
Abstract
Isolated REM sleep behaviour disorder (iRBD) is a predictive marker of prodromal Lewy body disease. iRBD prevalence in the general population is around 1%, but it remains under-diagnosed, even though symptoms are alleviated by medication. We developed a population screening strategy and identified 16 iRBD patients by conducting telephone interviews and polysomnography examinations. We compared our population-screened cohort with sleep-center referred patients and found higher MoCA scores and lower MDS-UPDRS-III scores in our patients. In conclusion, screening can be used to identify iRBD patients in a cost-effective manner with the benefit of identifying patients at a very early disease stage.
INTRODUCTION
Isolated REM sleep behaviour disorder (iRBD), a parasomnia characterized by dream-enactment and loss of REM sleep atonia, is a very predictive marker for synucleinopathies, including Lewy body diseases (LBD) and multiple system atrophy [1, 2]. iRBD is found in 30% of newly diagnosed Parkinson’s disease (PD) patients and a recent study estimated the prevalence of RBD in the general population to be 1% [3]. iRBD remains markedly under-diagnosed even though it can sometimes be alleviated by medication and is debilitating and even dangerous for the patient and bed partner. Well characterized cohorts of iRBD patients may be crucial to successful development of disease modifying strategies in the future due to the high rate of conversion to LBD compared to other prodromal markers. The aim of this study was to recruit patients suffering from iRBD from the general population and compare these to sleep-center referred iRBD patients.
MATERIALS AND METHODS
Screening procedure
The protocol was approved by the ethical committee of the Central Region of Denmark. Subjects provided informed consent according to Declaration of Helsinki. Telephone consent was used in subjects not fulfilling the criteria (were screen-negative) and therefore evaluated by phone only. Written consent was used for all screen-positive patients, who came for evaluation in the clinic.
The screening procedure started with advertisements placed in local community newspapers totalling approximately 500.000 printed newspapers. We performed screening in two rounds, separated by six months. Advertisement text included Danish versions of five questions (2, 3, 5, 6.1, 6.3) from the iRBD symptoms questionnaire (RBDSQ) [4]. Subjects who were ≥50 years of age and answered “yes” to at least three questions were encouraged to contact the research group. The research associate (TDF, KK) contacted respondents and obtained consent before conducting the telephone interview. Respondents were initially explained that the research purpose involved the association between iRBD and PD, and that iRBD requires diagnostic confirmation by video-polysomnography (PSG). If the respondents felt uneasy about the prospect of receiving an iRBD diagnosis, they were advised to discontinue the interview. Respondents were interviewed about medical history, current medication intake, the complete RBDSQ and questions to exclude subjects who were less likely to have iRBD. Questions included 1) onset of symptoms before the age of 40 years, 2) current history of night walking or night terrors, 3) taking antidepressant or antipsychotic drugs consistent with possible pharmacologic-induced RBD, 4) posttraumatic stress disorder, 5) suspicion of sleep apnea due to high body mass index, daytime sleepiness, and snoring. All participants who scored ≥5 on the RBDSQ and did not answer “yes” to any extra questions were invited to a PSG to confirm the diagnosis of iRBD according to consensus criteria from the International Classification of Sleep Disorders III. If iRBD was diagnosed, the results of the evaluation and implications of diagnosis were discussed in full with the patient by the evaluating neurologists (MO, KBS); all patients were offered annual follow-up, symptomatic treatment was provided as clinically indicated.
Polysomnography
The SOMNOscreentrademark plus Tele + Video device was utilized for overnight video-PSG, as described [5]. Ten electroencephalogram and two electrooculogram electrodes, nasal pressure monitoring, electrocardiogram, thoracic and abdominal effort belts, electromyogram of the submental and tibialis anterior muscles, pulse oximetry, and video monitoring were used. Data were scored by board-certified experts in sleep medicine (MO, MS) according to AASM guidelines [6].
Other assessments
We compared symptoms of iRBD patients identified from the general population with four groups of sleep-center referred patients from the literature since we did not have available iRBD patients in the local sleep-clinic. Non-motor symptoms were quantified with the scales for outcomes in PD - autonomic (SCOPA-AUT) [7], and the non-motor symptoms questionnaire (NMSQuest) [8]. Gastrointestinal function was assessed using the ROME III diagnostic criteria [9]. Motor symptoms were scored with MDS Unified Parkinson’s disease Rating Scale part III (MDS-UPDRS III) [10]. Blood pressure was measured after 15 minutes of supine rest and after 1 minute of standing. Olfaction was assessed with 16-item Sniffin’ Sticks identification battery [11]. Cognition was evaluated with Montreal Cognitive Assessment battery (MoCA) [12].
Statistics
All data is presented as mean±SD. Unpaired t-test was performed for between-group comparisons.
RESULTS
The patient flow is illustrated in Fig. 1. In short, 100 potential patients contacted the researchers following advertisements. Upon telephone interview, 31 did not wish to participate, 28 subjects due to the scope of the study, and three subjects due to unwillingness to receive knowledge of possible increased PD risk. Remaining subjects completed the phone screening interview as described above. A sleep expert (MO) evaluated the answers and 49% of subjects were eligible for examination with PSG. After having the procedure explained 10 of the 34 refused further participation. Thus, 24 PSG examinations were completed. In 16 subjects (67%) iRBD was confirmed according to the ICD-3 criteria. Five subjects suffered from severe sleep apnea disturbing REM sleep in a way that potential RBD could not be assessed and three subjects had normal PSG examinations.
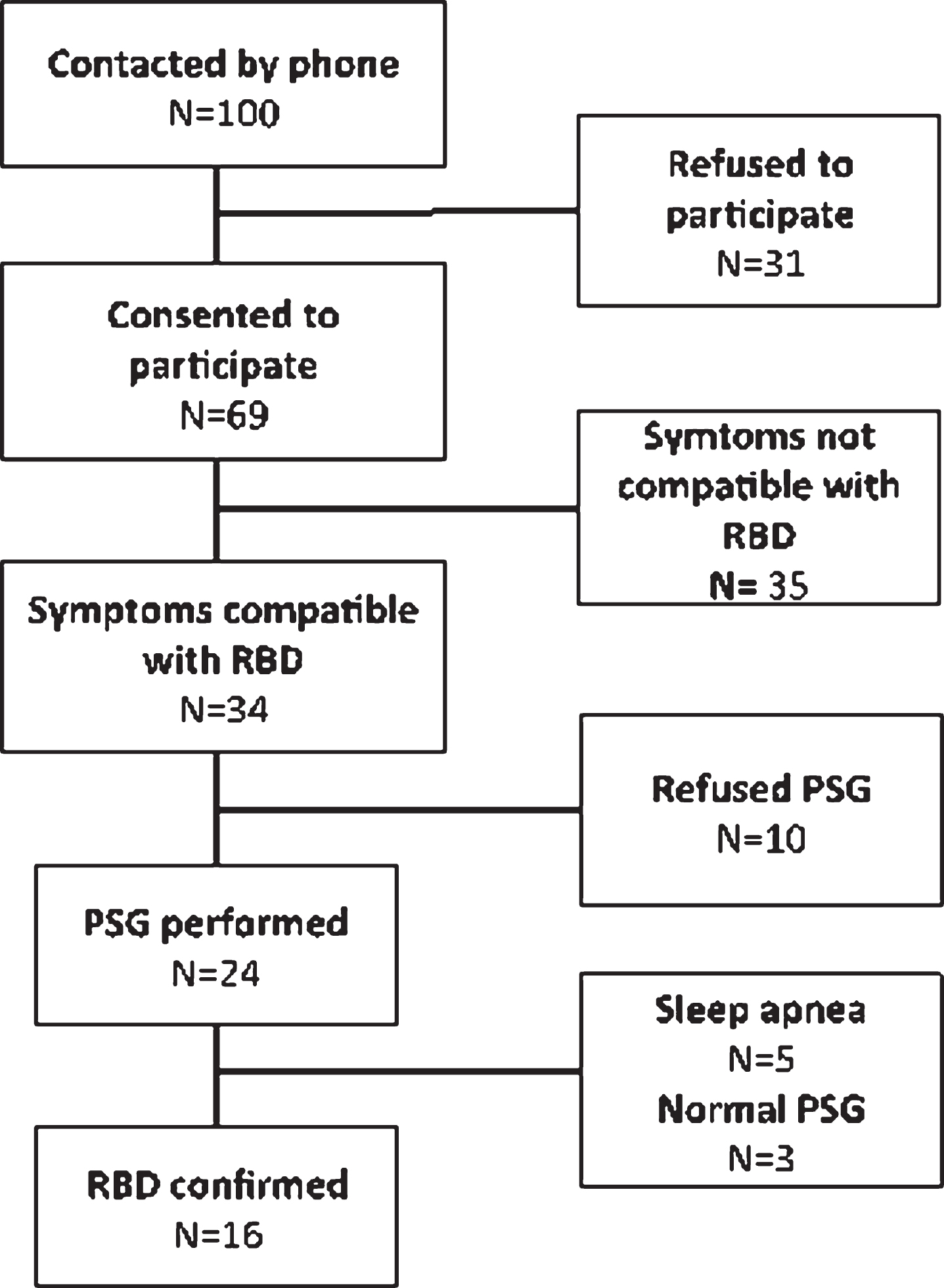
Patient flow.
Symptom severity in sleep-center referred iRBD patients and population-screened iRBD patients is compared in Table 1. There was no significant difference between the population-screened iRBD cohort and the cohort from Ferini-Strambi et al. [13]. When comparing our iRBD cohort with the cohort from Barber et al. [14], we found a better performance in MoCA (p = 0.03) and UPDRS (p = 0.03) in our iRBD patients. However, population-screened RBD patients were older (p = 0.02) and had more severe hyposmia (p < 0.01). When comparing our iRBD cohort with the cohort from Aguirre-Mardones et al. [15], we also found a higher MoCA score in our cohort (p = 0.01) as well as more severe hyposmia (p < 0.01). Furthermore, population-based iRBD patients had less severe daytime sleepiness (p < 0.01). In comparison to Postuma et al. [16], our population-based iRBD cohort had lower MDS-UPDRS III scores (p < 0.01) and higher MoCA scores (p = 0.02) when comparing to their sleep-center recruited patients, and lower MDS-UPDRS III scores (p = 0.04) in comparison to their population-screened patients.
Clinical and demographic characteristics of patients and controls
*Here, we used the method from Lawton et al.[19] to convert UPSIT results to a Sniffin Sticks’ equivalent.
DISCUSSION
Newspaper-based screening and PSG is a feasible method to identify patients with iRBD in a Western population. We identified 16 iRBD patients by conducting 100 phone interviews of 10–60 min duration. A single set of ambulatory PSG equipment was used for all examinations, reducing the cost of the study. The frequency of confirmatory PSG examinations was >60%, providing good cost-effectiveness. Furthermore, five patients who suffered from sleep apnea were excluded, but these might still have iRBD, so the proportion of iRBD may have been underestimated. A similar study performed by Postuma et al. [16] reported very similar frequency of positive PSGs, and a short commentary by Buškov
There is increasing interest in investigating cohorts of iRBD patients for research purposes, because iRBD is highly predictive of developing manifest LBD later in life. However, there are several ethical concerns regarding screening for iRBD. LBD is incurable and some will be reluctant to receive an iRBD diagnosis, since there are no treatments to prevent conversion to LBD. We paid close attention to initially informing respondents about the association between iRBD and LBD. Only 3% of participants refused further participation on this ground.
Our study suggests that iRBD patients identified by population screening may generally be in an earlier disease stage compared to patients followed in a sleep clinic. We compared our small cohort to published data from several iRBD cohorts followed in sleep clinics around the world. The present iRBD patients displayed lower motor score and less cognitive decline. Our iRBD cohort was older and had more severe hyposmia compared to at least one other cohort. We did not find any difference in autonomic symptoms between population-screened iRBD patients and sleep-center patients, but our patients had fewer complaints from daytime sleepiness.
Some limitations from this study need to be addressed. We did not have a large in-house cohort of sleep-center diagnosed iRBD patients as comparison and were forced to use several cohorts from the literature, none of which had a complete dataset to match ours. Furthermore, 16 RBD patients may have been too few to detect other differences between cohorts.
A multistep screening can be used to identify iRBD patients in the general population with the possible benefit of identifying prodromal PD patients at a very early disease stage.
CONFLICTS OF INTEREST
The authors declare that there is no conflict of interest regarding the publication of this paper.
Footnotes
ACKNOWLEDGMENTS
The research and publication of this article is funded by a grant from the Lundbeck Foundation [2014-4183].