
Abstract
Background:
OFF periods impair quality of life in Parkinson’s disease but the nature and degree of this impact is largely unquantified. Optimal treatment relies on assessing the experience and impact of these periods on patients and their carepartners.
Objectives:
To understand the experience and impact of OFF periods on their lives.
Methods:
Informed by qualitative interviews we designed questionnaires and surveyed neurologists, people with Parkinson’s disease and carepartners.
Results:
50 general neurologists, 50 movement disorder neurologists, 442 patients (median disease duration 5 years) and 97 carepartners were included. The most common OFF symptoms reported by patients and carepartners were stiffness, slowness of movement and changes in gait. Non-motor symptoms were less common. A higher proportion of carepartners reported each symptom. A minority of neurologists recognized pain, sweating and anxiety as possible symptoms of OFF periods. The three OFF symptoms most frequently designated as having great impact by people with Parkinson’s disease were changes in gait, slowness and stiffness. In contrast, cognitive impairment was most frequently rated as having great impact on carepartners. OFF periods were reported to impact many aspects of the lives of both patients and carepartners.
Conclusions:
In people with Parkinson’s disease of under 10 years duration, motor symptoms of OFF periods predominate in impact, however cognitive impairment has great impact on carepartners. Education is needed for neurologists regarding the non-motor aspects of OFF. The importance of involving carepartners in the assessment regarding OFF periods is supported by the higher frequency of symptom reporting by carepartners, and the significant impact on their lives.
INTRODUCTION
OFF periods are a temporary re-emergence of symptoms of Parkinson’s disease that are often controlled or partially controlled by medication. The combination and severity of these symptoms are unique for each patient and include a broad spectrum of motor and non-motor symptoms [1, 2]. They are also heterogeneous in their temporal pattern and this can vary not only between patients but from day to day [3]. OFF periods have been shown in many studies to be associated with poor health-related quality of life in both the physical and emotional domains [4, 5]. Our scoping review of OFF experience and impact on the daily lives of patients and carepartners [6] revealed a paucity of knowledge in this area, particularly the impact on carepartners. In a survey of patient-spouse pairs, OFF periods were among several factors identified as particular stressors on mutuality (sharing of feelings and activities) in the marital relationship [7]. The social limitations imposed by OFF periods through limiting engagements outside the home were illustrated in one qualitative study,[8] and in another carepartners of people with Parkinson’s disease (PwP) living in nursing homes expressed the need for emotional support specifically relating to dealing with OFF periods.[9] Given limited prior research, we surveyed physicians, PwP and carepartners to more fully understand stakeholder views of, and the impact of OFF periods. Such knowledge can inform the development of strategies or interventions needed to support patient-carepartner-clinician discussion about the management of OFF period management.
METHODS
Overview
As part of a larger study about OFF period communication, we administered an online cross-sectional survey to PwP, carepartners and neurologists residing in the US. We complied with STROBE reporting standards (http://www.equator-network.org/).
Questionnaire development
We developed questionnaires (see Supplementary Material) concerning the experience, understanding and communication about OFF periods based on qualitative interviews with patients, carepartners and physician representatives. Preparatory interviews were performed to ensure that questionnaire content covered the main issues facing these three groups. Survey results regarding communication practices are reported separately.[10] Here we describe the physician questionnaire items addressing their perception of the range of possible symptoms of OFF periods and the PwP and carepartner questionnaire items addressing OFF period symptoms and impact. The question eliciting symptoms of OFF periods was phrased as follows: “Choose all of the symptoms you experience during OFF periods/symptoms of OFF periods experienced by the person you care for with Parkinson’s disease.” The questionnaires are provided as Supplementary Material. Patients and carepartners from the practice of one of the authors (CM) and several neurologists pilot tested the questionnaires to ensure comprehension and sound logic. Authors reviewed all feedback and incorporated it into the questionnaire.
Sampling and recruitment
We used convenience sampling to recruit PwP and carepartners through Fox Insight (https://foxinsight.michaeljfox.org/), an online data collection platform developed and maintained by the Michael J Fox Foundation. This platform allows PwP and individuals without PD to contribute longitudinal data on their medical conditions, quality of life and lifestyle. Platform participants are invited by email to participate in ancillary projects, and Fox Insight participants were sent an invitation to complete our questionnaires. Follow-up invitations were sent at 4 and 7 weeks after the first invitation if individuals did not open the email. Questionnaires were open from February 7th, 2018 to March 30th, 2018. Fox Insight PD participants were eligible to participate in this study if they self-reported a PD diagnosis, were on PD treatment, and reported the occurrence of OFF periods. Primary carepartners for someone with OFF periods were also eligible. The following explanation was provided to assist potential participants in assessing for the presence of OFF periods: “When a person with Parkinson’s disease benefits from medication, over time they can begin to experience episodes where the medications don’t work or don’t work as well. In those episodes those symptoms that are typically improved by the medication temporarily worsen. These episodes are called
Physicians were recruited through Sermo, a physician social network that also invites members to participate in clinical research (http://www.sermo.com). Sermo sent invitations by email, inviting neurologists seeing at least 10 patients with PD per month to participate. Invited physicians received a single invitation between February 22 to March 9, 2018.
Data collection
Surveys for PwP and carepartners were administered online through the Fox Insight platform using a custom software. The physician survey was programmed and administered online using Confirmit software. Answers were required to proceed to the next question. Respondents could complete their questionnaire in multiple sittings. Data entry into a database was accomplished directly by the software programs.
Statistical analysis
Differences between PwP and carepartners in frequencies of reporting severe symptom impact were tested using Chi-squared tests for proportions. If less than ten PwP or carepartners reported severe impact, the test was not conducted. Associations with demographic and disease characteristics were analyzed using logistic regression. Given that we did not have a primary hypothesis regarding which symptoms would be associated and in order to keep the false positive rate low, we adjusted all p-values for multiple comparisons. We have chosen to use the Holm method as it allows us to put an upper bound on the probability of a false positive result. The Holm method consists of finding just how much rarer an event needs to be in order to reject the null while maintaining a set false positive rate. The frequency of symptom reporting was compared between carepartners and PwP using a mixed effects logistic regression model with the reporting of the symptom as the outcome, the type of respondent (PwP, care partner) as fixed effects and crossed random effects for the symptoms and individual respondents.
This study protocol was reviewed and approved by the Research Ethics Board of the University Health Network, Toronto, Canada.
RESULTS
Sample characteristics
Physicians
Neurologist response rate was 16% (223/1393). Respondents were of similar sex distribution to non-respondents (74% and 76% male respectively), but respondents were younger (mean age 45 years) than non-respondents (mean age 57 years). Among interested respondents, 123 did not qualify and were excluded. 50 movement disorders physicians and 50 general neurologists completed the physician survey. For both physician types the median number of years in practice was more than 10.
PwP and carepartners
PwP/carepartner response rate was 13% (2,262/17,085). Due to an initial programming error precluding linkage to the main Fox Insight dataset, data from the first 1,727 respondents were invalid. Thus, responses from 442 PwP and 97 carepartners were included. There were no significant demographic or disease duration differences between those included and excluded, however those included (PwP+ carepartners) were slightly older (mean age 66 years) and had a higher proportion of female sex (51%) compared with non-respondents (mean age 63 years, 42% females). 7% of both respondents and non-respondents had post-secondary education. The demographic characteristics and the characteristics of the OFF periods of those included are shown in Table 1. All carepartners indicated that their relationship to the PwP was as a spouse or partner.
Descriptive characteristics of participating people with Parkinson’s disease (PwP) and care partners
The symptoms of OFF periods
The frequency of OFF symptoms reported is shown in Fig. 1. The most common OFF symptoms reported by both PwP and carepartners were stiffness, slowness of movement and changes in gait. Non-motor symptoms were less commonly reported. The odds of a symptom being reported by a carepartner were on average 1.94 times higher compared with PwP (95% CI: 1.44, 2.61). The disparity between carepartner and PwP reporting was greatest for ‘difficulty thinking,’ reported by 67% of carepartners vs 42% of PwP.
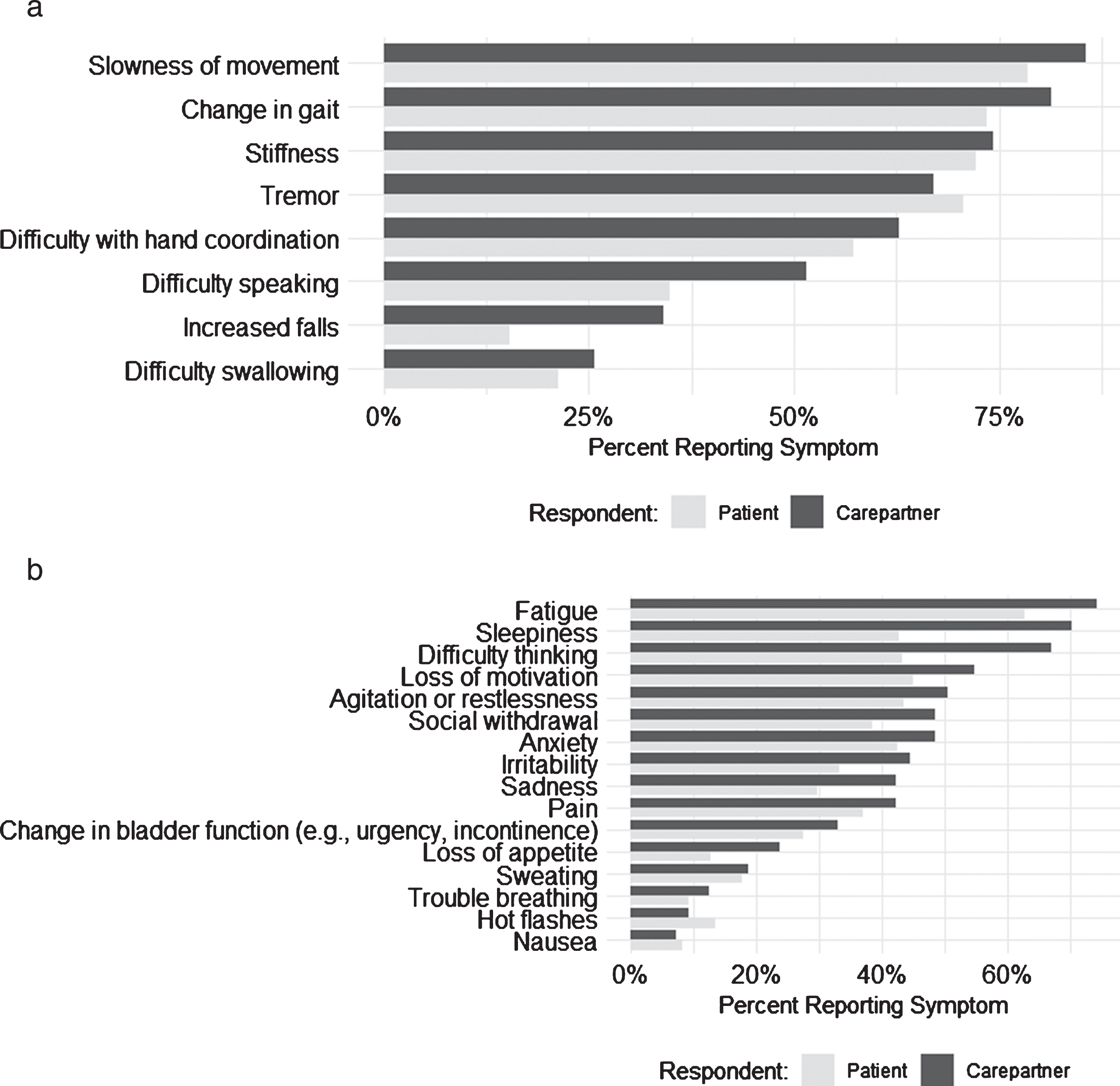
(a) Percentage of PwPs and carepartners reporting each motor symptom of OFF periods. b Percentage of PwPs and carepartners reporting each non-motor symptom of OFF periods.
After adjusting for multiple comparisons, disease duration was significantly associated with the odds of PwP reporting stiffness (OR = 1.1, 95% CI 1.1–1.2), slowness (OR = 1.3, 95% CI 1.2–1.4), changes in gait (OR = 1.1, 95% CI 1.1–1.2), falls (OR = 1.1, 95% CI 1.1–1.2) and difficulty with hand coordination (OR = 1.1, 95% CI 1.08–1.13) as OFF period symptoms. Odds ratios are reported for a one-year increment in disease duration. There was no statistically significant association between disease duration and the presence of non-motor OFF period symptoms. Stiffness (OR = 0.8, 95% CI 0.7–0.9), poor hand coordination (OR = 0.8, 95% CI 0.7–0.9) and hot flashes (OR = 0.7, 95% CI 0.6–0.9) were less likely to be reported with increasing age. Odds ratios are reported for a 5-year increment in age. Only the likelihood of reporting pain as a component of OFF periods was related to gender (more likely in females, OR = 0.49, 95% CI 0.32, 0.73). Results for all symptoms can be found in Supplementary Table 1.
Physicians indicated from a select list of symptoms whether or not each could represent an OFF period symptom. The majority of general neurologists indicated that slowness (44/50, 88%), changes in mobility (47/50, 94%) and tremor (31/50, 62%) could be symptoms of OFF periods. However, a minority indicated that pain (7/50, 14%), sweating (6/50, 12%) and anxiety (12/50, 36%) were possible OFF symptoms. Results were similar for movement disorder neurologists regarding motor features (slowness 43/50 (86%), changes in mobility 49/50 (98%), tremor 34/50, 68%)) but a higher proportion indicated that pain (22/50, 44%), sweating (15/50, 30%) and anxiety (26/50, 52%) could represent symptoms of OFF periods.
The impact of OFF periods
Participants and carepartners rated the impact of each symptom that they experience on their own (individual) daily lives. The frequency of symptoms designated as having great impact on activities of daily living are shown in Fig. 2. (Impact rated on a Likert scale of 1–5 where 0 = no impact, 5 = severe impact, Figure 2 shows the frequency of ratings 4 or 5, which we hereafter call ‘significant impact’). As a group, motor symptoms were more frequently designated as having significant impact than non-motor symptoms. The three OFF symptoms most frequently designated as having great impact by PwP were changes in gait, slowness in movement, and stiffness, all less than 30%. In contrast, cognitive impairment (“difficulty thinking”) was the symptom most frequently rated as having great impact by carepartners. Carepartners rated a number of symptoms as having great impact more frequently than PwP (Fig. 2). Sadness, anxiety, irritability, difficulty thinking, speaking, and swallowing were significantly more often rated as having great impact by the carepartner than the PwP before but not after adjustment for multiple comparisons.
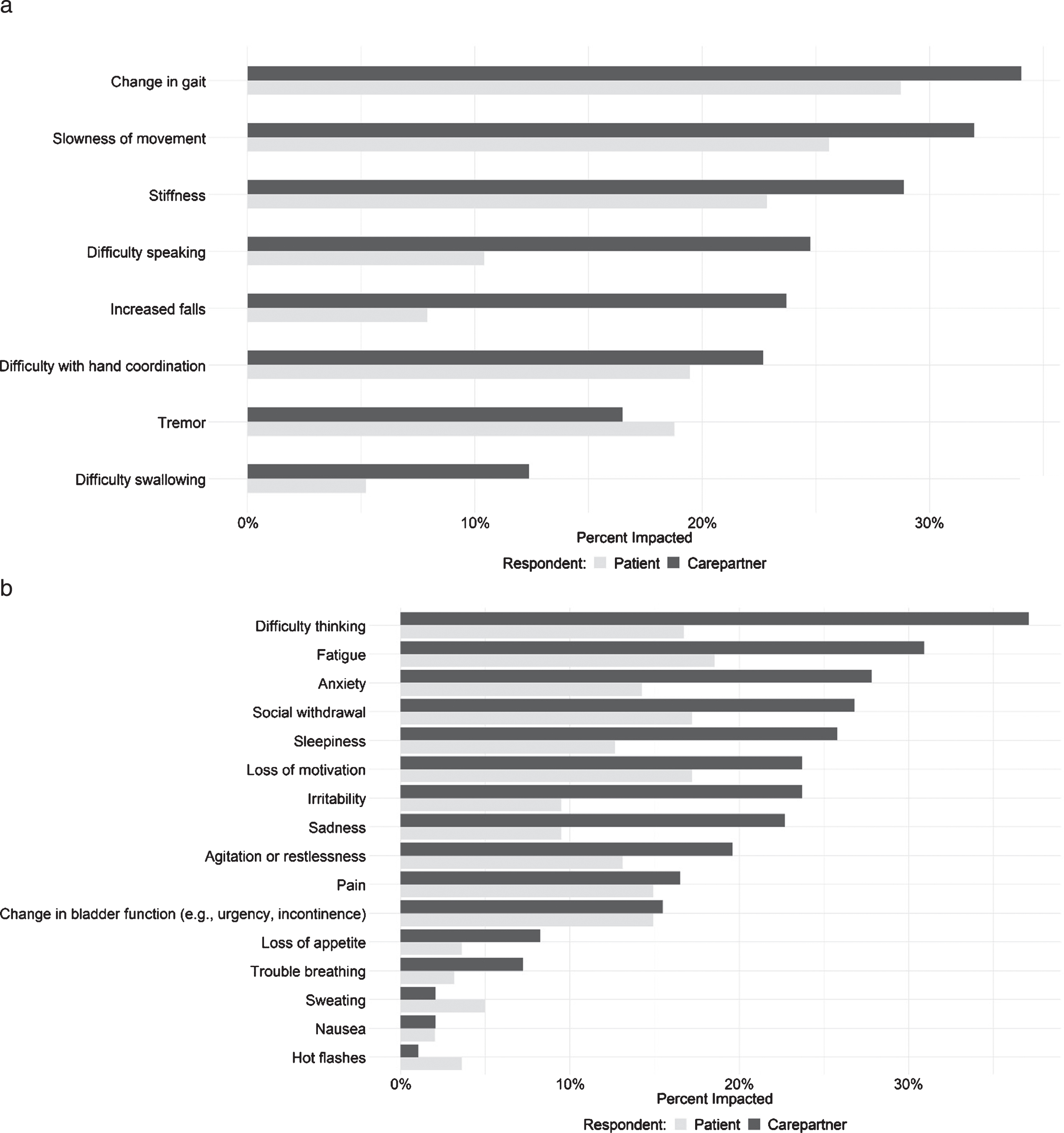
(a) Frequency of motor symptoms of OFF periods being designated as having significant impact. (b) Frequency of non-motor symptoms of OFF periods being designated as having significant impact. Significant impact = (rated 4 or 5 on a Likert scale of 1–5 where 0 = no impact, 5 = great impact).
The relationship between the likelihood of a symptom being rated by the PwP as having great impact and age, sex and disease duration is shown in Supplementary Table 2. After adjustment for multiple comparisons, change in gait, slowness of movement, stiffness, difficulty with hand coordination, pain and falls as symptoms of OFF periods were significantly more likely to be rated as having great impact with increasing disease duration. No statistically significant associations were found between symptom impact and age or sex after adjustment. Before adjustment for multiple comparisons, female carepartners were more likely to report the PwP’s difficulty thinking (OR 3.3, 95% CI 1.1–10) as having great impact than male carepartners. Gait impairment and swallowing dysfunction in the PwP were more likely to have great impact on younger carepartners (OR for gait impairment per 5-year increment in age = 1.4, 95% CI 1.1–2.0, for swallowing = 1.7, 95% CI 1.1–3.3). None of these remained significant after adjustment.
The aspects of their own lives most commonly rated by PwP as severely impacted were physical activities (164/442, 37%), household tasks (118/442, 27%), leisure/hobbies (115/442, 26%) and employment (101/442, 22%). Carepartners most frequently cited their own mood (42/97, 43%), leisure activities (35/97, 36%), freedom to leave the home (40/97, 41%) and household tasks (35/97, 36%) as severely affected. We only provided response options for aspects of life mentioned by participants in the qualitative interviews. Based on the qualitative interview responses that informed the design of the questionnaires, response options for PwP and carepartners overlapped but were not identical. The Supplementary Figure shows all response options for both groups and the frequency with which they were deemed severely affected. Frustration (57%), anxiety (35%) and embarrassment (28%) were the most common emotional reactions associated with OFF periods reported by PwP. Less commonly reported were fear (21%) and low self-esteem (21%). Among carepartners, frustration (51%) and anxiety (36%) were the most common reactions, followed closely by fear (33%). Embarrassment was much less common (5%).
DISCUSSION
Our results confirm the symptom complexity and impact of OFF periods. We extend prior literature on the impact of OFF by addressing what specific symptoms of OFF periods have the greatest impact and assessing their impact on various aspects of carepartners’ lives. OFF periods were reported to affect a broad range of aspects of daily living and elicited a range of negative emotions. In this relatively early group of patients, however, a minority designated their OFF period symptoms as having significant impact. Motor symptoms (as opposed to non-motor symptoms) were most commonly cited as having significant impact by PwP, but cognitive dysfunction during off periods was most commonly rated as having significant impact by carepartners. Considering all symptoms together, carepartners were more likely than PwP to designate symptoms as having significant impact. Another important finding was that physicians did not recognize several non-motor aspects of OFF periods.
The spectrum of OFF symptoms reported by our survey participants is in keeping with prior literature [3, 11–13]. Prior literature has described the impact of OFF periods in terms of relationships to health-related quality of life [4, 5], showing that non-motor OFF symptoms are associated with reduced HR-QoL [14], often to a greater extent than motor OFF symptoms [15, 16]. However the impact of individual non-motor symptoms relative to each other has been little studied. Our prior scoping review identified that a significant gap in the literature was in the specific impact of OFF periods or its symptoms on daily life, and we identified no new published literature on this topic.
Our survey found that OFF periods affected a broad range of aspects of the daily life of PwP and carepartners, consistent with a previous survey suggesting that the daily functions most limited by OFF periods were (in order of frequency) dressing, hygiene, getting around the house, communicating effectively, walking short distances, looking after the home, moving in bed, cutting food, getting around public places and writing [17]. The impact of OFF periods on carepartners has been less studied, as described above. The carepartner respondents indicated significant impact of OFF periods on their emotional and physical health as well as social, domestic and occupational functioning. These aspects of OFF periods can be easily overlooked if the carepartner is not included in the conversation. Recognizing the impact on the caregiver is critical considering the major role that carepartners play in the support of the PwP
The relative impact of OFF symptoms on patients and carepartners has not, to our knowledge, been reported before. The discrepancy between the ratings of impact of OFF symptoms by carepartners and PwP has several possible explanations, including cognitive impairment with poor recall or impaired self-awareness on the part of the PwP. Impaired self-awareness has been documented in PwP for both hypokinetic and hyperkinetic symptoms [18, 19] and is not correlated with cognitive test performance [18]. PwP and carepartner ratings were not paired, therefore participants were not commenting on the same OFF periods. However, the reported disease duration, and frequency and duration of the OFF periods described were very similar between PwP and carepartners. These results highlight the importance of taking into account the carepartner perspective when discussing OFF periods in order to obtain a comprehensive picture. This message is consistent with the findings of a study of psychiatric care of PwP, in which most participating psychiatrists considered that the perspective of the carepartner was critical to a correct psychiatric diagnosis [20]. In a prior survey of 47 PwP/carepartner dyads only 25% of carepartners reported that they have ever discussed with the neurologist the impact of the PwP’s symptoms on their own lives [21]. In that same study, 28% of carepartner respondents reported that they were not asked about the impact of the symptoms of PD on their own lives but indicated that they would like to have been asked. In a European survey study of PwP and carepartners 71% of 200 carepartners felt that the physician had tried to involved them in decision-making [22]. This leaves a significant proportion of carepartners who do not feel included in the discussion or involved in decision-making. Qualitative interviews that informed the development of our questionnaire explored communication between carepartners and the treating physician during the clinical evaluation and these results are published [23] separately. The main themes emerging from these interviews were the familiarity of carepartners with “off” symptoms, that carepartners were more likely to report “off” symptoms than PwP, that carepartners were not actively engaged by clinicians and the profound impact that OFF periods have on carepartners [24]. While medication adjustments should be guided by the patient’s concerns, the carepartner is a critical aspect in PD care and requires support through the journey [25, 26]. Understanding the carepartner’s concerns may trigger educational interventions or supportive counselling that could make a positive difference for both the PwP and the carepartner. For example, the carepartner’s input has been found to be important for arriving at an accurate psychiatric diagnosis in PD [20]. Also, specific carepartner support has been recommended as an integral aspect of PD care [27].
Cognitive impairment (“difficulty thinking”) in PwP during OFF periods stood out as a symptom perceived by a higher proportion of carepartners than PwP as having great impact. As noted above, impaired insight may play a role in this discrepancy, however cognitive impairment outside the context of OFF periods has been found to be a significant independent predictor of poorer carepartner quality of life (QoL) [28]. Even mild cognitive impairment in PwP has been associated with poorer caregiver health-related quality of life [29]. These results highlight the importance of assessing caregiver burden in individuals having OFF periods characterized by cognitive deterioration, and this aspect of OFF may only be revealed by discussions with the carepartner.
Our finding that motor symptoms were more frequently reported as having great impact than non-motor symptoms contrasts with previous findings that non-motor symptoms have a greater impact on health-related QoL [30]. This may relate to the relatively short (less than 10 years) duration of disease of our participants, considering that some non-motor symptoms are well known to become more prominent as the disease progresses. The relatively short disease duration of this sample may also account for the fact that we did not find an increase in non-motor symptoms of OFF periods with disease duration. The range of impact severity reported by our sample is broad, with the majority not rating their OFF period symptoms as having significant impact, but a significant minority reporting great impact. This variation underscores the importance of careful inquiry about not only the type of symptoms but also the way in which they affect the individual. Only with this information can treatment be properly guided.
In the qualitative interviews that informed this survey there appeared to be a lack of awareness among general neurologists that non-motor symptoms can be a component of OFF periods and this was corroborated in our survey showing that physicians tended not to recognize non-motor symptoms as OFF phenomena. These results are congruent with PwP and carepartner reporting of infrequent discussion of non-motor aspects of OFF periods in the encounter with their physician, as well as the minority of physicians indicating that they discuss non-motor aspects of OFF periods with their patients. These finding suggests the need for education of neurologists about non-motor fluctuations, but this is a small sample that may not be representative of all neurologists. The generalizability of these findings should be tested in a larger study with sampling strategies designed to include a representative sample of the range of neurologists caring for PwP. Improving physician awareness may not be sufficient however; a prior study examining the accuracy of movement disorder neurologist recognition of clinically significant non-motor symptoms through their routine evaluation found a >50% non-recognition of fatigue, depression and anxiety despite physician awareness of these problems [31]. Communication during the clinical encounter must also be optimized to maximize the recognition of these problems [10]. In the qualitative interviews with physicians that informed this survey physicians reported difficulty establishing whether symptoms related to PD, medication timing, or something else, and this was particularly true of non-motor symptoms [23]. Recognizing the nature of these symptoms as non-motor fluctuations can be very important as they may otherwise be mistaken for non-PD related symptoms and result in medically unnecessary procedures and/or misdiagnosis [13].
Strengths of our study include the large sample of patients and the recruitment of PwPs and carepartners through an online platform that does not restrict the sample to a specific geographic area or to those attending tertiary care centers. On the other hand, recruiting PwP and carepartners through an online platform is likely to select for highly motivated, highly educated and more mildly affected individuals that may not be representative of the general population with PD. Indeed, the median disease duration of approximately 6 years is also a relatively early group for a study of OFF periods that are likely experiencing more mild fluctuations than most. This is relevant in that the duration of OFF episodes, which increases with the duration of PD, correlates with poorer health-related quality of life [32]. The necessary exclusion of a large number of early responders to the survey due to a technical programming error raises the possibility of a less representative sample of individuals than we otherwise would have had. It is plausible that early responders which we had to exclude were more motivated to participate due to more bothersome OFF periods. Given the uncertainties surrounding sampling and responder bias it is important to focus on the relative frequency and impact of different symptoms as well as PwP-carepartner differences as opposed to the overall impact of OFF period symptoms in this sample. In addition, we did not recruit carepartners and patients as dyads, therefore differences in the responses between these groups could reflect differences in the nature of the OFF periods that they have been experiencing or exposed to. However, the descriptions of frequency and duration provided by the two groups are very similar. The questionnaires were custom designed incorporating information obtained from preceding qualitative interviews. Although they were pilot tested on a small number of patients and carepartners for readability and clarity and all suggestions incorporated, we do not have information on other properties such as test-retest reliability. The accuracy of responses may be compromised by poor recall, although we are asking them about OFF periods that they likely experience on a daily basis.
In conclusion, our work highlights the impact of OFF periods even relatively early in PD, underscoring the importance of recognizing and treating OFF periods. Future research can focus on the preferences of PwP and carepartners for different types of interventions to address these problems and the ‘trade-off’ of symptom improvement vs regimen complexity. This may differ at different disease stages, but our research would suggest it is relevant even relatively early in the disease. To understand the impact of interventions targeting OFF periods, clinical trials should report not only change in OFF time but also changes in daily function in response to treatment and where possible, incorporate carepartner reporting. The importance of involving carepartners in the assessment of OFF periods is supported by the higher frequency of symptom reporting by carepartners and the substantial impact on many aspects of their lives. In particular, cognitive decline during OFF periods should prompt inquiry of the carepartner about the impact of OFF periods. Future studies should explore the optimal way to integrate the input of the carepartner, who is not in a direct therapeutic relationship with the patient, into the decision-making process to the greatest benefit of the patient and where possible, the carepartner. In order to optimize clinical care, our study also suggests that neurologists need additional education regarding the non-motor aspects of OFF periods in order to ensure proper evaluation and treatment. Larger studies of neurologists’ knowledge will inform educational efforts.
CONFLICT OF INTEREST
Dr. Marras has received speaker honoraria from Acorda Therapeutics Inc. Drs. Armstrong, Gagliardi, Grabovsky and Rastgardani have no declarations of interest.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the Michael J Fox Foundation which received funding from Acorda Therapeutics Inc. to pursue research regarding OFF periods in Parkinson’s disease. The funding source had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.