-like manner. Therefore, antibodies targeting extra- or intracellular alpha-synuclein could be efficient in limiting the aggregation and transmission. Several active and passive immunization strategies have been explored to target alpha-synuclein. Here, we summarize immunotherapeutic approaches that were tested in pre-clinical or clinical studies in the last two decades in an attempt to treat Parkinson’s disease.
INTRODUCTION
Parkinson’s disease (PD) is the second most common neurodegenerative disorder in the world after Alzheimer’s disease (AD). PD is characterized by the degeneration of dopaminergic neurons in the substantia nigra pars compacta (SNpc), although other types of neurons are also affected [1]. Resulting symptoms are predominantly motor-related, including resting tremors, muscle rigidity, bradykinesia and postural instability [2, 3]. Several non-motor symptoms are also present and frequently appear several years before the onset of motor symptoms. They include sleep, olfactory and autonomic disorders, cognitive impairment, psychiatric symptoms, pain and fatigue (Fig. 1) [4, 5]. PD has a heterogenous clinical presentation and a complex pathogenesis. Around 15% of PD patients have family a history and 5–10% of cases are caused by monogenic mutations with Mendelian inheritance (SNCA, LRRK2, Parkin, VPS35, etc.) [6]. The remaining cases are sporadic with unknown etiology and are thought to occur following a combination of genetic and environmental risk factors [7, 8]. Despite that PD was first described more than 200 years ago [9], no disease modifying treatments are currently available. Existing therapies, solely focused on symptom management, are associated with incapacitating side effects [10].
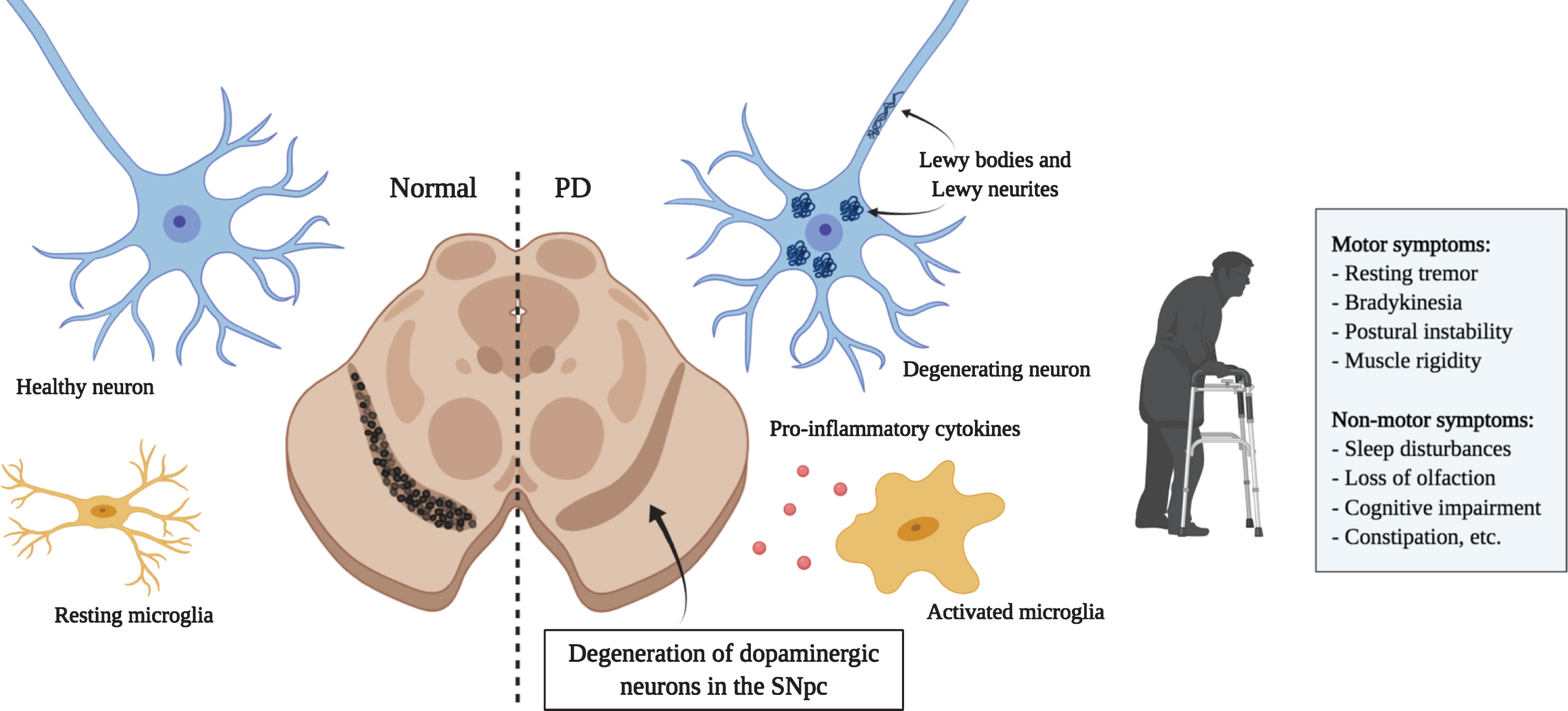
Principal hallmarks of Parkinson’s disease. Parkinson’s disease is characterized by the loss of dopaminergic neurons in the substantia nigra. Affected neurons present insoluble aggregates in their cytoplasm and neurites called Lewy bodies and Lewy neurites, respectively. These inclusions are predominantly composed of the protein alpha-synuclein. Activated microglia releasing pro-inflammatory cytokines are also present and promote an inflammatory environment possibly contributing to neuronal loss. Dopaminergic neuron degeneration leads to the classical motor symptoms. It is hypothesized that the affection of non-dopaminergic neurons in other brain regions would be responsible for the various non-motor symptoms that also greatly affect quality of life. (Created with BioRender)
Parkinson’s disease, along with Huntington’s disease (HD) and amyotrophic lateral sclerosis (ALS), is a member of a class of proteinopathies characterized by the aberrant accumulation of disordered proteins. In PD, affected neurons present insoluble inclusions in the cytoplasm and neurites called Lewy bodies (LB) and Lewy neurites (LN) [11, 12]. These aggregates are composed of multiple misfolded proteins, membranous organelles, and lipids that interfere with several cellular processes and contribute to cell death [13]. Their main component is the protein alpha-synuclein (aSyn) [14, 15]. Post-translational modifications and cellular stress are thought to trigger the misfolding of this protein and its subsequent association in toxic oligomers and fibrils [16]. Other diseases including dementia with Lewy bodies (DLB) and multiple system atrophy (MSA), gathered under the name synucleinopathies, have been associated with the aberrant accumulation of aSyn [15]. Because aSyn aggregation strongly correlates with cellular toxicity [17–19], strategies aimed at reducing aSyn burden would likely be beneficial for the treatment of these diseases as well.
Aberrant proteins are an attractive substrate for antibody-based therapies because pathological strains or aberrantly folded proteins can be specifically bound and targeted for degradation. Moreover, aSyn was shown to be present in the blood and cerebrospinal fluid (CSF) in humans [20], indicating that it can be secreted by cells. This represents a pool of proteins that could be efficiently targeted extracellularly by antibodies. Numerous pre-clinical studies using immunotherapeutic strategies have been previously explored to treat various proteinopathies including: amyloid-β and Tau for AD, mutant huntingtin protein (mHtt) for HD, and TDP-43 for ALS [21–24]. Clinical trials involving antibodies have also been carried out, notably in AD and progressive supranuclear palsy (PSP) research, with variable performances. For AD, despite promising pre-clinical results and good target engagement, most immunotherapeutic agents tested in clinical trials have until now failed to generate significant clinical improvement [25, 26]. Several clinical trials are however still ongoing. In PSP, three monoclonal antibodies targeting extracellular Tau are currently under clinical investigation. Two failed to meet the primary endpoint in phase II (ABBV-8E12 [27, 28] and BIIB092 [29, 30]), while the third (UCB0107) showed favorable results in phase I [31] and will likely be evaluated in phase II [32]. Herein, we review the therapeutic relevance of targeting aSyn for PD treatment and the different active and passive immunization strategies that have been or are currently studied in various stages of pre-clinical and clinical studies. We further assess the challenges of these therapeutic approaches and the requirements for an effective transposition to clinic.
ALPHA-SYNUCLEIN
Alpha-synuclein is a 140 amino-acid protein encoded by the SNCA gene [33]. It is abundantly and ubiquitously expressed in the brain and localized mainly at the presynaptic compartment. The family of synucleins also includes β, and γ-synuclein, that are also located in synaptic terminals [34]. Several point mutations in the SNCA gene (for example A53T, A30P, E46K, etc.) or a multiplication of the whole locus (mostly triplication) are highly associated with PD [33, 36]. Since aSyn is the main component of LB and LN, its involvement in the pathogenesis of the disease has been extensively studied. The aSyn protein can be divided in three main structural regions: a positively charged N-terminal region (residues 1–60); a central hydrophobic region (residues 61–95), called the non-amyloid-β component (NAC), which is responsible for β-sheet formation; and a negatively charged C-terminal region (residues 95–140) that is subject to numerous post-translational modifications [16].
aSyn exists in a dynamic equilibrium between a cytosolic and a membrane-bound form that influences its secondary structure. In its soluble state, aSyn is naturally unfolded and mostly monomeric. Studies have suggested that it also exists as a stable tetramer in the cytoplasm, and it is likely that both forms are present in physiological conditions [37, 38]. The N-terminal region adopts an alpha-helicoidal structure that allows it to associate to lipid membranes [39, 40]. This membrane association is necessary for the functions of the protein and prevents aggregation [41]. In a pathological context, aSyn tends to form β-sheets that aggregate, forms fibrils, and deposits in LBs [42, 43]. These toxic conformations most likely derive from the soluble and unfolded cytoplasmic protein [44]. In LBs and LNs, 90% of aSyn is phosphorylated at serine 129 (pS129) [45, 46], suggesting that this post-translational modification (PTM) plays a role in the pathological transformation of the protein. Indeed, only 4% of total aSyn is found phosphorylated in healthy individuals that lack LBs and LNs [46]. Several studies demonstrated that pS129-aSyn accelerates the formation of toxic inclusions and the loss of dopaminergic neurons in animal models [47–50]. Despite this, the role of pS129-aSyn in cell death is still debated [51]. Several other PTMs in aSyn are found in LBs, including phosphorylation at other residues, nitration, oxidation and truncation. Truncation mostly occurs in the C-terminal region of the protein and results in fragments that are more prone to fibrilization [52, 53].
The exact functions of aSyn are largely unknown. Its capacity to associate with highly curved membranes, interaction with other synaptic proteins, and localization to synaptic terminals suggest a role in neurotransmitter release [34]. Although it does not seem that aSyn is absolutely required for neurotransmission, studies showed that it regulates the clustering of synaptic vesicles at the membrane through its interaction with SNARE proteins [54]. aSyn was also found to modulate dopamine homeostasis through the inhibition of tyrosine hydroxylase (TH) expression, interaction with the dopamine transporter (DAT), and vesicular transporter VMAT2 which stores dopamine in synaptic vesicles [55–58].
PATHOLOGICAL SPREADING OF ALPHA-SYNUCLEIN
There are increasing numbers of evidences suggesting that pathologic forms of aSyn can propagate from cell to cell, and seed new LBs and LNs in a prion-like manner. According to this hypothesis, aSyn would spread following “permissive templating”— the process by which misfolded aSyn interacts with the endogenous protein, and induces its pathologic conformational change [59]. The first evidence of this process originates from the postmortem discovery of LBs in fetal tissue transplants more than 10 years after the graft in a PD patient [60, 61]. Since fetal tissue is composed of young and healthy cells, the presence of LBs suggested a transfer of toxic proteins from the recipient’s cells to the graft. As mentioned before, in humans, the presence of aSyn in plasma, brain interstitial fluid and CSF suggest that the protein can be released by neurons [20, 63]. The observation that LB pathology spreads in humans from the brainstem to the neocortex in a succession of stages further supports the hypothesis of cell-to-cell transmission [64]. In addition, aSyn-positive inclusions have been observed outside the brain, notably in the gastrointestinal track early in the disease [65, 66]. This indicates that the pathology could also spread from the periphery to the CNS.
Cell-to-cell transmission of misfolded aSyn has now been extensively studied in vitro and in animal models. Internalization of aSyn monomers, oligomers and fibrils by neurons, astrocytes [67], microglia [68–70], and subsequent recruitment of intrinsic aSyn into LBs/LNs, all have been shown in cell cultures [71] and in the murine olfactory bulb [72, 73]. Similarly, the intracerebral injection of brain homogenates from mice with aSyn pathology triggers the development of LB/LN pathology in inoculated healthy animals [74–76]. Moreover, overexpression of aSyn in the vagus nerve and inoculation of pre-formed fibrils in the hind limb muscles have been shown to trigger the formation of pathological aggregates in the SNC, indicating that pathological aSyn can indeed propagate from peripheral sites to the brain [77, 78]. The most studied mechanism for aSyn uptake is dynamin-dependent endocytosis. Since the inhibition of this process substantially reduces fibril internalization, it is proposed to be the primary mechanism involved [67, 79]. The exact cell surface receptors implicated in aSyn binding are still being studied, but lymphocyte activation gene-3 (LAG-3), neurexin 1b, Aβ precursor-like protein 1 (APLP1), and connexin-21 (CX32) gap junction proteins have been proposed as possible interactors [80, 81]. The internalization of aSyn fibrils by macropinocytosis, a clathrin and actin-dependent process consisting in the engulfment of a large amount of extracellular fluid, has also been observed [82]. The binding of aSyn fibrils to heparan sulfate proteoglycans (HSPGs) was necessary to initiate the internalization process [82]. Following endocytosis, aSyn can be transported in the axons bidirectionally, although retrograde transport is predominant [83, 84]. It is then directed to late endosomal compartments and lysosomes [67, 85]. aSyn can be degraded by both chaperone-mediated autophagy (CMA) and macroautophagy. In pathological conditions, these processes are impaired, which contributes to aSyn accumulation within cells [85–90]. In the context of exposure of healthy tissue to pathology-inducing aSyn, it is not clear how internalized aSyn fibrils escape the endosomal pathway to interact with the cytoplasmic protein. It is possible that the seeding occurs partly inside the vesicles of the autophagic pathway and that abnormal aSyn can disrupt endosomal membranes afterwards [91, 92]. Despite this uncertainty, the colocalization of exogenous and intracellular aSyn have been reported [71, 93], indicating that misfolded aSyn can effectively act as a nucleating seed. Moreover, aSyn-KO neurons are resistant to this seeding process [94]. Finally, aSyn would be released in the extracellular space by unconventional exocytosis, although the exact process is yet to be determined [95, 96]. It is also possible that aSyn is released via exosomes. However, the presence of the fibrillar form of the protein in these vesicular packages is still debated [97, 98]. The secretion of aSyn occurs in physiological conditions but is significantly increased following cellular stress (mitochondrial, proteosomal and lysosomal dysfunction, as well as oxidative stress) [99, 100]. Lastly, it has been shown in different cell models that aSyn can also move from cell to cell via tunneling nanotubules (TNTs) [79, 101]. TNTs are long, thin and dynamic membranous tubes connecting the cytoplasm of neighboring cells. They are used for intercellular communication and exchange of cytosolic material [102]. The transfer of aSyn preformed fibrils (PFFs) enclosed in lysosomes through TNTs was observed in catecholaminergic (CAD) mouse neuron-like cells and primary cortical neurons [79]. aSyn was also shown to move via TNTs between SH-SY5H cells and primary brain pericytes from PD patients [101].
Multiple strategies could potentially be employed to reduce aSyn toxicity in vivo (Fig. 2). Antibody-based therapies typically target extracellular proteins. As mentioned before, several studies have shown evidence of a substantial amount of extracellular aSyn, particularly in a pathological environment [99, 100]. Because misfolded aSyn can propagate from one cell to another, targeting this extracellular pool could be beneficial to limit the spread. However, studies have not found an agreement on which species or assembly of aSyn protein is the most toxic for cells. Whether is it best to target monomeric, early oligomeric or late fibrillar forms of aSyn is still unknown [103–107]. Most studies have used antibodies against the oligomeric form in an attempt to act earlier in the disease progression [108–111]. Antibody binding have been shown to activate microglia-mediated degradation by internalization through the Fcγ receptor [112]. Another strategy to prevent the spread of the pathology is to target the receptors to which aSyn binds, therefore preventing by competition or obstruction its entry into cells [80]. Other teams have been using nanobodies that can be engineered to penetrate cells to target intracellular aSyn [113, 114]. Since the pathological process that leads to aSyn accumulation and toxicity happens intracellularly, the ability to reach this protein pool could show promise to slow disease progression. Intrabodies, that will be described further below, can stimulate degradation through intracellular degradation pathways and/or block oligomerization and fibrillization processes. Although not discussed in detail here, another possible immunotherapeutic strategy for PD treatment consists of targeting the immune system reactivity. Neuroinflammation has been strongly associated with PD pathogenesis and correlates with aSyn toxicity. Using antibodies targeting pro-inflammatory cytokines like IL-1β and TNF-α, or preventing microglia and monocyte activation could thus be beneficial in slowing the disease progression [115, 116].
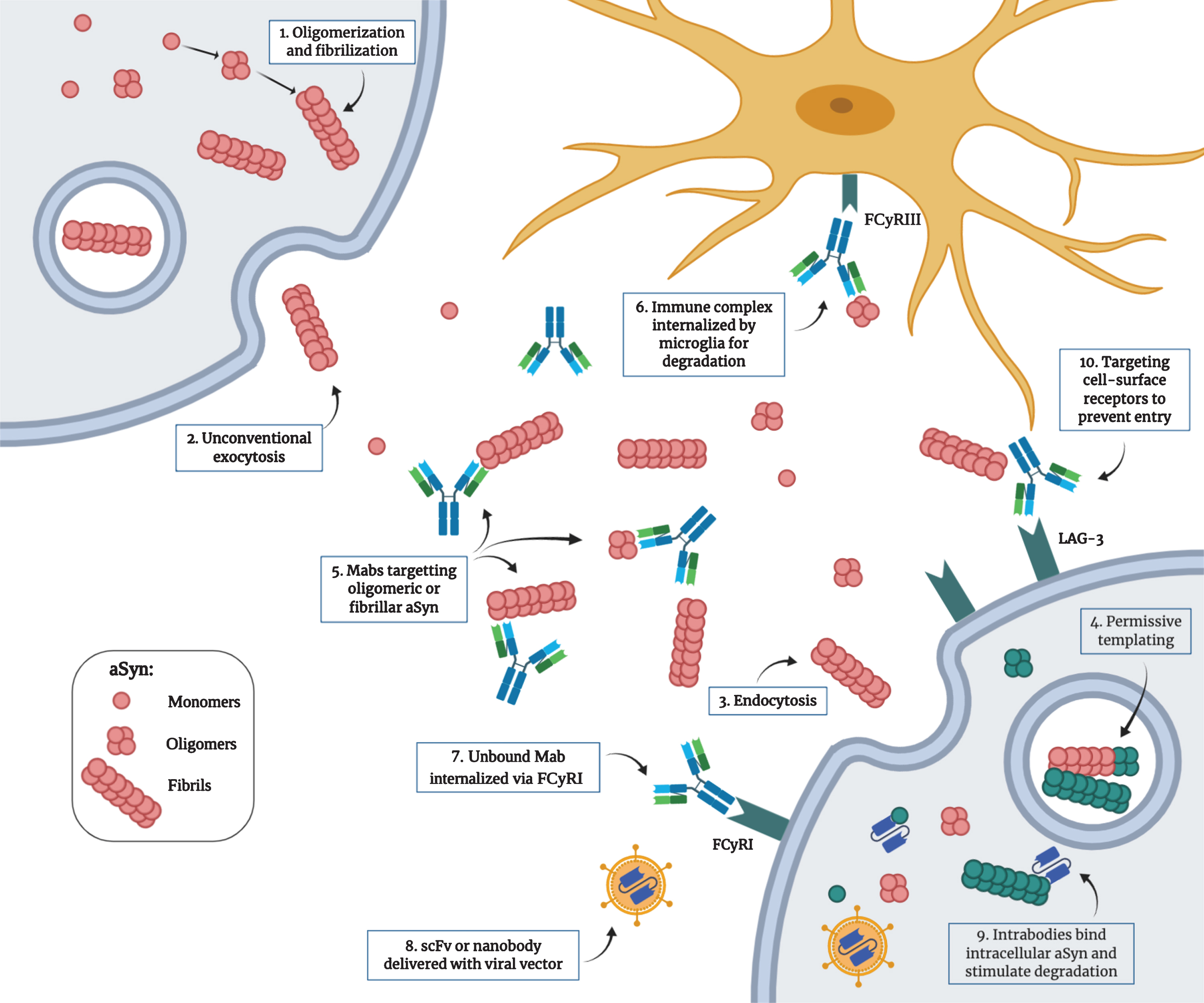
Proposed mechanism for the pathological transmission of aSyn and possible immunotherapeutic targets. 1) Post-translational modifications, cellular stress and mutations can trigger the misfolding and aggregation of aSyn into oligomers and fibrils. 2) Toxic forms of aSyn can be released in the extracellular space by unconventional exocytosis. 3) Once in the extracellular space, aggregated aSyn can be internalized by neighboring cells by endocytosis through binding of specific receptors. 4) Misfolded aSyn can act as a nucleating seed to trigger the misfolding of the endogenous protein. This process, called “permissive templating”, is thought to occur inside endosomes and lysosomes. 5) Monoclonal antibodies with different strain specificity can bind extracellular aSyn. 6) The immune complex can be internalized by microglia through the FCγRIII and is degraded intracellularly. 7) Unbound monoclonal antibodies can be internalized by neurons through the FCγRI and bind intracellular aSyn. 8) Single-chain variable fragment antibodies or single-domain antibodies (nanobodies) can be delivered as genes with viral vectors. 9) These intrabodies can target intracellular aSyn to prevent aggregation and can be engineered to be more efficient in stimulating degradation. 10) Antibodies can also target cell surface receptors used by aSyn to enter the cells (e.g., LAG3) to prevent entry. (Created with BioRender.com)
ACTIVE IMMUNIZATION
Active immunization refers to the classical vaccination strategy in which the administration of an antigen triggers the generation of specific antibodies by the immune system (humoral response). The advantage of this approach include a prolonged immune response that does not require repetitive drug administration, and is low-cost in a large-scale production [117]. However, PD is more prevalent in aged patients and immune responses are often diminished at a latter age [118]. Consequently, predicting the efficiency of an active immunization strategy in elderly patients is difficult, and variability in the response is also to be expected. Also, the active immunization against an endogenous protein has the risk of triggering an auto-immune response and neuroinflammation [119, 120]. Active immunization also implies a long-term or permanent response. Therefore, to ensure the safety of this approach, an extensive characterization of the immune response will be necessary. Studies regarding active immunization against aSyn that are discussed here are listed in Table 1. Agents that progressed to clinical trials are further described in Table 3.
Summary of the active agents discussed in this review
In 2005, Masliah and colleagues were the first to provide evidence of the efficiency of an active immunization against extracellular aSyn in a model of synucleinopathy. In their study, administration of purified recombinant human aSyn (haSyn) to transgenic (tg) mice expressing haSyn in the brain under the control of the platelet-derived growth factor-β (PDGFβ) promoter, lead to the generation of antibodies against aSyn; this reduced the toxic accumulation in cell bodies and synapses, thus preserving synapses density [121]. Antibodies were mainly targeting C-terminal epitopes of the protein and were hypothesized to bind membranous oligomeric aSyn. Because the authors observed a colocalization of haSyn and lysosomal markers, they suggested that the antibody-aSyn complex was internalized and directed to lysosomal degradation [121]. In this study, the involvement of microglia in aSyn clearance was not assessed in detail, nor was the possible immune-mediated cellular response. The authors concluded that inflammation and a cellular immunity response were unlikely since they observed only a mild microglial activation and no lymphocyte infiltration [121]. In addition, motor symptoms and possible recovery was not evaluated. It is important to note that the mouse model used in this study displayed aSyn aggregates in the temporal cortex and hippocampus, accompanied by motor and cognitive deficits [122]. Thus, this model displayed more characteristics of a DLB model than a PD model.
In 2013, Sanchez-Guajardo et al. vaccinated rats with recombinant human aSyn combined with Freund adjuvant and then overexpressed haSyn in the substantia nigra by unilateral stereotaxic injection of an adeno-associated viral vector (AAV) encoding recombinant haSyn. This resulted in a high titer of antibodies against C-terminal aSyn, reducing the number of aSyn aggregates. The authors also observed an accumulation of MHC-II- and CD4-positive microglia and a modification of their morphology, a recruitment of CD4-positive T Cells and Foxp3-positive T cells (Tregs) in the nigrostriatal system. The conclusion drawn from these results was that a protective vaccination strategy should involve a long lasting Treg response and IgG production in order to prevent autoimmunity, and to delay dopaminergic degeneration [123]. However, a drawback from this study is that the vaccination was given 10 and 6 weeks before haSyn stereotaxic injection and before any cell loss, limiting the potential transfer of these results to humans. There is no biomarker currently available to detect PD prematurely; a diagnosis is only possible after the onset of symptoms, when more than 60% of dopaminergic neurons are already lost [124]. It remains to be proven if an anti-aSyn humoral response triggered after a moderate degeneration can still have a beneficial effect in delaying the pathology.
To prevent an auto-immune response against aSyn that would impair its physiological functions, immunization with peptide fragments in lieu of the whole protein has been favored. In clinical trials, the company Affiris is assessing the efficacy of two next generation AFFITOPE® vaccines (PD01A and PD03A) which are peptides that mimic the C-terminus of aSyn. Different versions were tested by Mandler and colleagues in pre-clinical studies [125]. The most promising peptide, AFF 1, was tested in two different transgenic models of synucleinopathy: PDGFβ-aSyn and Thy1-aSyn mice. A vaccination induced the production of antibodies specific for aSyn oligomers that were able to traffic into the CNS. In Thy1-aSyn mice, the authors observed a reduced accumulation of aSyn oligomers in the SN and striatum, and a diminution in motor deficits (body suspension test). In the PDGFβ-aSyn tg mice, aSyn levels were reduced in the neocortex and hippocampus. The immunized mice also performed better in the Morris water maze after vaccination. In the same model, AFF 1 administration reduced synaptic pathology and neuronal cell death, and promoted microglial aSyn clearance and anti-inflammatory cytokine production [125]. Following these results, phase I clinical trials of the two AFFITOPE® vaccines PD01A, and PD03A, which ended in February 2015, and August 2016, respectively, assessed the safety and tolerability in early PD patients with no serious adverse effects. The treatment resulted in a robust humoral response with target engagement [126]. This allowed the development of a phase II trial.
Several other studies that analyzed the effects of active immunization against aSyn were made. Ghochikyan et al. [127] evaluated the immunogenicity of three epitope vaccines against aSyn (α-Syn85-99-P30-MAP, αSyn109-126-P30-MAP, and α- Syn126-140-P30-MAP) in mice. All vaccines were composed of a B cell haSyn epitope associated with a “non-self” T helper (Th) epitope from tetanus toxin (P30). The Th epitope P30 was used to promote an efficient humoral response by B cells. All three peptides stimulated B-cells and generated antibodies specific for the three epitopes without activating autoreactive Th cells. The antibodies generated were also able to specifically detect LB and LN in human DLB samples. However, the efficiency of these vaccines in reducing aSyn pathology and motor deficits was not evaluated [127]. Ugen et al. evaluated the efficiency of a dendritic cell (DC) based vaccination in A53T-aSyn tg mice. This strategy uses antigen sensitized DCs as the vehicle for immunization. An advantage of this approach is that DCs can serve as self-adjuvant, thus does not require the addition of an adjuvant that can result in an over-activation of the immune system. In addition, DCs can be collected autologously, which eliminates the possibility of a rejection reaction. The immunization with a peptide or full-length aSyn sensitized DCs was able to generate specific antibodies against aSyn, that ameliorated motor symptoms in mice (rotarod), and reduced the level of the pro-inflammatory cytokine IL-1α [128]. Doucet and colleagues [129] tested a vaccine based on the RNA bacteriophage (Qbeta) virus-like particle associated with short peptides of haSyn in mice. Antibodies against the C-terminal region of aSyn were generated and could effectively recognize LBs in postmortem tissue from PD patients. However, in SNCA-OVX tg mice (a mouse model expressing high levels of haSyn in a mouse Snca–/– background), the vaccination was unable to lower oligomeric aSyn burden, nor attenuate the motor deficits [129]. Finally, Rockenstein et al. [130] evaluated a novel vaccination strategy that combined active humoral and cellular immunization. They used an antigen-presenting cell-targeting glucan particle (GP) vaccine associated with aSyn and administered rapamycin (RAP) concomitantly (GP+RAP/aSyn). The vaccination of PDGFβ-aSyn mice induced high titers of anti-aSyn antibodies and an increased number of CD25 (Treg), FoxP3 (Treg) and CD4 (T cells)- positive cells in the CNS, suggesting an immunomodulatory response. The RAP-containing vaccine increased the production of TGF-β1 by Tregs, which would mediate the conversion of microglia into a neuroprotective state. The authors noted a reduction in aSyn accumulation (total pS129 and proteinase K resistant aSyn), neuroinflammation, and neurodegeneration in this model. The combination of antibody production and an anti-inflammatory effect thus resulted in a more effective vaccine, compared to humoral or cellular immunization alone [130].
PASSIVE IMMUNIZATION
In order to eliminate any danger of an auto-immune response against physiologic aSyn or unspecific targets, many teams have explored passive immunization as a novel strategy. Passive immunization refers to the direct administration of laboratory generated antibodies. This approach does not involve a humoral response and the humanization of antibodies can prevent unwanted reactions against the non-self. The dose can be closely monitored, and cessation of the treatment is possible if adverse effects appear [128]. Furthermore, antibodies can be engineered to have specific characteristics that facilitate their functions. However, passive immunization requires repetitive administration of the antibodies for as long as the treatment is needed. Delivering them to the brain is another challenge due to the blood-brain barrier (BBB). Typically, 0.1% of monoclonal antibodies administered peripherally enters the brain [131]. Several monoclonal antibodies and intrabodies that target various species of aSyn are currently at different stages of development. Monoclonal antibodies and intrabodies discussed in this section are listed in Table 2. Agents that progressed to clinical trials are further described in Table 3.
Summary of the passive agents discussed in this review
LV, lentivirus; PFF, preformed fibrils.
Antibodies previously or currently involved in clinical trials for Parkinson’s disease treatment
Complete antibodies
As for active immunization, the exogenous administration of complete antibodies is thought to target mainly extracellular aSyn. These antibodies are almost all monoclonal IgGs selected from human or murine libraries. Masliah et al. [132] investigated the efficiency of the monoclonal antibody (Mab) 9E4 directed against the C-terminus of haSyn. PDGFβ-aSyn mice received weekly intraperitoneal (IP) injections of 9E4 for 6 months. 9E4 was able to reduce the accumulation of calpain-cleaved aSyn in axons and synapses, and consequently attenuate cognitive (water maze) and motor deficits (pole test and rotarod). The study showed that 9E4 travelled into the CNS and co-localized with aSyn in lysosomes, suggesting that aSyn clearance occurred via autophagy activation. The authors proposed that the antibody recognized aSyn aggregates lying on the cell surface; the complex was then internalized and directed to lysosomes [132]. A humanized version of 9E4, PRX002 (Prasinezumab), has been developed and tested in phase I and 1b clinical trials. In healthy and mild idiopathic PD patients, the antibody showed favorable safety, tolerability and pharmacokinetics, with no immunogenicity and serious adverse effects. A significant reduction in free serum aSyn was also observed [133, 134]. Following these favorable results, a phase II clinical trial led by Roche in collaboration with Prothena started in June 2017 (PASADENA study). The study is evaluating the effectiveness of high and low intravenous doses of PRX002 in early PD patients for 52 weeks. It is intended to conclude in February 2021. Prothena released an update on Part I of the study in April 2020. Although the study didn’t meet the primary endpoint (a significant improvement over one year in the Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) total score), several secondary clinical endpoints were improved [135]. Part II of the study is still ongoing and has a year extension in which the placebo group from Part I also receives Prasinezumab.
Because the antibody 9E4 was shown to decrease the amount of truncated aSyn and reduced behavioral deficits, other antibodies targeting the C-terminal region of aSyn were tested. Games et al. [136] immunized mThy1-aSyn tg mice with 1H7 and 5C1: two Mabs against the C-terminus of haSyn. The mice received weekly intraperitoneal injections for 6 months. The authors observed: a reduction in C-terminal truncated aSyn in axons and in the loss of tyrosine hydroxylase (TH) in the striatum; an improved motor performance (beam test); and a reduction in memory deficits (water maze). In vitro, they showed that the antibody could efficiently block the cleavage of aSyn and the propagation of full-length aSyn from cell to cell [136]. Because truncated aSyn is more prone to aggregate, blocking this event is thought to slow its accumulation and propagation [137]. The antibody 1H7 was further evaluated for its ability to block the propagation of aSyn in the axons and reduce neurodegeneration in a lentivirus (LV) mouse model [138]. Non-tg, aSyn-KO, and mThy1-aSyn tg mice were injected unilaterally in the hippocampus with a haSyn-lentivirus. The IP immunization was performed weekly for three months, starting the day after LV injection. 1H7 reduced aSyn axonal transport and accumulation contralaterally. Reduced axonal degeneration and attenuated behavioral deficits in the water maze were also observed. The antibody was thought to limit the spread by binding extracellular aSyn, reducing the internalization into neighboring neurons and its association in oligomers. The authors suggest that the complex would subsequently be degraded by microglia [138].
Another C-terminal-specific Mab (of human origin) that targets both monomeric and aggregated forms of haSyn (MEDI1341) is being evaluated in a phase I clinical trial, and is intended to terminate in November 2020. The pre-clinical development of the antibody was made by Schofield and colleagues [139] and the results were published in 2019. In neuroblastoma cells (SH-SY5Y), MEDI1341 was able to block cell-to-cell transmission of aSyn PFFs, presumably by sequestering them in the extracellular space. In rats and in monkeys, this antibody could significantly and, for a prolonged period of time, reduce the level of free aSyn in the CSF. In mice, a unilateral hippocampal injection with an aSyn-encoding lentivirus, a model of aSyn spreading [138], MEDI1341 reduced accumulation of aSyn in the ipsi- and contralateral side, as well as in the trans-hippocampal axonal connexions; this suggests a blockade of cell-to-cell propagation. The IP immunization was given weekly for 13 weeks, starting seven days after LV injection. Interestingly, a version of the antibody with a mutated Fc domain that prevents its interaction with Fc receptors was as effective as the non-mutated form. This indicates that the beneficial effects of this antibody are not due to Fc-mediated mechanisms, thus do not involve microglial activation. The authors proposed that the aSyn-Mab complexes could have been internalized by neurons and degraded by the proteasome, but the exact modalities were not studied [139]. The phase I clinical trial sponsored by AstraZeneca is being conducted with the effector-null version of the antibody, and the safety evaluation of a single ascending antibody dose in healthy volunteers is ongoing.
In July 2018, the Danish company Lundbeck started assessing the safety, tolerability, and pharmacokinetics of a single dose of a human Mab against aSyn (Lu AF82422) in healthy and PD patients. The phase I clinical trial is in progress until August 2020. Another humanized Mab targeting aSyn, ABBV-0805, was developed by the company BioArctic. A phase I clinical trial that started in March 2020 aims to evaluate the safety and tolerability of increasing antibody doses in participants with PD; it is financed by the company AbbVie. The completion of this first phase is intended for November 2021. No pre-clinical data is presently available for these two candidate antibodies.
Recently, a human-derived Mab against the N-terminus of aSyn (BIIB054), selective for oligomeric and fibrillar forms of aSyn, was described by Weihofen et al. [140]. When administered IP weekly to heterozygous M83 mice (bearing a hA53T-aSyn transgene under the Prp promoter) that received an intrastriatal injection of pre-formed fibrils (PFFs), this antibody delayed the onset of paralysis associated with aSyn spreading. In PFFs-inoculated WT mice, BIIB054 reduced the level of truncated aSyn and improved the performance in the wire hang test. Finally, in A53T-aSyn tg mice, the antibody significantly reduced the loss of DAT in the striatum. In these three experiments, immunization was given two or three times before PFFs injection, and weekly following the procedure [140]. BIIB054 (Cinpanemab) was evaluated for safety and tolerability by Biogen in a phase I clinical trial. In healthy and PD patients, the antibody efficiently formed complexes with aSyn in the plasma. Thus, BIIB054 showed favorable characteristics and no serious adverse effects, allowing the development of a phase II trial [141]. This second phase is currently ongoing (SPARK study), and the completion is intended for June 2021. The study is evaluating the dose-related safety, the pharmacodynamic effects on the integrity of nigrostriatal dopaminergic nerve terminals, the pharmacokinetic profile, and the immunogenicity of BIIB054.
Numerous other teams are conducting pre-clinical studies on Mabs against aSyn. Bae and colleagues [112] tried to clarify by which mechanism(s) antibodies stimulate the degradation of aSyn in vivo. They showed that antibodies targeting extracellular aSyn mainly activate microglial degradation through the Fcγ receptor, preventing its entry in other cells, including neurons and astrocytes. Weekly intraperitoneal injections of an aSyn-targeted Mab (274) in PDGFβ-aSyn mice reduced the accumulation of aSyn in the neocortex and hippocampus, limited neurodegeneration, and reduced motor deficits in the pole test and open field [112]. Tran and colleagues [142] proved the efficiency of another Mab in a now well-established in vivo model of aSyn propagation. Antibody Syn303 was administered IP weekly to WT mice injected intrastriatally with aSyn PFFs. The immunization started immediately after PFFs injection. Immunized mice showed less LB/LN pathology in the SN and amygdala, a reduction in dopaminergic neurons loss, and less motor impairment on the wire hang test [142]. In vitro, Syn303 prevented the formation of insoluble aggregates and limited synaptic and neuronal loss. The Mab blocked PFFs entry into the neurons and consequently prevented the transmission of pathologic aSyn aggregates. In this study, the authors proposed that the pathology reduction relied mostly on the blockade of PFFs internalization since they did not observe the PFF-Mab complex inside the cells [142].
In another study by Lindström et al. [108], a protofibril-specific Mab (mAb47) was administered IP weekly to Thy1-hA30P-aSyn tg mice. Their objective was to spare physiological and functional aSyn monomers while acting on early forms of aggregates. A lower level of soluble and membrane-bound aSyn protofibrils was detected in the spinal cord, and motor symptoms were reduced. However, the mechanism by which the antibody acted (intra- or extracellularly) was not studied and no significant beneficial effect was found in the brain [108]. El-Agnaf and colleagues [143, 144] developed multiple antibodies targeting oligomeric or fibrillar forms of aSyn. They proposed that more efficient and specific effects could be achieved with antibodies that can recognize selective species of aSyn. Their Mabs Syn-O1, -O4 (oligomers-specific) and -F1 (fibrils-specific) were the most effective in the reduction of aSyn oligomer accumulation (resistant to proteinase K), and the neurodegenerational prevention in a mThy1-aSyn tg mouse model. Weekly antibody treatment also preserved the colocalization between synapsin I and synaptophysin in synapses, which is affected in aSyn tg mice and often reduced in PD and DLB patients. These improvements were found in multiple brain regions, but unfortunately not in the SN [143]. Finally, Shahaduzzaman et al. [128] generated two novel antibodies against the N-terminal (AB1) and central region (AB2) of aSyn. In rats injected unilaterally with AAV9-WT-aSyn, both antibodies significantly reduced the level of total aSyn when administered IP every two weeks for 3 months, thus protecting DA neurons against degeneration. AB1 also induced a moderate rescue in motor deficits in the cylinder test [128].
In light of the results presented so far, it appears there may be more than one mechanism by which antibodies promote the clearance of extracellular aSyn. It is possible that the neuronal uptake of unbound monomeric antibodies through FcγRI can stimulate intracellular aSyn degradation prior to cell exodus. On the other hand, antibodies bound to extracellular aSyn may participate in the clearance of the protein by increasing the internalization of immunoglobulin (Ig)-aSyn complexes into microglia through FcγRIII. Different Fc receptors have different affinities for Ig species, as well as for their monomeric vs complexed forms. FcγRI is expressed on certain neurons and is able to bind monomeric IgGs while FcγRIII is expressed solely on glial cells and can bind only complexed IgGs [112, 145, 146].
Finally, Mao et al. [80] showed that aSyn PFFs are endocytosed by neurons through the binding to lymphocyte-activation gene 3 (LAG3) on the membrane. Treating SH-SY5Y cells exposed to PFFs with two antibodies that target LAG3 (C9B7W [147] and 410C9 [148]) significantly reduced aSyn toxicity (pS129-aSyn) and cell-to-cell transmission. The same effect was found with 410C9 in primary cortical cultures from M83 tg mice (A53T-aSyn) exposed to human PFFs, or brain homogenates from 10 month old symptomatic M83 mice [80]. Thus, it appears likely that multiple receptors are involved in aSyn internalization, and that at least some are specific for particular forms (monomers, oligomers or fibrils) of aSyn. Therefore, the target of one entry mode by aSyn mono- or multimers might only partially mitigate the disease in the human pathological process. Moreover, cell surface receptors frequently have several ligands; the obstruction of these ligands could induce off-target effects by the cellular inhibition of other molecules. A thorough examination of the in vivo effects will be crucial to ensure the effectiveness and safety of antibodies that target receptors.
Nanobodies
In most species, complete antibodies are large molecular complexes made up of two different gene products in various proportions [149]. As therapeutic molecules, this large size can impair tissue penetration and offer a considerable target for the patient’s own immune system [150]. In addition to their binding domains, complete antibodies also harbor other effector domains that may prove detrimental in vivo; for instance, regions involved in complement-mediated toxicity [151]. For all these reasons, researchers try to derive smaller, safer proteins that mimic antibodies in their antigen binding. The progress in the molecular cloning and gene engineering that encode the binding domains of antibodies, coupled with the discoveries of certain high affinity animal antibody species made from a single gene product have made these goals a reality [150]
Nanobodies are of two main types: single-chain variable fragment (scFv), and single-domain nanobodies. Both have the advantage of being substantially smaller than Mabs, facilitating the crossing of the BBB and the infiltration into the extracellular space. Their small size also means the encoding recombinant DNA is small. Thus, nanobodies can fit into most viral vectors for cell transfer [152], be functionalized by addition of other function-encoding regions, or even be multiplexed (ibid). Because they lack the Fc region of traditional antibodies, nanobodies are less immunogenic and pose no risk of engaging an unwanted immune response. However, their half-life (especially for scFvs) can be considerably shorter than that of a complete antibody [152]. The scFv is composed of a polypeptide made of the antigen-binding regions of both the light, and heavy chains of an IgG antibody, attached by a flexible linker region composed of a small stretch of polar or non-polar amino acids. Their size is usually around 250 amino acids (AA). Single-domain nanobodies are even smaller (from 125 to 140 AA) [152], and are derived from a single immunoglobulin chain from a single gene product that encodes a functional immunoglobulin binding domain. This binding domain can be selected in vitro from a library made of only the heavy chains of regular IgG antibodies, or cloned from immunoglobulins of animals (e.g., Camelids) that have natural classes of antibodies composed of only heavy chains [150, 154].
Another major advantage of nanobodies is that their encoding sequence can be modified so that the nanobody can be made to be secreted like a regular antibody, or retained within the producing cell (as an intracellular antibody or “intrabody”). Cell-to-cell transmission of aSyn has only been documented in artificial models often overexpressing the protein, and clear evidence of this process has not been observed in human patients. Therefore, targeting intracellular aSyn could be an effective approach to slow down the disease progression by directly blocking aggregation and/or excretion of abnormal proteins. Intrabodies must be carefully tested for their affinity, stability, and solubility in vivo; the cellular cytoplasm is an unpredictable environment, particularly in neurons already affected by intracellular stress. Indeed, low intracellular solubility and stability is their principal disadvantage [152].
Zhou and colleagues [155] were amongst the first to test a scFv against aSyn in vitro. Their scFv, D10, binds to monomeric WT-aSyn. When transfected as a gene in HEK293 cells overexpressing WT-aSyn, D10 was able to efficiently bind monomeric aSyn intracellularly and prevent the formation of detergent-insoluble aSyn species. The antibody fragment also protected against the decrease in cell adhesion that is normally observed following aSyn overexpression [155]. Later, a scFv against the NAC region of aSyn was developed by Lynch et al. using a yeast surface display library of human scFv antibodies [156]. The antibody that showed the best affinity and viability, NAC32, was stably expressed in the cell line ST14A. When transfected with an aggregation-prone aSyn construct, cells that expressed NAC32 showed less pathological aggregation [156]. Emadi et al. [109] identified another scFv (syn-10H) from a phage display library specific to large oligomers of aSyn. The incubation of aSyn with syn-10H inhibited the aggregation of the protein, measured with a Thioflavin T assay. Added to the culture medium, it also reduced the cytotoxicity caused by aSyn aggregates in SH-SY5Y cells. Moreover, syn-10H was able to specifically recognize aSyn aggregates in human PD tissue when used as an immunohistochemical reagent [110].
The same group had previously identified from the same library another scFv binding specifically to oligomeric forms of aSyn (D5) [109]. D5 was further modified with the addition of the LDL receptor-binding domain of apoB (D5-apoB) to increase brain penetrance, cellular endocytosis, and degradation [114]. D5-apoB kept its previously described specificity for oligomeric forms of aSyn and reduced aggregation in rat neuroblastoma cells that overexpress WT-haSyn. The nanobody was encoded in a lentiviral vector and injected intraperitoneally in PDGFβ-aSyn mice. D5-apoB was thus secreted by the expressing cells. The addition of the apoB transport peptide significantly increased brain penetrance and colocalization with neuronal markers. D5-apoB decreased the accumulation of total and pS129-aSyn in the neocortex and hippocampus and reduced neurodegeneration. Accordingly, behavioral deficits were attenuated in mice that express the scFv (Morris water maze). Finally, the LDL receptor binding domain increased cellular uptake and degradation of aSyn by autophagy. The scFv-aSyn complex was imported into neurons through the endosomal sorting complex required for transport (ESCRT) pathway. The scFv colocalized with aSyn, LC3 (autophagosome marker), Rab5 (endosomal marker) and CHMP2B (ESCRT marker) [114]. This study showed strong evidence that scFvs can be effectively modified to enhance brain and neuronal penetrance as well as intracellular degradation.
Zha et al. [111] reported a conformation-specific scFv (W20) that can recognize various oligomeric assemblies of amyloid-β, aSyn, and prion protein. Purified W20 binds to a common epitope of various oligomeric structures assembled from different amyloids. Injection of the purified pan-amyloid oligomer-specific scFv could reduce motor (open field, rotarod and pole test) and cognitive (Morris water maze, object recognition test) impairments in A53T-aSyn tg mice. W20 also decreased the amount of total aSyn and pS129-aSyn, and maintained normal TH and DAT levels in the striatum [111]. These results suggest that targeting multiple abnormal proteins could be an effective strategy for neurodegenerative disorder treatments. Amyloid-β and Tau pathologies have been associated with PD dementia and also correlate with motor symptom severity, suggesting that these proteins can likely interact synergistically to worsen neurotoxicity [157–160]. Similarly, LB pathology is frequently observed in AD patients and sometimes leads to a double diagnosis [157]. Moreover, Gerson et al. demonstrated that targeting Tau oligomers with a Mab (TOMA) is protective against cognitive and motor deficits in A53T-aSyn tg mice. The reduction in Tau oligomers also prevented synaptotoxicity, and dopamine depletion in the olfactory bulb [161]. In light of these results, it would be particularly interesting to test a double-targeted strategy of Tau and aSyn in clinical trial for the treatment of PD.
Finally, Iljina et al. [162] described a camelid intrabody, NbSyn87, that binds to the C-terminal region of aSyn. Because it can bind to monomers and fibrils through the exposed C-terminus, NbSyn87 could both inhibit toxic fibril formation, and destabilize those that are already formed. Those effects could significantly reduce cellular damage [162]. NbSyn87, along with a human-derived intrabody that targets the NAC region of aSyn (VH14), was then modified with the addition of a proteasome targeting signal (PEST) [163]. The PEST motif, due to its negative charge, was used to increase cytoplasmic solubility and to stimulate degradation. When tested on different nanobodies (D5, 10H, D10, and VH14) the PEST motif was proven to be highly effective in enhancing steady-state soluble intrabody protein cellular levels, and specifically increase proteosomal degradation of the intrabody-aSyn complex [164]. In ST14A cells, both NbSyn87 and VH14 decreased aSyn levels and its related toxicity, while VH14*PEST showed a better efficiency [163]. NbSyn87*PEST and VH14*PEST were then tested in vivo in rats with a unilateral SN injection with AAV5-aSyn. The intrabodies were delivered as genes using AAV5 viral vectors three weeks after aSyn injection. Both significantly reduced the accumulation of pS129-aSyn in the SN. VH14*PEST also helped to preserve TH- and DAT-positive terminals in the striatum and showed a modest protection of DA neurons in the SN. VH14*PEST treated animals also showed a significant improvement of motor behavior in the stepping and cylinder tests compared to non-treated animals [113]. In this study, the NAC-targeted intrabody was more efficient than the C-terminus-targeted intrabody; suggesting that this region is important for aSyn aggregation. However, the two intrabodies are derived from different species (VH14 from human and NbSyn87 from camelid), which could partly explain the different outcomes.
SUMMARY AND CHALLENGES
Antibody-based therapies have been gaining increasing interest in the last few decades for the treatment of various diseases, including cancer and multiple sclerosis [165, 166]. Because antibodies can be selected and further modified to target specific protein species or conformations, they represent a promising therapeutic tool for the treatment of proteinopathies [24, 167]. Alpha-synuclein aggregation and accumulation in neurites and cytoplasm has been strongly associated with cellular toxicity in Parkinson’s disease [15, 16]. Moreover, several evidence point to a cell-to-cell transmission of misfolded aSyn through a “permissive templating” mechanism [59], which would explain the progression of the disease across the brain in distinct stages [64]. The presence of free aSyn in the CSF and plasma [20] further supports this hypothesis and has encouraged antibody development that can block extracellular transmission. Extracellular aSyn targeting should not interfere with aSyn physiological role. Both active and passive immunizations that use monoclonal antibodies or secreted nanobodies, are based on this approach. These methods have shown promising results in pre-clinical studies and some are being evaluated in phase I and II clinical trials. Active immunization has the advantage to be a long-term therapeutic option. However, the inability to accurately predict the immune response generated, especially in elderly patients, limits its applicability. Another drawback of this approach is the possible autoimmune response and neuroinflammation, as was observed in clinical trials for Alzheimer’s disease [168]. For this main reason, current studies mostly focus on passive immunization. This strategy does not pose the same level of immunogenic risk with the use of human or humanized antibodies (or nanobodies), and is easily reversible. How exactly these reagents promote toxic aSyn clearance is unknown, but multiple mechanisms are likely involved. Microglial activation has been shown in some cases. Internalization of the immune complex by neurons with subsequent intracellular degradation was also shown. It is possible that the binding specificity of the immunotool for certain mono, oligo, or higher-level assemblies of aSyn influences the type of degradation induced. In any case, a closer evaluation of the immune (cellular and humoral) response will be important to ensure the safety of any antibody-based therapy.
Studies that evaluated the prion-like transmission of aSyn were made in artificial models that overexpressed the normal or mutant protein; it is still unclear if this mode of transmission actually occurs in the human brain. Therefore, it is possible that intracellular aSyn would be a better target to achieve neuroprotection. Given that misfolding and toxic accumulation of aggregated aSyn originates inside the cells, blocking the initial protein oligomerization and fibrilization could provide a new strategy. Furthermore, intracellularly active nanobodies have the potential to stimulate the degradation through autophagy or proteasomal pathways. Along with their low immunogenicity, intrabodies are particularly attractive candidates for antibody-based therapies against aSyn. Their main disadvantage is the poor stability in the reduced environment of the cytoplasm. However, they can be easily modified to overcome this flaw with the incorporation of specific sequences [164].
The precise mechanisms underlying cell death in PD are still unclear. Mitochondrial, proteasomal, and autophagy dysfunctions are likely involved, but the sequence of events and the role of aSyn aggregates in these processes are not well established. aSyn has been shown to exist as a wide range of oligomeric and fibrillar assemblies. Typically, the protein initially forms an aggregation nuclei that acts as a seed for the elongation into protofibrils by the addition of monomers. These protofibrils then associate into mature amyloid fibrils [169, 170]. The term “oligomers” encompasses species with a variety of molecular weights and secondary structures. This heterogenicity, as well as their instability, renders them difficult to study, particularly in vivo. The term “fibrils”, on the other hand, refers to long, ordered, insoluble and compact fibril assemblies enriched in beta-sheet structures. aSyn fibrils can have various shapes (cylindrical-fibrils or flat-ribbons) and lengths [172–174]. Several studies have suggested that oligomers, rather than fibrils, could represent the major toxic assembly of aSyn rather than a simple intermediate in fibril formation [104, 175–177]. Lewy pathology is present in a surprisingly high proportion of postmortem brains from people without any neurological disorder [178, 179]. Also, the extent of LB deposition does not correlate with the severity of symptoms in several PD patients [180, 181]. Some patients with a clinical PD diagnosis do not even present Lewy pathology [182]. These elements suggest that the fibrils contained in LBs may not represent the major pathological strain of aSyn. However, several studies showed that fibrils are toxic to neurons as well [107, 184]. Moreover, their capacity to act as nucleating seeds for the pathological misfolding and aggregation of aSyn and their role in the cell-to-cell transmission of the disease still make them a very toxic species [93, 94]. Thus, there is no consensus regarding which strain of aSyn is the most toxic. It is likely that a variety of species exert different toxic effects in cells and their combined actions result in cellular malfunction and death. Due to the persistent uncertainty of which aSyn species is the most harmful, it is unclear at what stage to intervene in the toxic assembly process for optimal neuroprotection. Researchers should pay particular attention to which strains of aSyn are present in their models, and in immunotherapeutic studies, against which strain is their antibody directed. This would allow a better understanding of aSyn cellular toxicity. Proximity-ligation assay against aSyn can be used to detect oligomers with a high specificity and probably represent the best technique to distinguish between LBs/fibrils and early oligomers [185]. Multiple models should also be used to test target engagement and behavioral outcomes.
Several pre-clinical antibodies have been shown to reduce the level of total aSyn in vitro and/or in vivo. Since some studies have shown that the knockout or subthreshold knockdown of this protein alters DA synthesis and release, and can induce DA neuron degeneration in the SN [186, 187], it will be important to decipher in detail the important biochemical role that aSyn plays in healthy DA neuron survival [186]. aSyn is also implicated in regulating the synaptic vesicle pool during neurotransmission [188]. Thereby, it will be crucial to ensure that nanobodies against intracellular aSyn do not prevent this role and negatively affect DA neurotransmission in surviving DA neurons, which could worsen the patient’s motor symptoms. The ability to exclusively target the pathological species of aSyn (oligomers, fibrils, pS129, or truncated aSyn) would be a very desirable property to avoid this outcome.
Finally, another challenge in the clinical development of antibody-based therapies against aSyn is the absence of a reliable diagnostic tool to assess the disease progression. PD diagnosis relies solely on clinical signs and symptoms, medical history and neurological and physical examinations [10]. A good diagnostic marker would be important for two main reasons: to ensure that patients enrolled in clinical trials are at an expected stage of disease progression, and to evaluate if the treatment leads to a sufficient target engagement. First, since clinical signs and symptoms are highly variable between patients, the precise assessment of LB/aSyn pathology in the brain is challenging. Moreover, a small proportion of patients with clinical PD do not present Lewy pathology— a situation mainly seen with Parkin and LRRK2 mutations [10]. It is thus possible that patients that lack LBs could be included in clinical trials. Conversely, patients with severe aSyn burden and neuronal loss could be included as well. In both cases, antibody therapy may not prove any functional benefit, which would undesirably alter the clinical trial results. Also, the possibility to perform a genetic analysis could result in the exclusion of patients with specific mutations in the clinical trial recruitment. Additionally, a diagnostic tool that allows early diagnosis of PD, before extensive neurodegeneration, would permit a presumably more successful intervention in terms of disease progression, symptoms reduction, and quality of life improvement. Second, to properly evaluate if the antibody is to effectively engage its target and promote degradation, a reliable non-invasive method must exist to detect total aSyn levels and/or aggregates. Unlike amyloid-β and Tau, no validated PET-tracers currently exist to detect aSyn in the brain, despite various development efforts [189, 190]. Imaging modalities will demand careful evaluation for their resolution, i.e., their correlation with the extent of proteinopathy and strain specificity. Standard rating scales to assess PD symptoms, as the Unified Parkinson’s Disease Rating Scale (UPDRS), and striatal binding ratio with DATscan, are not adequately precise to determine the effectiveness of an antibody treatment. Finally, the detection of free aSyn in serum or CSF is commonly used in clinical trials but lacks a validated correlation with clinical outcomes. The ability to specifically detect aggregation-prone aSyn species in the CSF or brain biopsies would however be highly valuable. The Protein-Misfolding Cyclic Amplification (PMCA) and the Real-Time Quacking-Induced Conversion (RT-QuIC) are protein amplification assays that can detect misfolded protein aggregates. Both have shown a high sensitivity and specificity in detecting pre-clinical and clinical synucleinopathies in preliminary studies [191].
CONCLUSION
In conclusion, antibody-based therapies against aSyn promise a new therapeutic approach for Parkinson’s disease. Antibodies could be effective to reduce the aberrant accumulation of aSyn and limit the cell-to-cell transmission. Both passive and active immunization have shown enviable results in clinical trials so far, but clinical/functional recovery is yet to be proven. The development of a reliable imaging strategy or biochemical marker for the assessment of synucleinopathy will be important to monitor clinical trials effectiveness. Moreover, a better understanding of aSyn disorganization, aggregation and related toxicity, along with a clarification of its cell-to-cell transmission mechanism will greatly help developing efficient antibodies.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
Footnotes
ACKNOWLEDGMENTS
A.-M.C. is supported by a scholarship from the Neuroscience Thematic Research Centre. M.L. receives salary support from Fonds de Recherche du Quebec-Sante, Chercheur-Boursier Juniors 2 in partnership with Parkinson Quebec (34974). We also thank Modesto R Peralta III for help in revising the manuscript.