
Abstract
Background:
Urinary dysfunction is common in Parkinson’s disease (PD) patients and management options are limited.
Objective:
This study aimed to explore the management of urinary dysfunction by researching the special needs of PD patients.
Methods:
PD patients with urinary dysfunction who underwent urodynamic testing were recruited from a single center from October 2013 to February 2019. The urinary symptoms, International Prostate Symptom Score and Hoehn–Yahr scale were evaluated. Management was made at the urologists’ discretion with follow-up after three weeks. Urinary symptoms, urodynamics and the management of urinary dysfunction were analyzed.
Results:
A total of 187 patients with a median age of 66.2 and Hoehn-Yahr scale soccer of 2 were enrolled. Irritative symptoms were more common than obstructive symptoms, while obstructive symptoms were more common in male than female patients, except for incomplete voiding. There were 51% cases of detrusor overactivity, followed by 33% with bladder outlet obstruction, 13% had normal function, 12% had detrusor underactivity, 9% had stress incontinence, 7% had increased bladder sensation and 4% had an acontractile bladder. Tolterodine and tamsulosin were the most common therapeutic agents, respectively prescribed to 38.5% and 27.3% of the patients. Other treatments included catheterization, botulinum toxin A bladder wall injection, transurethral resection of the prostate and urethral dilatation. Urinary symptoms were improved significantly in 74.5% of the patients (p < 0.001), including 27 patients treated with tamsulosin only and 54 patients with tolterodine only.
Conclusions:
Urinary symptoms and urodynamics were highly variable in PD patients, indicating that most patients may benefit from personalized management.
INTRODUCTION
Parkinson’s disease (PD) is a chronic progressive neurodegenerative disorder that is correlated with aging, and is characterized by Lewy bodies and loss of dopaminergic neurons in the substantia nigra [1]. Globally, the prevalence of PD reached 98/100 000 in 2015, representing a 15.7% increase from 1990 [2]. Men are more susceptive than women, mainly from the ages of 55 to 65 years [3]. In China, PD affects approximately 1.7 % of those over 65 years old, and the total number of cases reaches over 2.5 million [4, 5].
PD is characterized clinically by motor disorders, including resting tremor, muscular rigidity, bradykinesia and postural instability [6]. However, the disease is now recognized as heterogeneous, with clinically significant non-motor features, such as neuropsychiatric problems, sleep disorders, sensory symptoms and autonomic dysfunction [1]. Urinary dysfunction is the most commonly reported non-motor symptom, affecting 27–64% of all PD patients [7–9]. Urinary dysfunction can occur in the early stages of the disease and worsens as the disease progress to become one of the main burdens of the patients. Moreover, PD patients with urinary dysfunction have a poorer quality of life [9–11] and higher tendency to fall [12]. However, few studies investigated the specific features and management of urinary dysfunction in PD patients [13, 14]. The objective of this study was to identify the specific features and investigate the current methods for managing urinary dysfunction in PD patients using combined evaluations of urinary symptoms and urodynamics in PD patients collected in daily clinical practice.
METHODS
Participants
From October 2013 to February 2019, PD patients with urinary dysfunction who underwent urodynamic testing were included from the neurological and urological outpatient clinics, as well as the neurological ward of Xuanwu Hospital of Capital Medical University. The patients were aged from 40–80 and all had idiopathic PD, with urinary dysfunction duration ≥1 months and sterile urine. The clinical diagnosis of idiopathic PD was adjudicated by two independent neurologists based on the UK Brain Bank criteria [15]. The Hoehn-Yahr (H-Y) scale [16] was used for neurological evaluation at “on” status. Exclusion criteria included communication difficulty, acute urine retention, history of prostate/urethra surgery, pelvic organ prolapse, cerebrovascular disease, coronary disease and H-Y scale of 5. All patients underwent routine history and physical examinations, anal sphincter electromyography, brain magnetic resonance diffusion-weighted imaging and ultrasound imaging of the urinary tract. The study was approved by the Hospital Review Board and all participants voluntarily joined this study with informed consent.
Symptom evaluation
Patients were required to finish the urinary questionnaire regarding irritative symptoms and their frequency, urgency, nocturia, and incontinence, as well as obstructive symptoms, including incomplete voiding, straining, hesitancy and weak stream. The International Prostate Symptom Score (IPSS) [17] was used to evaluate the severity of urinary dysfunction. In the IPSS questionnaire, frequency, urgency, and nocturia may reflect the state of irritative symptoms, whereas incomplete emptying, intermittency, weak stream and straining at the beginning of urination are viewed as indicative of obstructive symptoms [17].
Urodynamic evaluation
The urodynamic evaluation was completed using the UDS-600 System (Laborie Medical Technologies, Toronto, Ontario), equipped with 6 F double-channel urethral catheters and 12 F double-channel rectal catheters (Medtronic, USA). The methods and definitions used for the urodynamics conformed to the standards proposed by the International Continence Society [18]. Specially, detrusor overactivity (DO) is a urodynamic observation characterized by involuntary detrusor contractions during the filling phase, which may be spontaneous or provoked, while maximum flow rate (Qmax) is the maximum measured value of the flow rate after correction for artefacts during pressure-flow study [18]. In men, the bladder outlet obstruction index (BOOI, PDet @ Qmax –2Qmax) >40 was used to define bladder outlet obstruction (BOO), while the bladder contractility index (BCI, PDet @ Qmax + 5Qmax) <100 constitutes detrusor underactivity (DUA) [19]. For women, the following standards were used in the pressure-flow analysis: (1) BOO: PdetQmax > 30 cm H2O together with Qmax < 10 ml/s [20]; (2) DUA: conformed to ICS definition [19] and PdetQmax≤30 cm H2O together with Qmax < 10 ml/s; (3) normal: PdetQmax > 0 and Qmax > 10 ml/s; (4) acontractile detrusor: no detrusor contraction. Increased bladder sensation was defined as a decrease in the first sensation volume (100 ml < normal<300 ml) without DO during the filling phase [21].
Interventions and follow-up
The management of urinary dysfunction was made by the urologists who performed urodynamics, based on each patient’s age, symptoms, urodynamics results and motor disorders. Possible urinary dysfunction etiology was analyzed for all the patients. For patients with nocturia, fluid intake was restricted. Timed voiding and psychological counseling were provided for patients with motor disorders and anxiety caused by urinary dysfunction. Further investigations were suggested when a patient’s symptoms were mild according to IPSS or did not warrant treatment. Tolterodine was prescribed when storage symptoms/DO were dominant in patients with low risk of urinary retention, while tamsulosin was prescribed when obstructive symptoms/BOO/DUA were primarily found. Combined therapy was used when both components were found. For male patients with BOO, IPSS > 7, prostatic weight >50 g and H-Y scale 2–3, transurethral resection of the prostate was suggested. For female patients with BOO, weekly urethrocystoscopic urethral dilation was suggested. Other treatments were also suggested to the patients. The patients were followed-up after 3 weeks and post-treatment IPSS was assessed via a phone call. The study flowchart is shown in Fig. 1.
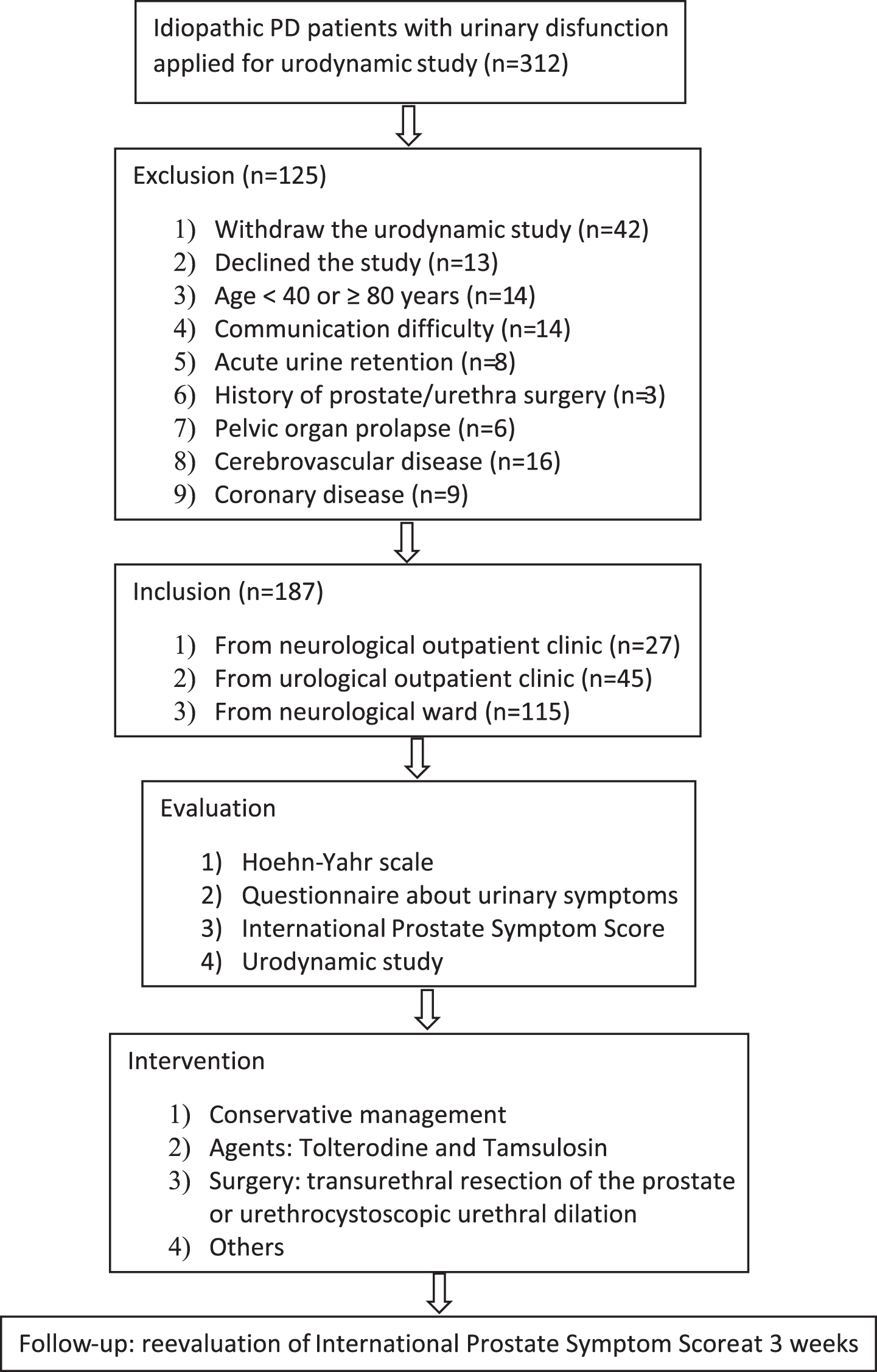
Study flowchart.
Statistical analysis
Qualitative variables were described using absolute frequencies and percentages. Quantitative variables were described using the mean, standard deviation, median and interquartile range (IQR). The independent-samples t-test was used to assess the gender differences of urinary symptoms, and the paired-samples t-test was used to assess the improvement of urinary dysfunction. SPSS software version 22.0 (IBM, Armonk, NY, USA) was used for data analysis and differences with p < 0.05 were considered statistically significant.
RESULTS
Demographic data
A total of 187 patients with a median age of 66.2 years (IQR: 58, 73) and H-Y scale of 2 (IQR: 2, 3), selected from 312 patients, were enrolled. Before urodynamic testing, 132 (70.5%) patients received drugs for PD, while 36 (19.3%) received agents for urinary dysfunction. A total of 91 (48.7%) patients had comorbidities, especially benign prostate hyperplasia in men. The patients’ characteristics are summarized in Table 1.
Demographic data
PD, Parkinson’s disease; IQR, interquartile range; BMI, body mass index.
Urinary symptoms
Irritative symptoms were more common than obstructive symptoms, while obstructive symptoms were more common in male than female patients, except for incomplete voiding (Fig. 2A). The mean IPSS, irritative and obstructive symptom scores were 18.7±7.2 (range: 4–35), 10.6±4.2 (range: 0–15) and 8.1±3.6 (range: 0–20), respectively. Male IPSS (20.2±7.6 versus 15.5±8.3) and obstructive symptom scores (12±5.3 versus 6.4±4.5) were significantly higher compared to those of females (p < 0.05). However, there was no gender difference for irritative symptom scores (9.7±4.2 versus 10.2±3.6) (p = 0.989).
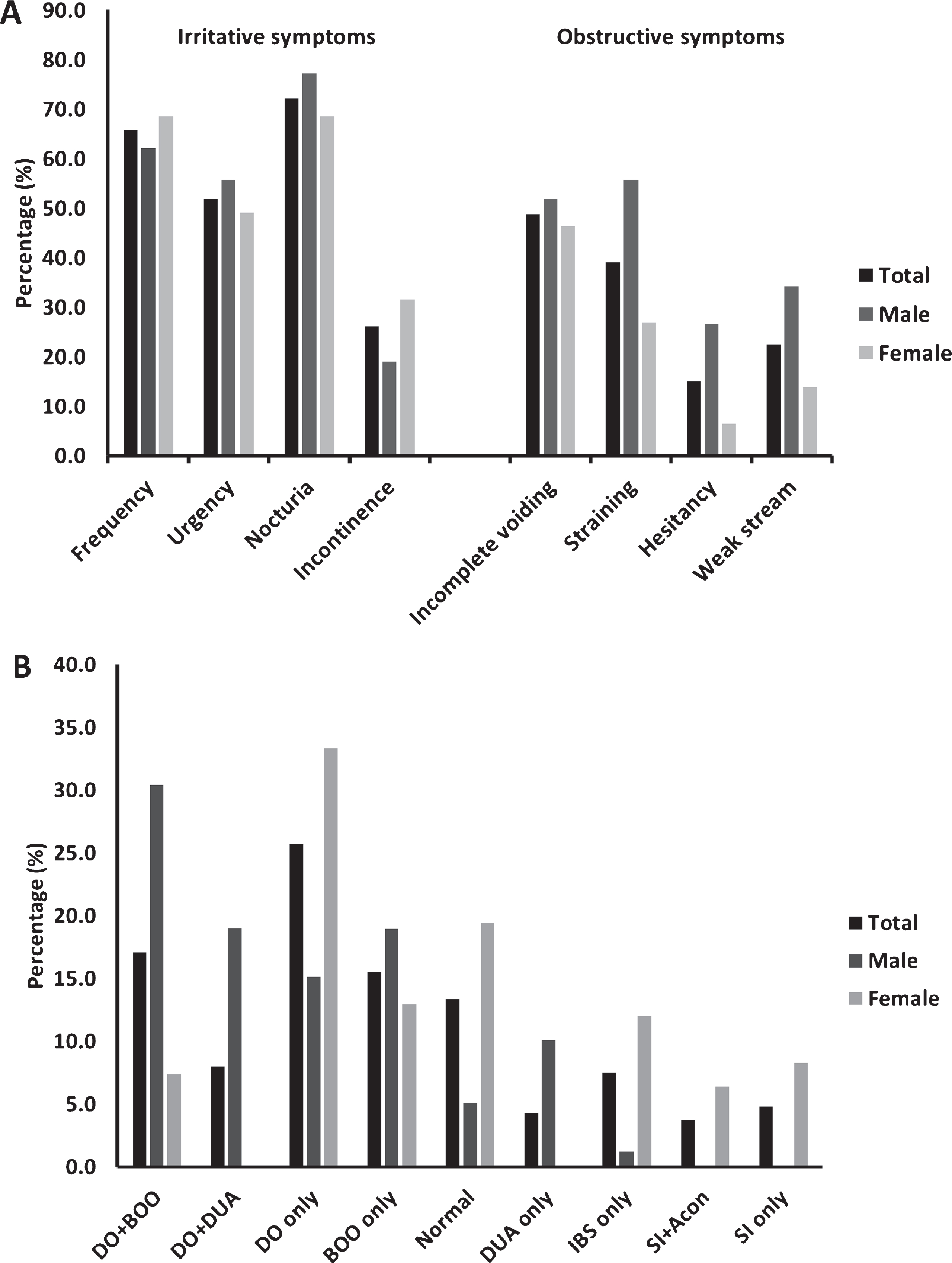
Distribution of urinary symptoms and urodynamic findings. Among the 187 PD patients with urinary disfunction, urinary symptoms (A) and urodynamics (B) were analyzed. DO, detrusor overactivity; BOO, bladder outlet obstruction; DUA, detrusor underactivity; IBS, increased bladder sensation; SI, stress incontinence; Acon, acontractile detrusor.
Urodynamic findings
Overall, 95 (51%) patients had DO and it was the most common urodynamic finding, followed by BOO in 61 (33%) patients, normal findings in 25 (13%) patients, DUA in 23 (12%) patients, stress incontinence in16 (9%) patients, increased bladder sensation in 14 (7%) patients and acontractile bladder in 7 (4%) patients. There were also obvious gender differences. DUA and DO + DUA were only found in males, while stress incontinence + acontractile bladder and stress incontinence were observed only in females. DO + BOO was more common in males, while DO only and otherwise normal findings were more common in females (Fig. 2B). Residual urine was found in 24 (12.8%) patients, and the median volume was 190 ml (IQR: 135, 240). One man with DO only showed significantly decreased detrusor compliance. The IPSS of 56 (30%) patients was in accordance with the urodynamics findings, including 34 (70.8%) patients with irritative symptoms had DO only, 15 (31.9%) patients with combined symptoms had DO + BOO or DO + DUA, while 7 (18.9%) patients with obstructive symptoms had BOO only or DUA only (Supplementary Table 1).
Management and follow-up
A total of 9 patients with abnormal urodynamics findings were found to have non-urological etiological factors contributing to their urinary dysfunction, including 1 patient with severe nocturia due to sleep disturbance and excessive drinking at night, 3 patients with increased frequency due to serious anxiety for incontinence with intentional increase of the times of voiding, 1 patient with increased frequency due to Sjögren syndrome, the main symptom of which is thirst and excessive drinking. A total of 3 patients with urgency due to PD-induced bradykinesia had difficulty going to the toilet. There was also 1 patient with typical complaints of severe stress incontinence who later was found to not have actual incontinence even during sneezing, coughing or jumping. The reason for this illusion was a persistent burning sensation around the urethra, which was relieved by vaginal estrogen cream application. Tolterodine and tamsulosin were the most common therapeutic agents, prescribed in 72 (38.5%) and 51 (27.3%) patients, respectively. Other treatments included catheterization, botulinum toxin A bladder wall injection, transurethral resection of the prostate, and urethral dilatation. Table 2 shows the overall strategies used for management of urinary dysfunction in the patients.
Management of urinary dysfunction
DO, detrusor overactivity; BOO, bladder outlet obstruction; DUA, detrusor underactivity; IBS, increased bladder sensation; SI, stress incontinence.
A total of 156 (83.4%) patients presented at follow-up. We excluded 1 patient due to prostate cancer, 4 men with indwelling catheters and two women with intermittent catheterization. Urinary dysfunction improved significantly in 111 (74.5%) patients (p < 0.001), including 27 patients with tamsulosin only and 54 patients with tolterodine only (Fig. 3). One patient stopped using tamsulosin due to hypotension. In addition, the symptoms improved to different degrees in the patients treated with tamsulosin+tolterodine, antidepressant or botulinum toxin A bladder wall injection, although a statistical comparison was not made because of the small number of patients in each treatment group. A total of 4 men were able to discontinue catheterization after tamsulosin usage, and the urinary symptoms of 4 women were relieved after weekly urethrocystoscopic urethral dilation.
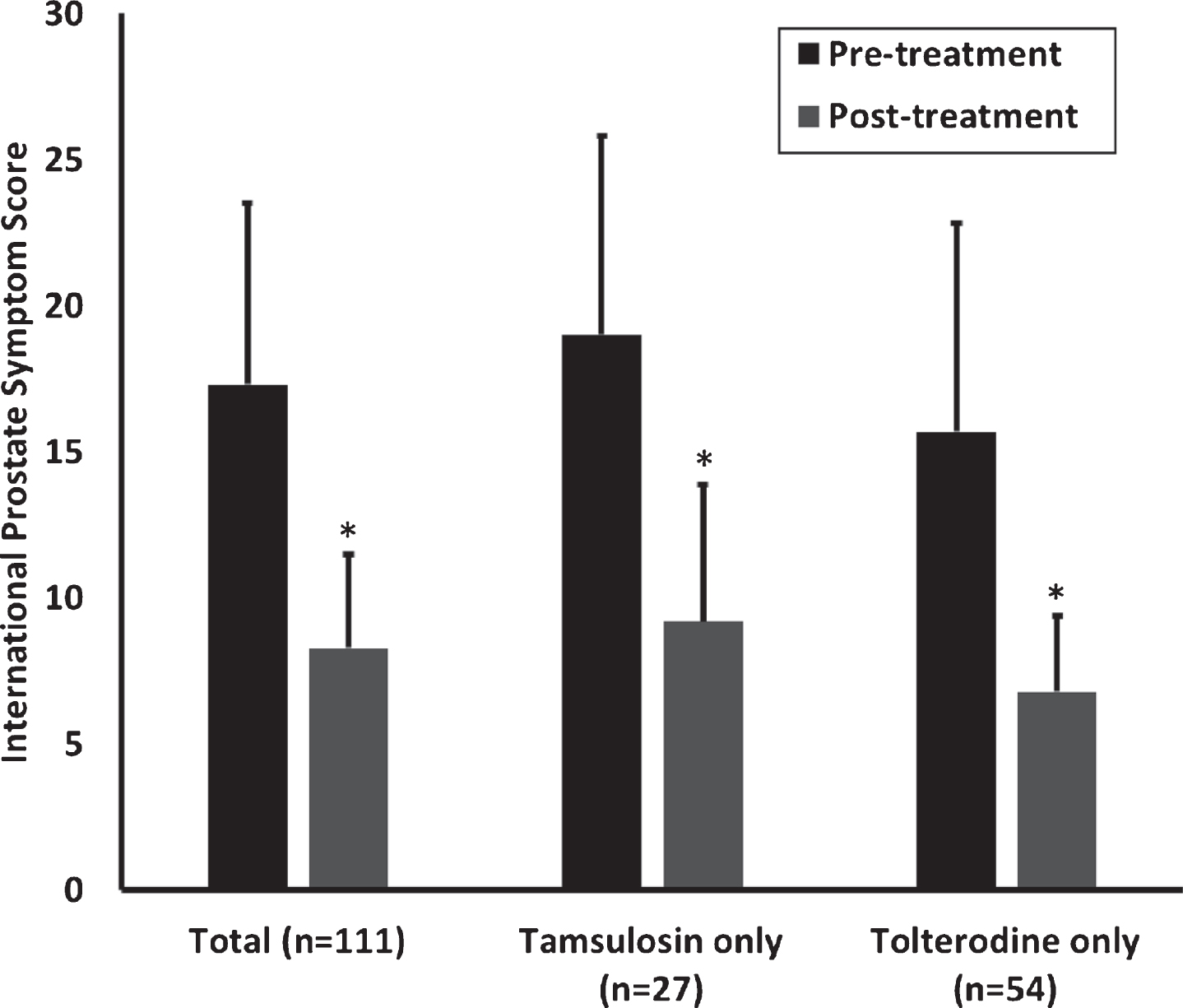
Improvement of urinary symptoms in PD patients. Among the 149 follow-up patients, urinary dysfunction was improved in 111, including 27 patients treated with tamsulosin only and 54 with tolterodine only. The 38 patients without improvement include 5 patients with tamsulosin only and 7 with tolterodine only. *p < 0.001 compared with pre-treatment.
DISCUSSION
The number of PD patients is increasing and urinary dysfunction is one of the most pronounced symptoms that severely impacts the quality of life. However, the management of urinary symptoms is usually neglected due to limited clinical evidence. Consequently, the aim of this study was to investigate the features and management of urinary dysfunction in PD, and 187 were enrolled patients. According to the results, urinary symptoms and urodynamics were highly variable in PD patients, and most patients benefited from personalized management.
The study showed that irritative symptoms predominated in PD patients, while obstructive symptoms were less frequently observed. In previous studies, nocturia (57–86%) was the most commonly observed symptom in PD patients, followed by frequency (32–71%), urgency (32–68%) and urge incontinence (21–40%) [13], which was consistent with this study. For PD patients with motor disorders, urgency and frequency became a major concern. However, daytime fluid control is more difficult because of regular activities such as taking medication or controlling constipation. Thus, the management in our search was focused on nocturia and nighttime fluid control. In addition, straining was not rare in female patients, as a previous study had showed that the prevalence was 28% [9], and we found that 26.9% of female patients had straining while 20.4% had BOO. The straining symptoms were relieved in four out of six female patients after urethral dilation.
The etiology of urinary dysfunction in PD patients is complex, and it is difficult to determine the exact impact of PD on urinary dysfunction [13]. Generally, PD medications or some other conditions such as benign prostatic enlargement can increase the symptoms of urinary dysfunction [22–24]. In the IPSS questionnaire, irritative symptoms mainly suggest DO, while obstructive symptoms suggest DUA or BOO [13]. The IPSS of only 56 (30%) patients was in accordance with the urodynamics findings (Supplementary Table 1). Therefore, it is advisable to manage refractory/complex urinary dysfunction under the guidance of urodynamics, which allows objective discrimination of the underlying bladder and voiding disorders. In this study, there were no women with DUA, while 29.1% men had DUA. By contrast, a previous study found DUA in 66% of women and 40% of men with PD [25]. Different criteria may be responsible for the different prevalence of DUA in woman, although the discrimination between BOO and DUA in women remains a vexing problem because there are no strict urodynamic criteria to establish the differential diagnosis [26].
An individualized approach is often required for the management of urinary dysfunction. Given the profound cognitive, psychological and motor limitations of PD patients, it is more important to have a discussion with individuals about outcomes before treatments [27]. Conservative management can include patient education, bladder training, fluid and diet management and/or pelvic floor muscle exercises [14, 28]. In this study, these management strategies were applied in the patients when needed, and were not only restricted to the individuals under observation.
Antimuscarinics and α-adrenergic antagonists are the most commonly used agents for urinary dysfunction. However, most such drugs have not been specifically evaluated in PD patients, including tolterodine and tamsulosin [14, 29]. Tamsulosin is a selective α1-adrenoceptor antagonist, which has a lower incidence of orthostatic hypotension compared with other α-blockers in BPH patients. In the early stage of MSA, some patients were misdiagnosed as PD. To minimize the incidence of orthostatic hypotension, we chose tamsulosin in the study. Tolterodine is the only antimuscarinic drug available in our hospital, and β3-adrenoceptor agonist mirabegron is also not available in our hospital. The efficacy and tolerability of the two drugs was confirmed by the good compliance during this study, whereby only one patient stopped tamsulosin due to orthostatic hypotension. Additionally, fewer male patients with irritative symptoms took tolterodine due to concerns regarding urinary distension. In addition, antidepressants, botulinum toxin A detrusor injecting, urethral dilatation and estrogen cream were also effective in selected patients.
The management of urinary dysfunction in the study was challenging. Among the 149 follow-up cases, 25.5% did not achieve an improvement of urinary dysfunction, and among the patients with improvement, the mean IPSS was still above 7 post-treatment. This indicates that there was only moderate success and a need for further treatment [17]. Transurethral resection of the prostate was suggested in 24 selected patients with a mean age of 65.3±7.6 years (range: 55–75) and a median H-Y scale of 2 (IQR: 2, 3), but only 7 patients accepted surgery during follow-up. There was also a lack of effective management of stress incontinence except for surgical treatment in the study. Future clinical studies are needed to develop advanced therapeutic modalities for PD-related urinary dysfunction.
The limitations of this study are as follows: 1) There was a lack of intimate collaboration between neurologists and urologists, and we did not explore the effects of PD-specific drugs on urinary dysfunction and the effects of drugs against urinary dysfunction on PD; 2) There was often no voiding diary, since it was difficult for some patients to fill out the diary; 3) IPSS is not satisfactory for assessing urinary dysfunction because it does not address incontinence, which is one of the most common disturbances in PD patients [27]; 4) There was only short-term follow-up.
Conclusions
We investigated the assessment and management of urinary dysfunction in 187 consecutive PD patients at the daily work situation. We found that the urinary symptoms and urodynamic findings were highly variable. Most patients benefited from personalized management. However, future clinical studies are needed to provide optimal treatment recommendations for PD patients with urinary dysfunction.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to report.
Footnotes
ACKNOWLEDGMENTS
This work was supported by grants from the National Natural Science Foundation of China [No. 81500578] and the Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding Support [No. ZYLX201801].