
Abstract
Abstract. Background:
Parkinson’s disease (PD) negatively affects patients’ Quality of Life (QoL) which depends on both objective criteria such as physical health and subjective ones such as worries and norms according to personal believes. Therefore, QoL could be also associated to personality dimensions in chronic neurological diseases such as PD.
Objective:
Our objective was thus to study the potential association between personality dimensions and QoL in PD patients with motor fluctuations before Deep Brain Stimulation of the Sub-Thalamic Nucleus (DBS-STN).
Methods:
Data were obtained from the French multicentric cohort study Predi-Stim. All PD patients awaiting DBS-STN and responding to the inclusion criteria at the time of the study were included. All participants answered the “Temperament and Character Inventory” (TCI) and the PDQ-39 before surgery. Analyses were made using adjusted univariate generalized linear regression models to evaluate a potential association between TCI dimensions and PDQ-39 scores.
Results:
Three hundred thirty-three consecutive patients were included. The temperament Harm Avoidance was negatively associated with QoL (p = 1e-4, R2= 0.33), whereas the character Self-Directedness was positively associated with mental component of QoL (p = 2e-4, R2= 0.33) in PD patients with motor fluctuations awaiting DBS-STN.
Conclusions:
PD patients with motor fluctuations, with lower Harm Avoidance and higher Self-Directedness scores have the best QoL mainly at an emotional and social level. Therapeutic education of these PD patients focusing on their personal resources may thus be important to improve their well-being.
INTRODUCTION
Besides motor symptoms, several non-motor symptoms affect PD patients such as sleepiness, anxiety, depression and pain [1]. All these symptoms impair Quality of Life (QoL) in Parkinson’s disease (PD) population [2].
It is known that different factors may affect QoL in general and diseased populations, since it depends on both objective criteria such as patients’ physical health or psychological state as well as subjective perceptual factors such as expectations, norms and worries according to personal believes [3]. Therefore, personality, which is defined as a system determining individuals behavior, characteristics and thoughts, seems to be a factor associated with QoL [4]. Indeed, several studies have shown a relationship between QoL and personality in different diseases such as schizophrenia [5], epilepsy [6] and anxio-depressive syndromes [7]. Thus, personality could probably influence QoL in PD.
Indeed, in a study using the Big Five personality traits model (NEO PI-R), a negative correlation between PD patients QoL (assessed by the Parkinson’s Disease Quality of Life Questionnaire (PDQL)) and “neuroticism” (behavior of exacerbated anxiety assessed by the Neuroticism–Extraversion–Openness Five-factor Inventory (NEO-FFI)), and a positive correlation with “conscientiousness” (behavior of implication/commitment in its work from the NEO-FFI) were shown [8].
Nevertheless, the use of this questionnaire in PD is unusual (only 2 studies from 17 in a recent meta-analysis of PD and personality [9]) whereas the “Temperament and Character Inventory” (TCI) is one of the most widely used tool to evaluate personality within PD population (7 studies in the meta-analysis [9]). The TCI is a self-questionnaire developed by Cloninger to evaluate individual’s personality traits according to seven dimensions: Novelty Seeking (NS), Harm Avoidance (HA), Reward Dependence (RD), Persistence (P), Self-Directedness (SD), Cooperativeness (C) and Self-Transcendence (ST) [10], themselves subdivided into sub-dimensions (see the Methods section). It was validated in several studies through its stability and methodological qualities [4, 11–13]. Based on psychobiology, the particularity of Cloninger concept is that personality is dependent on two main traits: the temperaments and the characters. Temperaments (NS, HA, RD and P) are relatively stable personality dimensions related to genetics and neurotransmitters; whereas characters (SD, C and ST) are developmental personality dimensions formed according to personal life and experiences which could vary over time [4].
To our knowledge, TCI personality dimensions as explanatory factor of QoL have never been evaluated in PD. Only one preliminary study was conducted by our team in 30 PD patients and allowed the identification of three personality dimensions (HA, P and SD) associated with QoL [14]. Both high P and SD scores were correlated with a higher QoL, whereas high HA scores were correlated with a lower QoL in PD patients.
The aim of this study was to investigate the impact of personality dimensions (through the TCI) on QoL (evaluated by the Parkinson Disease Questionnaire 39 (PDQ-39)) in a large cohort of PD patients with motor fluctuations expecting Deep Brain Stimulation of the Sub-Thalamic Nucleus (DBS-STN). The purpose of this first paper would be to guarantee the adequacy of using a personality questionnaire in predicting QoL of PD patients, leading to a second paper about how personality traits can significantly predict QoL after DBS-STN.
MATERIALS AND METHODS
This is an ancillary study of a multicentric prospective study PREDI-STIM whose objective is to identify predictive factors of QoL response after Deep Brain Stimulation of the Sub-Thalamic Nucleus (DBS-STN) in PD patients (clinicalTrial.gov n°NCT02360683). The purpose of our study is to evaluate the association between some personality dimensions and PDQ-39 QoL in PD patients with motor fluctuations before DBS-STN.
Patients
The study population consisted of PD patients who participated to the PREDI-STIM study and were waiting for surgery of DBS-STN.
Patients were selected for DBS-STN with the standard surgical selection criteria (CAPSIT-PD - Core Assessment Program for Surgical Interventional Therapies in Parkinson’s Disease [15]): PD, moderate or severe L-Dopa related motor complications despite adjustment of dopaminergic treatment and absence of contraindications (dementia or cognitive deficit (MoCA score <24), age >75 years old, psychosis, dopa-sensibility <30%). Each patient underwent a psychiatric evaluation by a psychiatrist to ensure that he had no significant psychiatric symptoms.
All patients gave their informed consent and PREDI-STIM study was approved by ethic committee (CPP Nord-Ouest IV).
Study design and clinical measures
All the patients participated in investigations of the PREDI-STIM study. Briefly, motor state was evaluated by MDS-UPDRS in OFF and ON conditions before DBS-STN. Behavioral, clinical, genetic assessments and medical imaging were also carried out (clinicalTrial.gov n°NCT02360683).
As part of our ancillary study, only the TCI was added before surgery of DBS-STN.
The Temperament and Character Inventory (TCI) was used to access PD patients’ personality through seven dimensions. This self-questionnaire is divided into four genetically determined temperaments, according to Cloninger’s model: Novelty Seeking (NS), Harm Avoidance (HA), Reward Dependence (RD) and Persistence (P). This questionnaire is also formed by three characters which are developed through growing: Self-Directedness (SD); Cooperativeness (C) and Self-Transcendence (ST). Except for P dimension, each dimension is divided into sub-dimensions: NS and HA are formed by 4 sub-dimensions, RD and ST by 3, and SD and C by 5. The TCI is formed by 226 items with binary responses (true/false) allowing to obtain an independent score for each of the seven personality dimensions. Each dimension represents a part of individual personality ranging on a spectrum. Higher is the score, higher the patient presents the associated personality dimension. NS scores range from reserved and organized individuals to more impulsive and curious persons; HA scores from optimist and courageous people to anxious and pessimist ones; RD scores from independent and insensitive individuals to socially attached and sensitive ones; and P scores from underperforming and without ambition people to hardworking and perseverant ones. Concerning characters, they represent levels of different maturity: SD is associated with individual maturity (ranging from irresponsible profiles to determinate and responsible ones); C is associated with social maturity (from intolerant profiles to empathetic and good teamwork skills); and ST is associated with spiritual maturity (from proud and materialist persons to believing and humble individuals).
Patients’ Quality of Life (QoL) was evaluated through the Parkinson’s Disease Questionnaire 39 (PDQ-39). This questionnaire is specific to PD and divided into eight sub-scales of QoL with a Mental Component Score (“Emotional Well-Being”, “Stigma”, “Social Support”, “Cognitions” and “Communication”) and a physical component score (“Mobility”, “Activities of Daily Living” (ADL) and “Bodily Discomfort”). The higher score indicates the worst QoL. The eight sub-scales altogether also forming a total PDQ-39 score.
The total Levodopa Equivalent Dose (LED) was calculated for each patient according to levodopa treatments, dopaminergic agonists, inhibitors of dopamine catabolism (COMT and MAO inhibitors) and other antiparkinsonians such as amantadine [16], to be used as adjustment variable.
In order to evaluate some behavioral aspects, patients’ apathy was measured through the Lille Apathy Rating Scale (LARS) and depression was evaluated by the Hamilton Depression Rating Scale (HDRS/HAMD).
Data analysis
Data missing
Because of the expected data missing and because none imputation method of TCI missing data was yet validated, we have determined one with an expert committee consisting of neurologists, biostatisticians and psychiatrists.
Patients with more than 20% of non-responses (NR) in the whole TCI, were eliminated from the study. As for patients with less than 20% of NR in the whole TCI, we have treated differently the NR depending to the proportions of NR by dimensions.
For patients with less than 20% of NR by TCI dimension, we corrected NR by each patient tendency (the tendency being the way in which the majority of a patient’s responses goes in a unique dimension). For example, NR of a patient having a tendency of impulsivity in the NS dimension, were replaced accordingly to this impulsivity profile.
For patients with 20% or more NR by TCI dimension, we corrected NR by mean score: their dimension’s scores were substituted by the mean score of all patients in this dimension (mean was calculated according to sex only for HA and RD dimensions since their score is influenced by sex [17]).
Statistical analyses
Descriptive analyses were made: mean, standard deviation and range (min, max) for quantitative variables; effective and percentage for qualitative variables.
In order to evaluate the association between TCI dimensions and PDQ-39 scores, we used generalized linear regression models (GLM) respecting normality of data. Univariate GLM, rather than multivariate GLM, were chosen in order to evaluate separately if each personality dimension, and not global personality, is associated with QoL. The response variables corresponded to each QoL score. We calculated the score in percentage of each TCI personality dimensions, depending on the maximum dimension score, to use as explanatory variables for comparison of each TCI dimensions association with QoL. Two supplementary explanatory variables were also added in the regression models (in more of the TCI dimensions) to evaluate the impact of behavioral aspects on QoL: the HAMD and the LARS total scores. Models were adjusted with sex, age, disease duration and LED (cognition as seen by the MoCA was not used as adjustment because MoCA scores <24 were used as exclusion criteria), and quality of each model was assessed. Similar univariate generalized linear models were built with the sub-dimensions of each significant TCI dimension. The score in percentage of each sub-dimension was used as explanatory variables. For the dimensions level analyses, significance threshold corrected by Bonferroni method of p < 0.007 was used (7 models for each response variable) and p < 0.0016 for the sub-dimensions level (31 models), and analyses were proceeded on R Studio Software Version 1.1.456.
RESULTS
Among the 489 patients having completed the TCI, 156 patients were excluded (>20% of NR in the whole questionnaire (n = 12), and missing data in the other variables (n = 144)). Finally, of the 333 remaining patients, 237 had none NR in their whole TCI; 96 had less than 20% of NR per TCI dimensions which were corrected by tendency; and from them, 2 patients also had 20% or more of NRs by dimension which were replaced with the mean score of patients’ responders in these dimensions (Fig. 1). From these 96 PD patients with missing TCI responses, 76% of them had less than 4 missing responses in the whole TCI (226 questions) (51 patients (53%) having only one missing responses) and only 8 patients (8%) had more than 10.
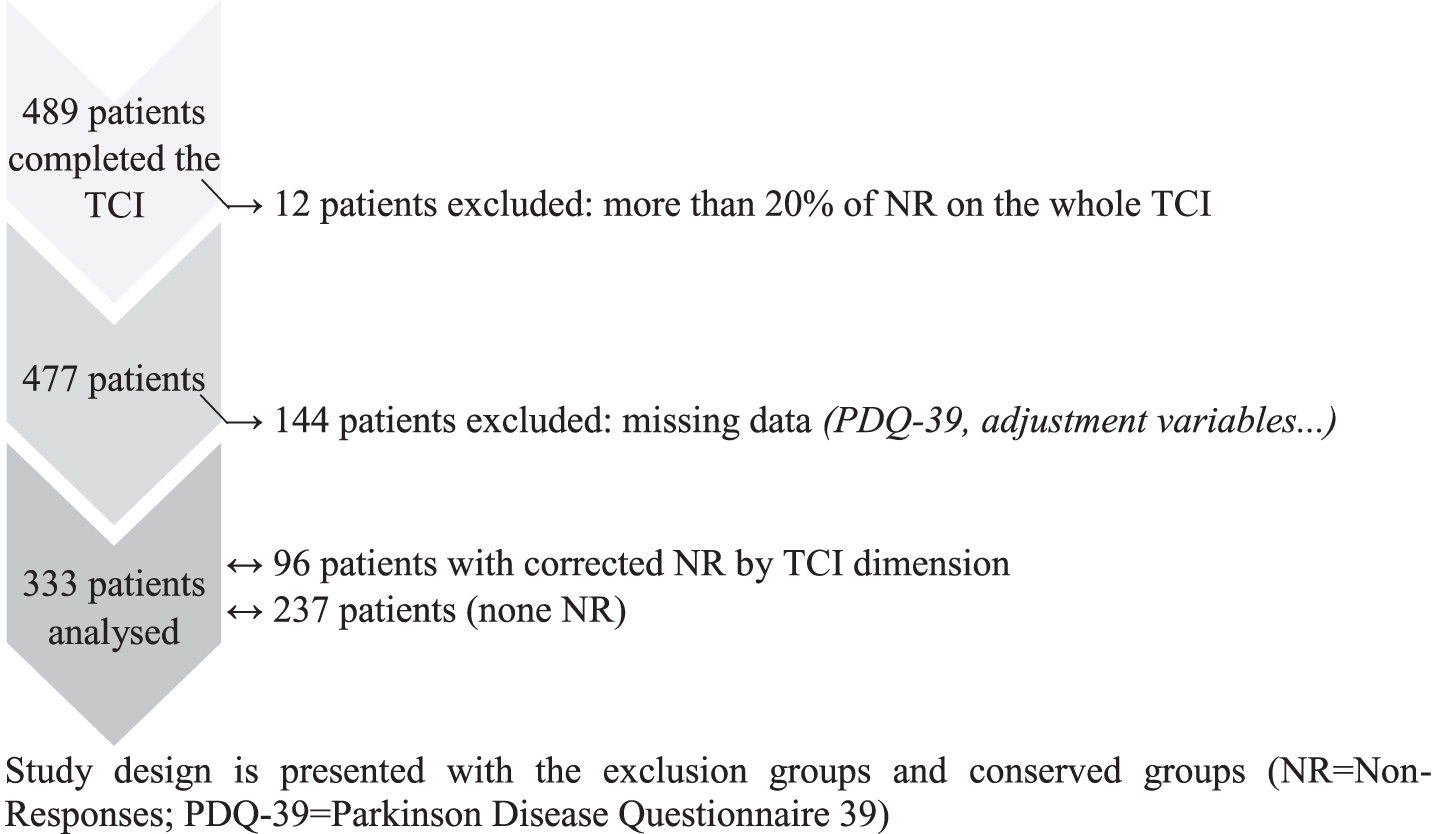
Flow chart of PD patients.
A total of 333 PD patients (113 women (33.9%) and 220 men (66.1%))—with average age of 61.1±7.3 years old and PD average duration of 10.2±4.1 years—were analyzed in this study (Table 1). All patients were treated by antiparkinsonian treatments: levodopa (n = 217), dopaminergic agonists (n = 171), MAO (n = 89) or COMT inhibitors (n = 11), and anticholinergics (n = 9). Mean LED was of 1181.6±789.4 mg/day. PD patients had a good response to dopaminergic treatments as seen by the MDS-UPDRS III ON and OFF scores, and no cognitive decline (mean MoCA score of 26.6±2.3). Regarding QoL, the total score of PDQ-39 was of 32% with higher scores in “Bodily discomfort”, “Activities of daily living” and “Mobility” (Table 1). Concerning personality dimensions, our patients had the highest score in P (5.4±1.7, max = 8), SD (34.2±6.1, max = 44) and C (33.6±4.5, max = 42) dimensions (Table 1).
Baseline demographics and PD characteristics (n = 333)
SD, standard deviation; LED, Levodopa equivalent dosage; *MoCA>24, absence of cognitive deficit; **HAMD<20, none-depressive state; ***LARS< -26, none-apathetic state.
Table 2 shows TCI dimensions with a significant linear association on PDQ-39 scores at a corrected significant threshold (p-value corrected < 0.007).
Adjusted linear regression models of association between TCI dimensions scores (in %) and PDQ-39 sub-scales scores
HA, Harm Avoidance; SD, Self-Directedness; C, Cooperativeness; ST, Self-Transcendence; R2, adjusted R-squared; *statistically significant p-value after Bonferroni correction for 7 comparisons, p-value <0.007.
HA, SD and ST dimension scores were significantly associated with PDQ-39 Total score: association was positive for the HA temperament and the ST character, while negative for the SD character.
Considering the different sub-scales of QoL, HA and ST dimensions were significantly positively associated with part of the Mental Component Score (MCS) (“Emotional well-being”, “Stigma” and “Communication” sub-scales) for HA and with only two items of the MCS (“Emotional well-being” and “Communication”) for ST (higher HA and ST scores resulting in worse QoL).
SD dimension was significantly negatively associated with most of the MCS: “Emotional well-being”, “Social support”, “Cognition” and “Communication” (higher scores resulting in best QoL).
C dimension was only negatively significantly associated with PDQ-39 “Cognitions” scores (higher C scores resulting in best QoL).
TCI sub-dimensions presenting a significant linear association with PDQ-39 scores at a corrected significant threshold (p-value corrected <0.0016) are shown in Table 3.
Adjusted linear regression models of association between TCI sub-dimensions scores (in %) and PDQ-39 sub-scales scores
HA, Harm Avoidance; SD, Self-Directedness; C, Cooperativeness; ST, Self-Transcendence; R2, adjusted R-squared; *statistically significant p-value after Bonferroni correction for 31 comparisons, p-value <0.0016.
Most HA sub-dimensions (HA1, HA2 and HA3) were positively significantly associated with Total PDQ-39 score and most sub-scales of the MCS.
All SD sub-dimensions (SD1, SD2, SD3, SD4 and SD5) were negatively significantly associated with either Total PDQ-39 score or some MCS.
Only ST2 sub-dimension was positively significantly associated with Total PDQ-39 and “Communication” scores.
Only C1 sub-dimension was negatively significantly associated with “Cognitions” scores.
Finally, concerning the behavioral variables, a positive and significant association was observed between the HAMD and all of PDQ-39 scores (Total and sub-scores) (p-value corrected <0.007); whereas no significant association was found between the LARS and any PDQ-39 scores.
DISCUSSION
In this study, we could demonstrate a significant association between personality dimensions and QoL in PD patients with motor fluctuations before DBS-STN. Specifically, higher HA scores are significant independent predictor of poor QoL, whereas higher SD scores are significant independent predictors of good QoL. Moreover, the only QoL sub-scales associated with personality dimensions are MCS. We could also confirm the significant association between depression and QoL in these PD patients with motor fluctuations.
Considering our PD population, as expected, the most affected sub-scales of PDQ-39 concern the physical component: “Mobility”, “Activities of daily living” and “Bodily discomfort” [18]. Our PD patients have also high values in the P temperament and in the SD and C characters preoperatively, suggesting their perseverance, adaptability, self-control and social maturity. These personality aspects may correspond to a profile of patients waiting for DBS because it is an invasive surgical intervention that some patients refuse.
Concerning the relationship between QoL and personality, four out of the seven TCI personality dimensions (HA, SD, C and ST) can significantly explain between 9% and 35% of the QoL variance of PD patients fitted for depression. In fact, considering the Beta coefficient of linear regression, the p-value and the R-squared values, two of these personality dimensions (HA and SD) seem to have a major association with PDQ-39 scores. These two TCI dimensions are differently associated with QoL. The HA temperament is negatively associated with QoL, whereas the SD character is positively associated with QoL of PD patients. PD patients with lower scores at HA dimension and higher scores at SD dimension have the best QoL at baseline.
On the one hand, HA dimension, through its link with serotonin [19], has been correlated to depression [20] which has been evaluated as the most determinant factor of QoL in PD patients [2, 21–24]. Higher HA scores have also been associated with a worst QoL in several diseases such as schizophrenia [5] and anxio-depressive syndromes [7]. In PD, higher score of neuroticism (a personality trait close to HA) was correlated with a low QoL [8]. In addition, our previous study has found a negative association between HA and PDQ-39 [14]. HA profile is viewed as an inhibition behavior with worry and pessimism in anticipation of future events [25]. Thus, PD patients with this personality profile would have a low QoL.
On the other hand, higher SD scores are associated with better personal resources. This character may have been developed because of the chronic disease in order to adjust to a new environment and to better manage themselves. It is thus not surprising that SD dimension has already been positively correlated with QoL in different population [6, 27]. In epileptic inpatients, SD was also positively correlated with the MSPSS scale (Multidimensional Scale of Perceived Social Support Scale which measures the perceived social support from family, friends and special persons) [6]. In PD patients, we have also already shown a positive association of SD with PDQ-39 [14], corroborating our actual results.
Even if these two TCI dimensions (HA and SD) are associated with global QoL (PDQ-39 total score), this association seems mainly due to an association with the emotional or psychological and social part of QoL, rather than with the physical parts of the QoL more directly related to PD. Indeed, the PDQ-39 “Emotional well-being”, “Stigma”, “Social support”, “Cognitions” and “Communication” scores (MCS) are the only associated sub-scales with HA and SD dimensions, according to the linear models; whereas the PDQ-39 sub-scales “Mobility”, “Activities of Daily Living” and “Bodily Discomfort” are not associated with personality dimensions. This suggests that TCI dimensions are mainly associated with the emotional complaints of PD patients and not with the physical component of the PDQ-39.
Regarding the TCI sub-dimensions, most of all the HA and SD sub-dimensions explained around 10 or 34% of the different PDQ-39 sub-scales variance. Therefore, we can hypothesize that during the course of PD, patients tend to become more focus on themselves and thus develop higher personal resources (higher SD) in order to handle at best with their disease and have a better QoL. In this idea, a study on a PD educational program has shown that engaging in self-management promotes life well-being [28]. Self-monitoring is a technique to initiate behavior to better deal with physical and emotional symptoms [28]. By contrast, higher HA scores reflecting an inhibition and worry behavior may stand in the way of progress of these PD patients to deal with their disease and thus lead to a worse QoL.
Finally, depression (evaluated by the HAMD) was always positively and significantly associated with PDQ-39 Total score and all of its sub-scores: the most depressed patients had the worst QoL. This confirms previous studies which have found that depression was one of the main factors influencing QoL in PD patients [2, 21–24] and that this association is also present in a PD population with motor fluctuations awaiting DBS-STN. It also shows that depression is an important factor to take into account when studying QoL because it affects as much physical as mental component of QoL, as opposed to personality dimensions which affect only mental component of QoL. By contrast, apathy was not significantly associated with any sub-scores of QoL.
Our study has strengths and limitations. The main strength is the large cohort of PD patients with motor fluctuations (one of the biggest published). The main limitation is the low adjusted R-squared values indicating that personality is not the sole parameter associated with QoL and that there are probably other explanatory factors of QoL. Indeed, in our regression models, we have tested several adjustment variables and have found three demographical factors that seem associated with QoL. Sex and age of PD patients are associated with QoL mainly with the physical component, whereas disease duration is associated with Total QoL. Thus, men seem to have a better QoL than women, disease duration worsens QoL, and oldest PD patients have a better QoL. This could be explained by the hypothesis that younger PD patients have higher expectations and are thus rating their QoL more severely.
In conclusion, in PD patients with motor fluctuations, the HA temperament and the SD character are associated with QoL, mainly at an emotional and social level. Then, PD patients with lower HA and higher SD scores have the best QoL.
This might lead to propose therapeutic education to these PD patients focusing on their personal resources to improve their well-being, assuming that this personality dimension (SD character) can be developed. Moreover, our aim of guaranteeing the adequacy of using a personality questionnaire in predicting QoL of PD patients being achieved, thus some personality dimensions could be predictive factors for a better QoL after DBS-STN. In fact, despite a good result on their motor status, some patients are still unsatisfied after DBS-STN [29, 30]. The assessment of the influence of personality dimensions on QoL improvement after DBS-STN will be examined further in a following study.
Members of the PREDI-STIM study group*
Dr Caroline Moreau, Pr Luc Defebvre, Dr Nicolas Carriere, Dr Guillaume Grolez, Dr Guillaume Baille, Dr Kreisler, Pr Jean-Pierre Pruvo, Pr Leclerc, Dr Renaud Lopes, Dr Romain Viard, Dr Gregory Kuchcinski, Mr Julien Dumont, Pr Kathy Dujardin, Mme M Delliaux, Mrs M Brion, Dr Gustavo Touzet, Pr Nicolas Reyns, Pr Arnaud Delval, Mrs Valerie Santraine, Mrs Marie Pleuvret, Mr Victor Laugeais, Thavarak Ouk, Camille Potey, Celine Leclercq and Elise Gers (for Lille University Hospital); Jean-Christophe Corvol, Marie-Vidailhet, Elodie Hainque, Marie-Laure Welter, Lucette Lacomblez, David Grabli, Emmanuel Roze, Yulia Worbe, Cécile Delorme, Hana You, Jonas Ihle, Raquel Guimeraes-Costa, Florence Cormier-Dequaire, Aurélie Méneret, Andréas Hartmann, Louise-Laure Mariani, Stéphane Lehericy, Virginie Czernecki, Fanny Pineau, Frédérique Bozon, Camille Huiban, Eve Benchetrit, Carine Karachi, Soledad Navarro, Philippe Cornu, Arlette Welaratne, Carole Dongmo-Kenfack, Lise Mantisi, Nathalie Jarry, Sophie Aix and Carine Lefort (for the AP-HP of Paris); Dr Tiphaine Rouaud, Pr Philippe Damier, Pr Pascal Derkinderen, Dr Anne-Gaelle Corbille, Dr Elisabeth Calvier-Auffray, Mrs Laetitia Rocher, Mrs Anne-Laure Deruet, Dr Raoul Sylvie, Dr Roualdes Vincent and Mrs Le Dily Séverine (for Nantes University Hospital); Dr Ana Marques, Dr Berangere Debilly, Pr Franck Durif, Dr Philippe Derost, Dr Charlotte Beal, Carine Chassain, Laure Delaby, Tiphaine Vidal, Pr Jean Jacques Lemaire, Isabelle Rieu and Elodie Durand (for Clermont-Ferrand University Hospital); Pr Alexandre Eusebio, Pr Jean-Philippe Azulay, Dr Tatiana Witjas, Dr Frédérique Fluchère, Dr Stephan Grimaldi, Pr Nadine Girard, Eve Benchetrit, Marie Delfini, Dr Romain Carron, Pr Jean Regis, Dr Giorgio Spatola and Camille Magnaudet (for the AP-HM of Marseille); Dr Ansquer Solène, Dr Benatru Isabelle, Dr Colin Olivier, Pr Houeto JL, Pr Guillevin Remy, Mrs Fradet Anne, Mrs Anziza Manssouri, Dr Cam Philippe, Dr Page Philippe, Pr Bataille Benoit, Mrs Rabois Emilie and Mrs Guillemain Annie (for Poitiers University Hospital); Dr Drapier Sophie, Dr Frédérique Leh, Dr Alexandre Bonnet, Pr Marc Vérin, Dr Jean-Christophe Ferré, Mr Jean François Houvenaghel, Pr Claire Haegelen, Mrs Francoise Kestens and Mrs Solenn Ory (for Rennes University Hospital); Pr Pierre Burbaud, Dr Nathalie Damon-Perriere, Pr Wassilios Meissner, Pr Francois Tison, Dr Stéphanie Bannier, Dr Elsa Krim, Pr Dominique Guehl, Sandrine Molinier-Blossier, Morgan Ollivier, Marion Lacoste, Nicolas Auzou, Marie Bonnet, Pr Emmanuel Cuny, Dr Julien Engelhardt, Olivier Branchard, Clotilde Huet and Julie Blanchard (for Bordeaux University Hospital); Pr Rascol Olivier, Dr Christine Brefel Courbon, Dr Fabienne Ory Magne, Dr Marion Simonetta Moreau, Pr Christophe Arbus, Pr Fabrice Bonneville, Dr Jean Albert Lotterie, Marion Sarrail, Pr Patrick Chaynes, Pr François Caire and Estelle Harroch (for Toulouse University Hospital); Pr David Maltete, Dr Romain Lefaucheur, Dr Damien Fetter, Dr Nicolas Magne, Mrs Sandrine Bioux, Mrs Maud Loubeyre, Mrs Evangéline Bliaux, Mrs Dorothée Pouliquen, Pr Stéphane Derrey, Mrs Linda Vernon and Dr Frédéric Ziegler (for Rouen University Hospital); Mathieu Anheim, Ouhaid Lagha-Boukbiza, Christine Tranchant, Odile Gebus, Solveig Montaut, S Kremer, Nadine Longato, Clélie Phillips, Jimmy Voirin, Marie des Neiges Santin and Dominique Chaussemy (for Strasbourg University Hospital); Dr Caroline Giordana, Dr Claire Marsé, Lydiane Mondot, Bruno Giordana, Robin Kardous, Bernadette Bailet, Héloise Joly, Denys Fontaine, Dr Aurélie Leplus, Amélie Faustini and Vanessa Ferrier (for Nice University Hospital); Pr Pierre Krystkowiak, Dr Mélissa Tir, Pr Jean-Marc Constans, Sandrine Wannepain, Audrey Seling, Dr Michel Lefranc, Stéphanie Blin and Béatrice Schuler (for Amiens University Hospital); Pr Stephane Thobois, Dr Teodor Danaila, Dr Chloe Laurencin, Pr Yves Berthezene, Dr Roxana Ameli, Helene Klinger, Dr Gustavo Polo, Patrick Mertens, A Nunes and Elise Metereau (for the Civil Hospitals of Lyon); Dr Lucie Hopes, Dr Solène Frismand, Dr Emmanuelle Schmitt, Mrs Mylène Meyer, Mrs Céline Dillier, Pr Sophie Colnat and Mrs Anne Chatelain (for Nancy University Hospital); Dr Jean- Philippe Brandel, Dr Cécile Hubsch, Dr Patte Karsenti, Dr Marie Lebouteux, Dr Marc Ziegler, Dr Christine Delmaire, Dr Julien Savatowky, Mrs Juliette Vrillac, Mrs Claire Nakache, Dr Vincent D’Hardemare and Mr Lhaouas Belamri (for the Rotschild fondation of Paris); Dr Philippe Graveleau, Dr Jean-Marc Trocello, Dr Camille Decrocq, Dr Frédéric Bourdain, Dr Anne Boulin, Mrs Elodie Dupuy, Dr Bérénice Gardel, Pr Béchir Jarraya and Mrs Delphine Lopez (for the Foch Hospital of Paris-Saclay University); and David Gay, Robin Bonicel, Fouzia El Mountassir, Clara Fischer, Jean-François Mangin, Marie Chupin and Yann Cointepas (for CATI (MRI acquisition management, preprocessing and data management)).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
Footnotes
ACKNOWLEDGMENTS
We thank all participants and their families for their cooperation, Déborah Meligne from ToNIC (Toulouse NeuroImaging Center - University of Toulouse III, INSERM, Toulouse) and the psychologists from the CERPPS (Study and Research Center in Psychopathology and Health Psychology –University of Toulouse II Jean-Jaurès (UT2J)) Gaelle Bongeot, Aurélie Croiset and Alice Dhellemmes for their support and reflection within this study; Antoine Pelissolo for its help and reflection considering TCI data treatment and the NS-Park French Network.
The authors are grateful for financial support from the France Parkinson charity, Lille University Hospital, and the Fédération de la Recherche Clinique du CHU de Lille (with Anne Sophie Rolland, Alain Duhamel, Maeva Kheng, Julien Labreuch, Lynda Djemmane, Florence Duflot, Professor Dominique Deplanque, Edouard Millois, Victor Laugeais, Maxime Caillier, Aymen Aouini, Pauline Guyon, Francine Niset, Valérie Santraine, Marie Pleuvret, Julie Moutarde, Laetitia Thibault).
This work was supported by the France Parkinson charity and French Ministry of Health [PHRC national 2012]. This is an ancillary study to Protocol ID: 2013-A00193-42; ClinicalTrials.gov: NCT02360683.