
Abstract
Background:
Patients hospitalized with Parkinson’s disease (PD) require timely delivery of carbidopa-levodopa (C/L) medication. Ill-timed administration of C/L doses is associated with greater morbidity and longer lengths of stay.
Objective:
To understand the barriers to timely C/L administration, and implement strategies to improve the administration of the drug to hospitalized PD patients.
Methods:
Several key strategies were employed in 2015 to improve the timely delivery of C/L doses: 1. three kinds of nursing alert in the electronic medical record (EMR); 2. staff in-service education; 3. stocking immediate-release C/L into automated medication dispensing machines on key hospital units; 4. reports to nurse unit managers on timeliness of C/L administration; and 5. reconciliation of inpatient and outpatient levodopa orders by the hospital pharmacist upon admission. The primary outcome was the percent of C/L doses administered within 60, 30, and 15 minutes of scheduled time.
Results:
Our urban hospital, affiliated with a Parkinson’s Foundation Center of Excellence, had 5,939 C/L administrations in 2018. There was sustained improvement in timely delivery of doses, from 89.3% in 2012 to 96.5% in 2018 (within 60 minutes of the scheduled time), 65.5% to 86.4% (30 minutes), and 42.3% to 71.1% (15 minutes) (all p < 0.001).
Conclusions:
With multifaceted but relatively simple measures, we were able to “change the culture” so that hospitalized patients with Parkinson’s disease receive levodopa on time.
INTRODUCTION
Parkinson’s disease (PD) is a common chronic neurologic disease affecting an estimated one million Americans, a number expected to double between 2005 and 2030 [1]. Previous studies have shown that people with PD are hospitalized more frequently than people without PD [2, 3] and that there are obstacles to providing adequate care [4]. Hospitalized PD patients have longer lengths of stay [3], and a greater risk of in-hospital complications such as falls, delirium, and mortality than comparable patients without PD [3, 5]. These observations led Low et al. [3] to conclude that “urgent attention should be given to developing cost-effective interventions to reduce the burden of hospitalization for patients, caregivers, and healthcare systems.”
The reasons for hospitalization in people with PD vary depending on the type of hospital and data analysis [6–10]. One critical challenge for the hospitalized PD patient is the proper administration of anti-Parkinson medications [4]. Medication regimens for PD can be complex, due to the use of multiple anti-Parkinson medications, the need for frequent dosing of carbidopa-levodopa (C/L) preparations, or both. As the disease progresses, PD patients may require C/L dosing as often as every 1–4 hours, with dramatic consequences on mobility and function when the medication benefits have worn off (including symptoms such ranging from “freezing of gait” to complete immobility, dysphagia, tremor, dystonia, shortness of breath, and anxiety). An influential review published in 2010 by the National Parkinson Foundation (now the Parkinson’s Foundation [PF]) Working Group on Hospitalization in Parkinson’s Disease highlighted the challenges for hospitalized PD patients [6]. A survey conducted by this group showed that 94% of physician respondents from PF Centers of Excellence were “not confident” that patients were receiving PD medications on time in their own hospitals [11]. A similar survey in the UK found that 61% of surveyed providers were “not confident” that medications were being given properly in the hospital [12]. A recent retrospective study found that 29.5 percent of scheduled C/L doses were given late (defined as more than an hour after the scheduled time) or not at all, and that patients whose C/L doses were all given on time (28.2% of patients) had substantially shorter hospital stays than those who had one or more late or missed doses (an average of 3.6 days vs 8.2 days) [13]. A study of post-surgical patients found that 25.7% had to remind hospital staff that they were due for medication, and 79% of those patients complained of post-operative confusion or worsening of PD compared to only 38% of those who did not have to prompt staff for their medication (p < 0.001) [14].
Additional studies have documented late or missed dosing of PD medications [15–22], use of medications contraindicated in PD [13, 23], or both, occurring in 39% to 90% of PD admissions. Longer hospital stays and other complications have been associated with incorrect dosing [13, 22], as has poor patient satisfaction with medication administration [24, 25]. Gerlach et al. [20] identified medication errors as the most important risk factor for motor function deterioration for PD patients during hospitalization. We describe below the actions and effects of a quality improvement initiative to enhance the safety and timeliness of medication administration to inpatients with PD in our affiliated hospital.
MATERIALS AND METHODS
Description of the setting
Struthers Parkinson’s Center (SPC) is a PF-designated Center of Excellence treating about 2000 individuals with Parkinson’s disease and related conditions. Park Nicollet Methodist Hospital is an affiliated 361-bed hospital, with medical admissions generally managed by hospitalists, utilizing neurology consultation as needed. Park Nicollet Methodist Hospital and SPC share an electronic medical record system (EMR), so that outpatient prescriptions, medication schedules, and notes written by SPC physicians are immediately accessible to the hospital team.
Consent was not obtained from subjects at the time that data were collected/analyzed as this was a quality improvement initiative. When the decision was made to publish the results, the project was submitted to the HealthPartners Institutional Review Board for review, which determined that no additional consent was needed to proceed. This project did not receive any specific grant support from funding agencies in the public, commercial, or not-for-profit sectors.
Quality improvement activities
The initiative included participation of SPC physician, nursing, and rehabilitation leaders; patients and families; and Park Nicollet Methodist Hospital administrative leaders, hospitalists, nursing (nursing administrators, nursing education, nursing informatics, and floor nursing), pharmacy director, rehabilitation therapists, discharge planners, and the EMR information technology team.
In late 2012,we began to receive a report, created through the EMR, of patients receiving C/L products during a hospital admission. After two years of baseline data collection and planning, interventions were carried out in 2015.Brief educational presentations were given to physician hospitalists, inpatient nurses on key units, and hospital-based rehabilitation therapists about PD in general, challenges for the hospitalized PD patient, and the importance of timely delivery of C/L products. The internal Park Nicollet Methodist Hospital Pharmacy and Park Nicollet Methodist Hospital Nursing monthly newsletters featured brief articles about the initiative. A quarterly C/L compliance scorecard was circulated to the pharmacy director, nursing education director and hospital unit nurse managers which indicated the percent of C/L doses administered within 15 minutes.
EMR interventions were developed, which provide standardized prompts for nursing teams across all the inpatient units. The initial interventions were focused around medication management workflows and a later intervention was around transition communication workflow.
Nurses review each patient’s Medication Administration Record (MAR) at the beginning of each shift to identify special needs or requirements for each patient. The time of administration of each medication is recorded in the MAR using a bedside barcode scanner; the MAR then serves as a basis for data abstraction. An EMR alert was created within the MAR, which serves as a time-sensitive reminder if a C/L dose is 15 minutes late (later modified to an alert 1 minute after a dose is scheduled).To convey a sense of urgency, the alert color is red. In addition, the instructions that accompany the listing of Parkinson’s medications in the MAR now include a statement that the patient has a diagnosis of PD and should receive PD medications within 15 minutes of the scheduled time.
Both of these interventions were developed to improve medication administration workflows. EMR-embedded alerts thus provide both an at-the-moment reminder of a C/L dose due for delivery and continuous education for nurses that PD patients require timely medication administration. Neither alert requires acknowledgement by the nurse, to minimize “pop-up fatigue”.
Based on nursing team recommendations, a final visual reminder was created to help with shift-to-shift communication workflow. The EMR includes a Situation-Background-Assessment-Recommendation (SBAR) that nursing team members use to enhance handover communication. The nursing team members use the SBAR at the start of their shift and the just-in-time message sets them up to understand their patients’ unique needs. A reminder automatically populates the SBAR, based on the presence of an order for C/L, to remind the nurse that the patient has a diagnosis of Parkinson’s and that time-sensitive medication administration is imperative.
In late 2015, immediate-release C/L products were stocked into automated dispensing machines on the two nursing units with the highest number of PD admissions (neurology, general medicine). On these units, C/L can be administered by the nurse as soon as it is ordered, without waiting for the drug to be delivered from the central pharmacy. In early 2016, the decentralized hospital pharmacist began receiving a daily report of inpatients to whom levodopa has been prescribed, in order to reconcile inpatient and outpatient C/L orders and notify nursing staff if there are inconsistencies or concerns.
Measurement of outcomes
Data in the EMR regarding admissions and C/L administrations during admission were recorded from 1/1/2012 thru 12/31/2018. The 2012–2014 data provide a baseline prior to any interventions, which occurred in 2015–2016. 2017–2018 is regarded as the sustainability phase of the initiative.
The primary outcomes are the frequencies with which C/L products were administered within 60 minutes, 30 minutes and 15 minutes of the scheduled times. Variables are recorded continuously in an EMR-based dataset for each C/L administration, including: a unique patient code, a unique admission identifier, sex, admit and discharge dates, hospital unit, type of levodopa preparation used, scheduled date and time of levodopa administration, actual date and time of administration, minutes between scheduled and actual administration times, and mode of administration. “Mode of administration” is indicated by the nurse regarding each prescribed medication dose and includes options such as “given”, “missed”, and others. It was evident from early chart reviews that the both the nurses’ selection of terms other than “given”, and the reasons for using those terms, were quite varied, and it became a separate project to understand or change the frequency of C/L doses not given. In this project, we focused our attention and analysis on doses listed as either ‘given’ or ‘given during procedure’.
Statistical methods
The total number of admissions, unique patient admissions and C/L administrations during these admissions were reported by year. Patient sex (percent male), number of inpatient days, and length of stay were also recorded for each admission. Number of C/L administrations per admission and average number of minutes before or after scheduled administration time (reported as absolute value) were summarized.
Of the included C/L administrations, the percent of C/L doses that were administered within 15, 30, and 60 minutes of the scheduled time by year was calculated. To test the hypothesis that the probability of receiving PD medication on time increased or decreased over time, we utilized a two-sided Cochran-Armitage test, for each time interval of interest.
Finally, we assessed whether C/L administration rates within 15, 30, and 60 minutes of scheduled time varied by patient and/or administration characteristics such as sex, days since admittance, time of day, and day of week. This was completed using Chi-Square Tests for Independence on data from January 1, 2016–December 31, 2018.
All statistical analyses were conducted in SAS Version 9.4 at the 0.05 level of significance.
RESULTS
Figure 1 identifies the selection process for included C/L administrations (39,447 C/L administrations in the seven-year period). The first step was to remove those C/L administrations which were not given to patients with PD (4,464 administrations removed). Of the 34,983 remaining C/L administrations, 93.0% of doses were given to patients whose diagnosis was “Parkinson’s disease” and 7.0% to patients whose diagnosis was “Parkinsonism”. Diagnosis was determined by review of the EMR. For the remainder of this paper, “Parkinson’s disease” and “Parkinsonism” are grouped together as Parkinson’s disease (PD). We then excluded C/L administrations that were never given to the patient, including Missed Doses (5.8%) and Held Doses (2.2%). We then excluded C/L administrations (2.8%) in the Emergency Center, as the focus of this project was on patients admitted to the hospital. Finally, 14 administrations were removed as the scheduled and administered times differed by greater than 10 hours, suggesting the incorrect medication time was selected. After these administrations were excluded, 30,909 C/L administrations (78.4%) were included in the analysis.
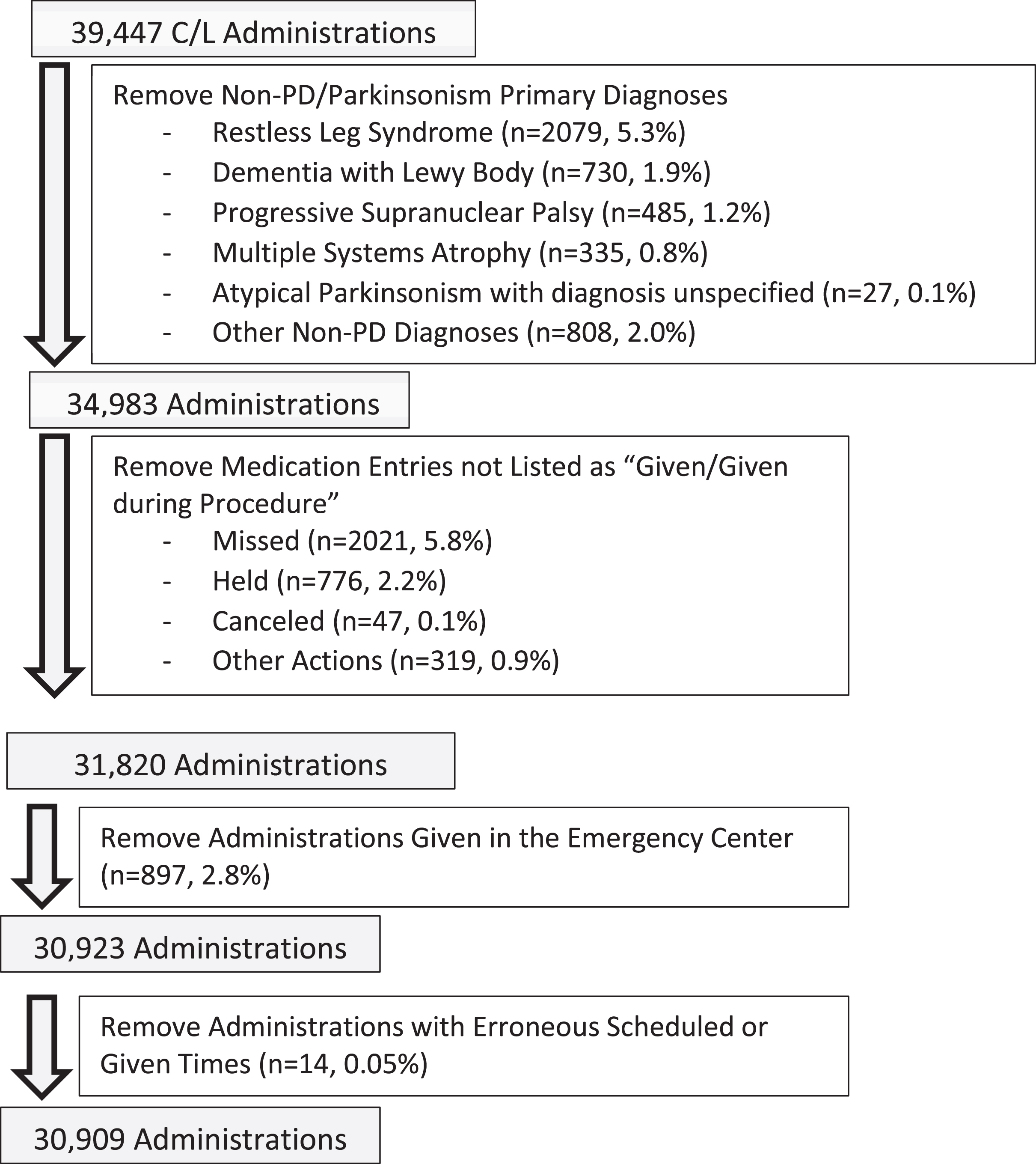
Selection of C/L Administrations from 1/1/2012 thru 12/31/2018.
From 1/1/2012 thru 12/31/2018, there were, on average, 4415.6 C/L administrations per year. From 2012–2018, there were, on average, 301 PD hospital admissions per year and 14.7C/L administrations per admission (Table 1). Of note, there were fewer unique patients than admissions, indicating that patients in our cohort, once admitted to the hospital, are likely to return.
Demographics of Admissions and C/L Administrations by Year of Discharge
‡absolute value.
Figure 2 shows the primary outcome, the percent of C/L doses given within 15, 30, and 60 minutes of the scheduled time. These rates were stable at about 43%, 66%, and 90%, respectively, in the years 2012–2014. In 2015, as interventions were implemented, there was a modest improvement, and beginning in the first half of 2016, a dramatic and sustained improvement in timely administration of C/L: 71% of doses within 15 minutes of the scheduled time, 86% within 30 minutes and 96.5% within 60 minutes by the end of 2018.
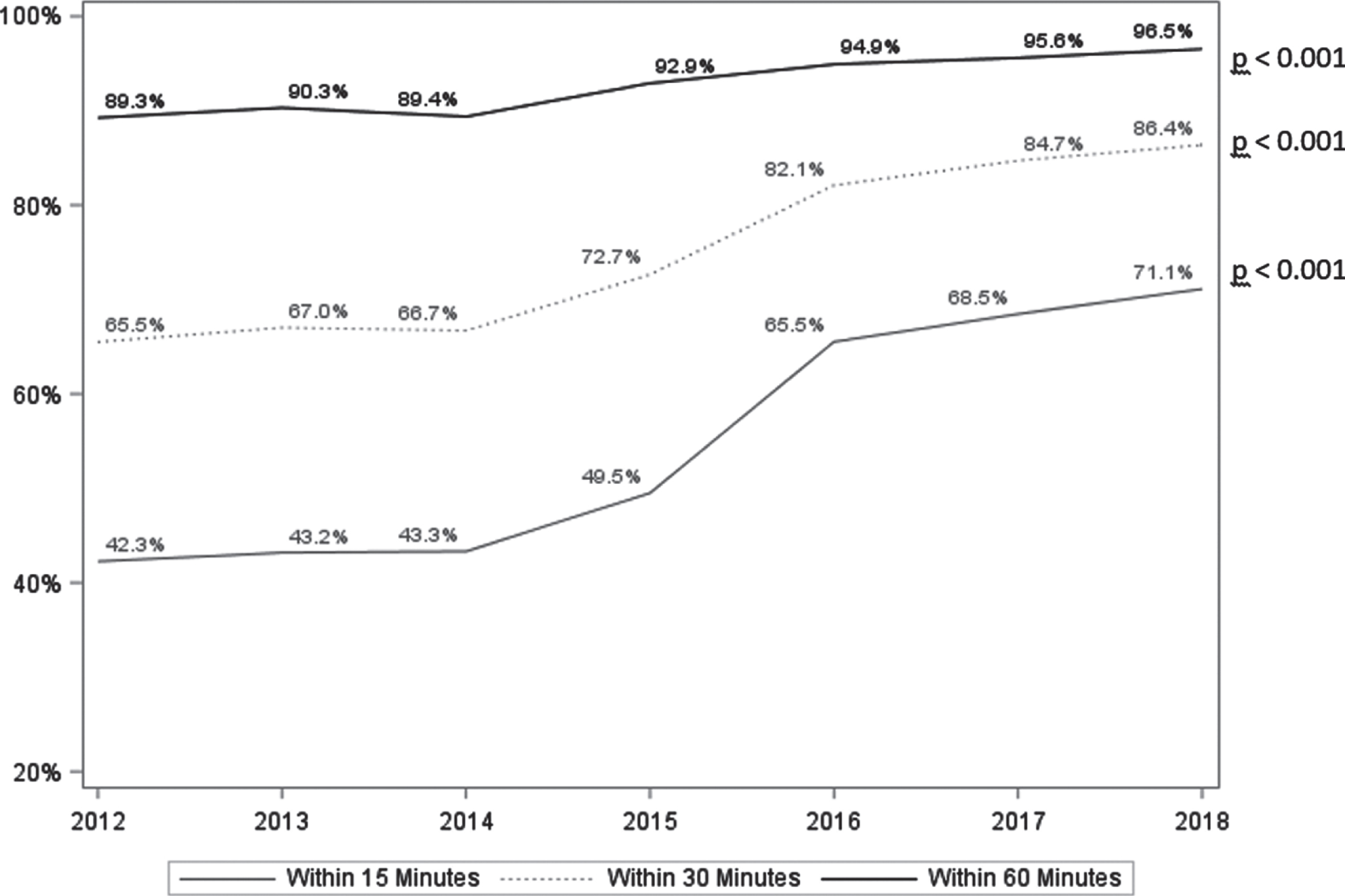
Percent of levodopa doses administered within 15, 30, and 60 minutes of the specified time (1/1/2012 thru 12/31/2018). Values calculated using Cochran-Armitage Trend Tests.
Timely administration of C/L significantly improved in almost all nursing units between 2012 and 2018, even though in-service training and on-unit stocking of immediate-release C/L only included the neurology and general medical units (data not shown).Timeliness of medication delivery within 15 minutes was significantly better for males (p < 0.001), after the first day of admission (p < 0.001), and during the hours of midnight to 6 : 00 am (Table 2).Timeliness was not impacted by day of the week.
C/L Administration rates within 60, 30 and 15 minutes by patient and administration characteristics for discharges from 1/1/2016 thru 12/31/2018 (N = 15,586 administrations)
‡P-values calculated using Chi-Square Tests for Independence.
DISCUSSION
The primary result of this initiative was a statistically significant improvement in timely administration of C/Lin a community hospital affiliated with a PF Center of Excellence, following the implementation of a series of educational, pharmacy, and nursing support interventions. In our hospital, C/L was consistently given within 60 minutes about 90% of the time at baseline, but with interventions, the rate of administration within 30 minutes went from about 65% to 86%, and administration within 15 minutes from 43% to 71%. By comparison, Martinez-Ramirez et al. [13] found that 61.5% of levodopa doses were administered within 60 minutes. On the PD specialty unit of Skelly et al. [22], 66% of PD medication doses (including C/L and other drugs) were administered within 30 minutes of the scheduled time, while Hou et al. reported that 83% of levodopa doses were given within that time frame [18]. Derry reported that 88% of scheduled doses were given, but that late dosing (not defined) occurred in 26% of admissions [17]. We believe that the standard should be delivery of C/L products within 15 minutes of the scheduled time, and that this is an achievable goal.
A number of studies over the last decade have identified medication use in hospitalized PD patients as an area that needs improvement. Aminoff et al. [6] described a number of “management considerations” related to medications; in a comment about this manuscript, Gerlach et al. [26] also singled out medication administration as a particularly important aspect of management. Strategies suggested by others to improve medication timeliness have included: education for nurses and hospital physicians, the establishment of a “Parkinson’s unit”, neurology specialist consultation, and patient self-administration of PD medications [22]. Recent reports describe a Disease-specific Certification program for PD [27], and a clinical process review to improve administration of C/L in the emergency department [28]. None of these studies report on the effects of the proposed strategies on the timeliness of medication administration.
This quality improvement initiative focused on improving timeliness of C/L administration, as we felt that this single change would have the greatest impact on the patient’s hospital experience, while keeping the processes simple and the message to hospital staff clear. Further, we were confident that addressing C/L administration would capture essentially all PD patients for whom medication timing is critical [29, 30]. The enduring interventions and processes include: EMR alerts for nursing along two different workflows, pharmacist review of levodopa orders at the time of admission, ongoing data collection and analysis through an EMR-based data report, and reports to nurse managers about the performance of their nursing unit. These automatic processes provide visual reminders to nurses and physicians regarding the importance of timely administration of Parkinson’s medications. Since implementing them, we have seen a sustained improvement in timeliness of C/L administration. There was no external funding for this project, but it was supported through internal support for quality improvement projects from hospital leadership, who in turn were particularly responsive to input from patients and families.
An important aspect of our program was the availability of an inpatient pharmacist to assist with inpatient/outpatient medication reconciliation (with 30 PD admissions/month, this has not been burdensome to the pharmacist). We were able to stock immediate-release C/L products on certain hospital units (neurology and general medicine), to reduce the waiting period between order placement and delivery of the drug to the patient care area. However, improvements in timely administration occurred on all nursing units, not just on units that now stock C/L products (data not shown). Finally, SPC physicians and nurses in the outpatient setting strive to write prescriptions that provide specific times for levodopa administration, which increases the likelihood that medications will be given at correct times in the hospital (e.g., 8 am, 12 pm, 5 pm, rather than “TID”, which may default to 8 am–2 pm–10 pm).
Critical to the program’s success was the development of systematic nursing alerts in the EMR. Addressing two different nursing workflows, medication administration and transition communication, strengthened systematic interventions. Inpatient nurses refer to the EMR and MAR frequently, and record information in it throughout their shift. The tactics serve as both a specific reminder for each patient on each nursing shift, and as a general educational tool for nurses on all units.
Ours can be viewed as an ideal situation, with an outpatient Parkinson’s disease center sharing an administrative and EMR system with our affiliated hospital. There are enough PD admissions and C/L administrations each year to justify the development of a process, and timely patient complaints provided impetus to the project. Potential barriers at other sites include lack of time, personnel, or priority in any of the involved departments, including the very first step, the development of an EMR-based report on C/L administration.
Limitations
This project was performed at a single institution with limited data collection about concomitant medications, diagnoses, and hospital course. While the majority of patients at our hospital have been seen by a movement disorders neurologist, not all of them have, and the diagnosis of PD was not verified by an in-hospital examination. As there was no control group for this quality improvement project, we cannot say with certainty that the improvement in timely administration of C/L was due to our interventions, and not to some other process or system change that we were unaware of. Further, we focused in this project on C/L doses that were actually given; understanding and reducing the number of ordered doses that are “not given” (9% of all ordered doses [Fig. 1]) is also important. While the percent of ordered doses that were “not given” declined over the course of the project (9.3% of doses in 2012, compared with 7.6% in 2018 (data not shown)), a fuller understanding of “not given” doses requires additional chart reviews and analyses that were not part of the project described here.
While non-timely administration of PD medications has been associated with longer hospital stays and more complications, we do not know from this initiative whether the converse is true—whether improvements in timely administration will lead to improvements in patient outcomes, such as length of stay and readmission rate, in-hospital complications such as falls, pneumonia, or transfer to a higher level of care. While we do not have objective data, our patients and families report less stress and anxiety during their hospitalizations at Park Nicollet Methodist Hospital, and report to us that the hospital staff understand their unique care needs. We believe that it is possible to aim for administration of C/L within 15 minutes of the scheduled time, which, given the sustained improvements seen here, does not appear to have been burdensome to staff. Additional work is needed to determine how/whether successful C/L administration (a process outcome) relates to successful admission (a patient outcome). Additional work is also needed to understand the observed relationship of timely C/L administration to patient sex, time of day, and day of hospital stay. Finally, many other special aspects of Parkinson’s disease care in the hospital—and in long-term care—deserve attention, including the potential for oral or tube feedings to interfere with levodopa absorption, the increased potential for orthostatic hypotension in relation to illness/immobility/dehydration, the increased risk of delirium, and the need to avoid the use of dopamine-blocking drugs, sedatives, and narcotics when possible.
In summary, we improved on-time administration of levodopa to hospitalized Parkinson’s patients through a quality improvement initiative that included staff education, and the enduring use of pharmacist interventions and EMR-based tools for nursing. The net result has been a cultural change, whereby physicians, nurses, and pharmacists throughout the hospital recognize the importance of timely administration of levodopa to the comfort and function of the hospitalized PD patient.
CONFLICT OF INTEREST
The Authors have no conflict of interest to report.
Footnotes
ACKNOWLEDGMENTS
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.