
Abstract
Parkinson’s disease (PD) is a common neurodegenerative disorder, with a continuously increasing prevalence. With improved clinical and therapeutic management of PD, more patients reach later stages of the disease, meaning they may face new clinical problems that were not commonly approached. This gave way to the description of a new PD stage, late-stage PD (LSPD), which is clinically discernible from the advanced-stage one. Therefore, LSPD patients have new and different needs, regarding pharmacological and non pharmacological interventions, including palliative care and multidisciplinary teams. LSPD patients constitute an‘orphan population’, who traditionally was excluded from previous studies, due to its high disability. With this manuscript, we intend to review specific management challenges of LSPD patients, covering this new concept and its clinical features, how to assess these patients, therapeutic recommendations, as well as discussing ongoing research and future perspectives.
INTRODUCTION
Parkinson’s disease (PD) is the second most common age-related neurodegenerative disorder after Alzheimer’s disease, and its prevalence is expected to increase up to 12.9 million by 2040 [1]. As a reflection of increased life expectancy and a better clinical management, the number of old PD patients or patients with a more prolonged disease course is estimated to increase, carrying a higher burden of disease for patients, caregivers, and healthcare systems [2]. The aim of this viewpoint is to illustrate the main clinical features, treatment challenges and future research perspectives for late-stage (LS) PD patients, a recently described PD stage, which actually represents an “orphan population”, usually not included in clinical trials or observational studies, due to its great disability [2].
PARKINSON’S DISEASE STAGING
PD motor progression is non-linear (Fig. 1) and more pronounced in patients with cognitive dysfunction or older age at onset [3] and faster in the LS if compared to the advanced one [4].
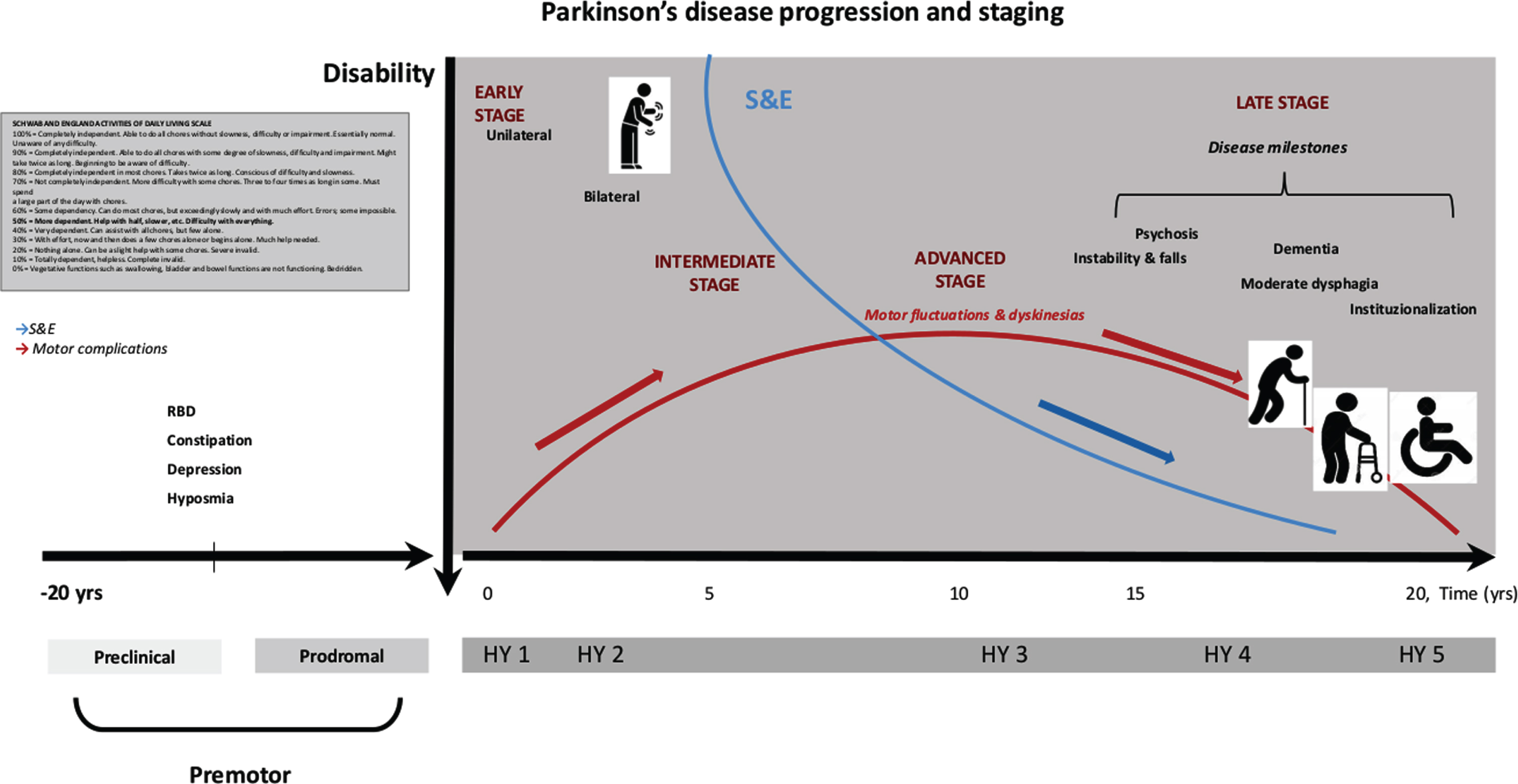
PD staging progression.
Classically, PD progression is marked by the severity of motor symptoms, appearance of patients’ physical dependence and motor complications (MCs), whose severity classically define the beginning of the advanced PD stage [5, 6], as well as reaching a Hoehn and Yahr stage (HY) of 4 or 5 in the “Med Off” condition [4]. However, it may occur that patients displaying different disease severities, may be included in the same HY stage, as the HY does not consider the presence of non-motor symptoms (NMS) or MCs, whose prevalence increase with disease progression [7]. Indeed, besides MCs, PD patients in advanced stage also manifest several NMS and axial motor features, such as postural instability, freezing of gait (FoG), falls and dysphagia [6, 8] (Fig. 1).
LATE-STAGE PARKINSON’S DISEASE CONCEPT AND CLINICAL FEATURES
In the last two decades, it has been observed that a small subset of advanced PD patients progress to a later phase of the disease, clinically discernible from the previous one [2]. LSPD patients usually present a severe bradykinesia with reduced or absent appendicular rigidity [9, 10]. Disability from MCs is reduced, because these complications attenuate naturally, either due to levodopa treatment reduction or in response to device-aided therapies [11, 12]. Conversely, disability is related to a cluster of variables that consists of NMS, as cognitive impairment, psychosis, depression, daytime sleepiness, autonomic dysfunction, and axial symptoms poorly responsive to levodopa. Taken as a whole, we have a “late” phenotype whose clinical features do not really fit with the common concept of idiopathic PD, but rather sharing common clinical elements with atypical parkinsonisms (Table 1) [2, 13].
Late-stage PD: clinical and therapeutic key points
Level of evidences as reported by Seppi et al., 2019 [24]; Fox et al., 2018 [22], Ferreira et al., 2013 [23]. (§) Efficacious, (∧) Likely efficacious, (∞) unlikely efficacious, («) insufficient evidence, (+) clinically useful, (#) possibly useful, (x) investigational; (GPP): Good practice point; Level C: based on non-comparative trials; PD, Parkinson’s disease; HY, Hoehn & Yahr scale; S&E, Schwab and England Activities of Daily Living scale; FoG, freezing of gait; MMSE, Mini-Mental State Examination; NMS, non motor symptoms; NPI-12 items, The Neuropsychiatric Inventory Questionnaire; NMSS, Non-Motor Symptoms Scale for Parkinson’s Disease; QoL, quality of life; PDQ-8, Parkinson’s Disease Questionnaire-8; ESAS, Edmonton Symptom Assessment Scale; L-dopa, levodopa; DA, dopamine agonists; IMAO-B, Monoamine oxidase B inhibitors; COMT-I, Catechol-O-methyltransferase inhibitors; SSRI, selective serotonin reuptake inhibitors; SSNRI, selective serotonin norepinephrine reuptake inhibitors; LSVT, Lee Silverman Voice Therapy; BoNT, botulinum toxin injection; EMST, expiratory muscle straightening training; FEES, fiberoptic endoscopic evaluation of swallowing; VFSS, video fluoroscopic swallowing study; VAST, video-assisted swallowing therapy; TTS, thermal–tactile stimulation; CPAP, continuous positive airway pressure; OSA, obstructive sleep apnea; PC, palliative care.
Which are the most relevant clinical problems?
Four principal disability milestones, i.e., symptoms of disease progression that should draw additional medical attention, have been identified to precede death by around 5 years, independently from disease duration and age of onset: visual hallucinations (5.1 years), falls (4.1 years), dementia (3.3 years), and institutionalization (3.3 years) [14]. Other recognized red flags for a poor outcome are the need for a formal caregiver and the presence of swallowing problems [4]. The presence of dementia predicts a blunted or absent levodopa response [15], though such a milder levodopa responsiveness does not seem to be a risk for death [4] (Table 1).
Who is affected?
LSPD disability has a major impact not only on patients’ quality of life (QoL), but also on relatives and/or caregivers, who carry themselves a high physical, psychological and socioeconomic burden. Failure to acknowledge and properly manage caregivers’ burden may ultimately lead to burnout, diminishing their effectiveness and capacity to maintain their informal partner role in treatment, therefore creating an “invisible patient”. This may also lead to premature institutionalization of such patients, with an associated cost increase [16].
INSTITUTIONALIZATION AND MORTALITY
Around 20% of LSPD patients are institutionalized [4, 18], usually in nursing homes and not in assisted living facilities, as they are mostly dependent in activities of daily living (ADLs), needing medical care and supervision. Psychosis is a risk factor for institutionalization, with 25% of PD patients with psychosis being institutionalized vs. one in ten patients without psychosis [19].
Pneumonia and food aspiration are listed among the most frequent death causes [4], which is influenced by older age, dementia and severe axial symptoms [20, 21]. However, no study has specifically assessed mortality causes among LSPD patients, as it may frequently happen that those frail patients are no longer followed by their treating physician during the last years/months of life.
THERAPEUTIC RECOMMENDATIONS
Pharmacological treatment
No randomized controlled clinical trials (RCTs) specifically addressed LSPD patients as a target population. Hence, a scarce amount of systematic data exist for the treatment of motor and NMS of LSPD patients, and treatment recommendations are frequently based on expert opinions and good clinical practice (Table 1) [24]. Table 1 summarizes the pharmacological and non-pharmacological interventions for the most common motor and NMS of LSPD, based on the Movement Disorder Society (MDS) Evidence-Based Medicine (EBM) Reviews or the European Federation of Neurological Society guidelines [22–24]. However, those recommendations are based on RCTs that classically do not include LSPD patients [25].
Overall, levodopa is the gold standard of PD treatment, even in LS (Table 1) [4, 27]. LSPD tremor dominant patients, with no dementia and who still present MCs have the better responsiveness profile and may benefit from a cautious dose increment, when clinically indicated [15, 26]. Additionally, due to the frequent occurrence of adverse events (AEs) induced by anti parkinsonian drugs, a regimen simplification of treatment strategy, based on the unique use of levodopa and drugs for psychosis/dementia is recommended [10]. Conversely, no acute effect of levodopa has been observed on several NMS, such as pain, anxiety, fatigue and axial symptoms, i.e., speech, postural instability, posture and FoG [4, 29]. On a related note, a mild acute response should not be translated into a levodopa ineffectiveness nor in recommendations for drug suspension or decrement, in absence of AEs. The levodopa “long-duration response” should be taken into account, even in this latest stage [30].
Nonpharmacological treatments
Considering the last MDS-EBM update [22] on treatments for PD motor symptoms, with the exception of physiotherapy which is “likely efficacious”, exercise-based movement strategies, formalized pattern exercises, speech therapy, and occupational therapy, were all deemed “possibly useful”, not with standing insufficient evidence regarding efficacy, to date (Table 1) [22].
Within the non-phamacological approaches for LSPD we believe that it is worth to consider also palliative care (PC) and health-care models.
Palliative care
PC includes a broad range of “aims to improve the QoL of patients and their families with life-threatening illness” (Table 1). PC no longer restricts to “end-of-life care”, seeking to appease suffering along the entire course of the illness [31]. Given the complex clinical picture of LSPD patients, an implementation of PC interventions is desirable, integrated with traditional care and variably delivered as inpatient or outpatient PC, hospice care or at home PC nursing, in agreement with patients’ needs. Additionally, advance care planning, a component of PC, which provides a vehicle through which patients, families, and clinicians can collaborate to identify values, goals, and preferences regarding future medical care, could be particularly helpful. Indeed, LSPD patients often present with all the red flags for unmet PC needs, which should “trigger” specialized PC referral. These that are: swallowing problems, recurrent infections, marked decline in physical function, first aspiration pneumonia, cognitive difficulties, weight loss and significant complex symptoms [32]. Identifying these red flags could help with the practical application of integrated models of care.
Health care models
The complex clinical picture of LSPD patients suggests adoption of an individualized and multispecialty care approach. Multispecialty models of care can be organized as: a) multidisciplinary care: each discipline is responsible for a specific patient need without a standardized coordination; b) interdisciplinary care: healthcare team members collaborate and make group decisions; c) integrated care: a care plan involving multiple members of a healthcare team is guided by consensus building and engagement of patients as team members [33–35]. However, results of past trials on both multidisciplinary or integrated care models have suggested heterogeneous results, from no change to a small/moderate benefit in QoL [36–38], though no trials on integrated care were specifically addressed to LSPD patients. Of note, a recent observational study on a home visit care model has found a good satisfaction and feasibility of the model, even among HY 4–5 PD patients [39].
HOW TO ASSESS LATE STAGE PD PATIENTS
A proper assessment of a LSPD patient should be always made in co-presence with the principal formal or informal caregiver, due to the high prevalence of dementia. A Schwab and England Activities of Daily Livingscale <50% has been proposed as operational clinical criterionto identify LSPD patients (Fig. 1) [2].
Healthcare professionals should actively investigate, the presence of falls, hallucinations, choking episodes, cognitive decline, sleep and urinary disturbances. Among those symptoms, swallowing problems should receive particular attention, and a prompt assessment by a phoniatrician should be considered on a regular basis. To date, no specific questionnaires have been created for demented LSPD patients. However, a European multicenter study has been recently developed (see below) [40] with the aim of characterizing a large population of LSPD patients; questionnaires adopted in this study may be considered as a sort of guideline to assess these patients (Table 1).
BOTTLENECKS
LSPD patients’ assessment and treatment reflect a long list of clinical unmet needs [41]. Most of the instruments available to assess LSPD patients seem to be partially adequate or mostly inadequate, probably because clinometric properties of such scales have not been specifically tested among LSPD patients, who are difficultly testable due to dementia, behavioral disorders and severe dysarthria. Equally, non-pharmacological interventions are not adapted to these frail and demented patients. This is one of the reason why, when we extrapolate data of HY 4–5 patients from small trials on multidisciplinary or home-based exercise and strategy training, no improvement is found, for instance, on ADLs or falls [41, 42]. Additionally, the neuropathology of levodopa unresponsive motor or NMS, remains largely undefined, besides the fact there are no new marketed drugs that properly target those symptoms [43]. Finally, the management of LSPD patients previously submitted to device-aided therapies may be particularly challenging, with no guideline available to help clinicians to manage this sub-group of LSPD patients, including the possible discontinuation of on-going advanced therapies.
ONGOING RESEARCHES
Several clinical studies and trials are currently ongoing on LSPD.
The results of a longitudinal, multicentre, prospective cohort study, i.e., Care of Late-Stage Parkinsonism (CLaSP),which assessed the needs and provision of care for patients with LSPD and their caregivers in six European countries (UK, France, Germany, Netherlands, Portugal, Sweden) will be shortly published [40]. A PC model that could be integrated in traditional care is also being evaluated in a multinational European project (http://www.pdpal.eu), though it will not focus only on LSPD. In UK, OPTCARE Neuro, a multicentre RCT evaluating the short-term effectiveness of short-term integrated PC in long-term neurological conditions, including PD, is ongoing [44]. In the USA, a randomized multicentre, comparative effectiveness trial of team-based outpatient PC versus usual care for PD patients with moderate to severe PC needs, has begun [45]. Another trial on interdisciplinary home PC model (IN-HOME PD; NCT03189459), focused on HY3–5 homebound PD patients, is currently ongoing in the USA, and will be completed in late 2020. Finally, the results of an Italian multicentre study that has explored the effect of deep brain stimulation among LSPD patients, in order to develop a decisional algorithm to rule a possible stimulation discontinuation, will be shortly published.
FUTURE PERSPECTIVES
Researches on the LSPD domain should be focussed on several targets and steps: a) basic research: to develop non-dopaminergic drugs that may tackle the extra-dopaminergic dysfunction, and improve the tolerability profile of anti parkinsonian agents; b) clinical assessment and non-pharmacological treatments: develop adapted assessment tools and rehabilitation strategies for demented homebound LSPD patients; c) environment: to consider the family caregiver as well as the environment as therapeutic targets; d) healthcare models: based on the shortcomings of the present institution-based medical approach [46] and the frequent need for LSPD to be visited at home [4], this population could be the proper target for an in-home integrated care trial.
Overall, an effort should be made to include LSPD patients in clinical studies, as this “orphan population” is likely to increase, and may represent a model to tackle disability milestones of neurodegenerative diseases.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
Dr. Margherita Fabbri: grant from AbbVie. Dr. Kauppila: nothing to disclose. Professor Joaquim J. Ferreira: Consultancies: Ipsen, GlaxoSmithKline, Novartis, Teva, Lundbeck, Solvay, Abbott, BIAL, Merck-Serono and Merz; Grants: GlaxoSmithKline, Grunenthal, Teva and Fundação MSD. Professor Oliver Rascol: Advisory Boards and Consultancy: AbbVie, Adamas, Acorda, Addex, AlzProtect, Apopharma, Astrazeneca, Axovant, Bial, Biogen, Britannia, Buckwang, Cerespir, Clevexel, Denali, INC Reasearch, Lundbeck, Lupin, Merck, MundiPharma, Neuratris, Neuroderm, Novartis, ONO Pharma, Osmotica, Parexel, Pfizer, Prexton Therapeutics, Quintiles, Roche, Sanofi, Servier, Sunovion, Théranexus, Takeda, Teva, UCB, Vectura, Watermark Research, XenoPort, XO, Zambon; Grant: Agence Nationale de la Recherche (ANR), CHU de Toulouse, France-Parkinson, INSERM-DHOS Recherche Clinique Translationnelle, MJFox Foundation, Programme Hospitalier de Recherche Clinique, European Commission (FP7, H2020), Cure Parkinson IK; Other: Grant to participate in a symposium and contribute to the review of an article IPMDS.
Footnotes
ACKNOWLEDGMENTS
The present study has no funding.