
Abstract
Background:
Levodopa is the most efficacious medication in controlling the motor symptoms of Parkinson’s disease (PD). There continues to be a controversy as to whether levodopa remains effective after years of therapy.
Objective:
To assess the long-term effectiveness of levodopa in PD patients.
Methods:
The response to levodopa in PD patients undergoing a levodopa challenge for deep brain stimulation (DBS) surgery evaluation from June 1997 through March 2017 were evaluated. The patients were broken into four groups based on disease duration (Group I: 0– 5 years, Group II: 6– 10 years, Group III: 11– 15 years, and Group IV:≥16 years). Levodopa response was calculated based on the changes in Unified Parkinson’s Disease Rating Scale (UPDRS) motor and activities of daily living (ADL) scores in the medication ON and OFF states.
Results:
A total of 361 PD patients were included. The mean age in Group I was 59.4 years with a mean disease duration of 3.9 years (n = 29), Group II was 61 years with a mean disease duration of 8.1 years (n = 131), Group III was 64 years with a mean disease duration of 12.8 years (n = 143), and IV was 66.5 years with a mean disease duration of 18.5 years (n = 58). There was a significant improvement in UPDRS motor and ADL scores after the levodopa challenge for all groups.
Conclusions:
In a subgroup of PD patients who were evaluated for DBS surgery, there was a marked improvement in UPDRS motor and ADL scores which did not decrease with disease progression.
INTRODUCTION
Since its discovery in 1967, levodopa continues to be the most potent agent in the treatment of Parkinson’s disease (PD) [1]. This treatment is not without side effects and can lead to dyskinesia, motor fluctuations, excessive daytime sleepiness (EDS), and hallucinations which are seen more commonly in the later stages of PD [1]. As the disease progresses, other symptoms such as imbalance, cognitive dysfunction, and postural abnormalities appear which are typically dopamine resistant [1]. Consequently, there is a common misconception and controversy as to whether levodopa enhances disease progression, loses efficacy, and should be delayed because of the risk of dyskinesia [2]. The delayed initiation of levodopa often leads to more disability because of inadequate treatment [2]. Therefore, it is critical to understand the long-term efficacy of levodopa so that patients maintain the greatest benefit with the fewest side effects throughout the disease course.
As the general care of patients with PD has improved, the prevalence of advanced stage PD is likely going to increase. Since many of the patients with a longer disease duration have dopamine resistant symptoms, it is important to understand the effect of levodopa in this group. This study examined the improvement with levodopa in Unified Parkinson’s Disease Rating Scale (UPDRS) activities of daily living (ADL) and motor scores in PD patients based on the disease duration and to compare the degree of improvement throughout the course of the disease.
METHODS
Participants
This study included 361 patients diagnosed with PD and evaluated for deep brain stimulation (DBS) surgery from June 1997 through March 2017 by a movement disorder specialist. Patients were referred for surgery for medication-resistant motor fluctuations, dyskinesia or tremor. Patients intolerant to levodopa and those who had previous brain surgery (DBS, pallidotomy, or thalamotomy) were excluded. All patients were evaluated in the OFF state defined as receiving no PD medications for at least 12 hours and after taking their PD medications and achieving their typical ON state. L-dopa equivalent daily dose (LEDD) was calculated based on an online calculator [3]. All the participants signed consent approved by the University of Kansas Medical Center for their data to be used for research.
Clinical assessment
All patients underwent a standardized assessment which included a complete UPDRS assessment in practically defined medication OFF and ON states. Other parameters such as Mini-Mental Status Examination (MMSE), Parkinson’s Disease Quality of Life Questionnaire (PDQ-39), dyskinesia duration, and off duration were recorded as well. Montreal Cognitive Assessment (MoCA) scores were converted to Mini-Mental State Examination (MMSE) when MoCA scores were available instead of MMSE [4]. These assessments were all prospectively collected. The included participants were assigned to one of four groups based on the duration of disease (Group I: 0– 5 years, Group II: 6– 10 years, Group III: 11– 15 years, and Group IV:≥16 years).
Statistical analysis
Analysis of variance was used to compare changes in assessments across groups with Bonferroni corrections applied. Within groups, paired t-tests were used to examine differences in ON vs. OFF states.
RESULTS
A total of 361 PD patients (113 females) were included in the study. The demographics and outcome measures are presented in Table 1. As shown in Fig. 1, after the levodopa challenge, there was a significant improvement in UPDRS Motor and ADL scores in all four groups, although the improvement in those with the shortest disease duration was less when compared to the other three groups which were similar to each other. The data in Table 2 reveal that the individuals with the shortest disease duration had little improvement in tremor when compared to the other three groups; although all groups had a significant improvement in tremor with levodopa. There was also a significant improvement in bradykinesia, rigidity, and postural instability and gait (PIGD) in all four groups when comparing medication OFF and ON conditions; however, the degree of improvement was less in group I when compared to the other groups. Also, there was a greater improvement in bradykinesia, rigidity, and PIGD in group III when compared to group IV.
Demographics of the participants included in the study
Demographics of the participants included in the study
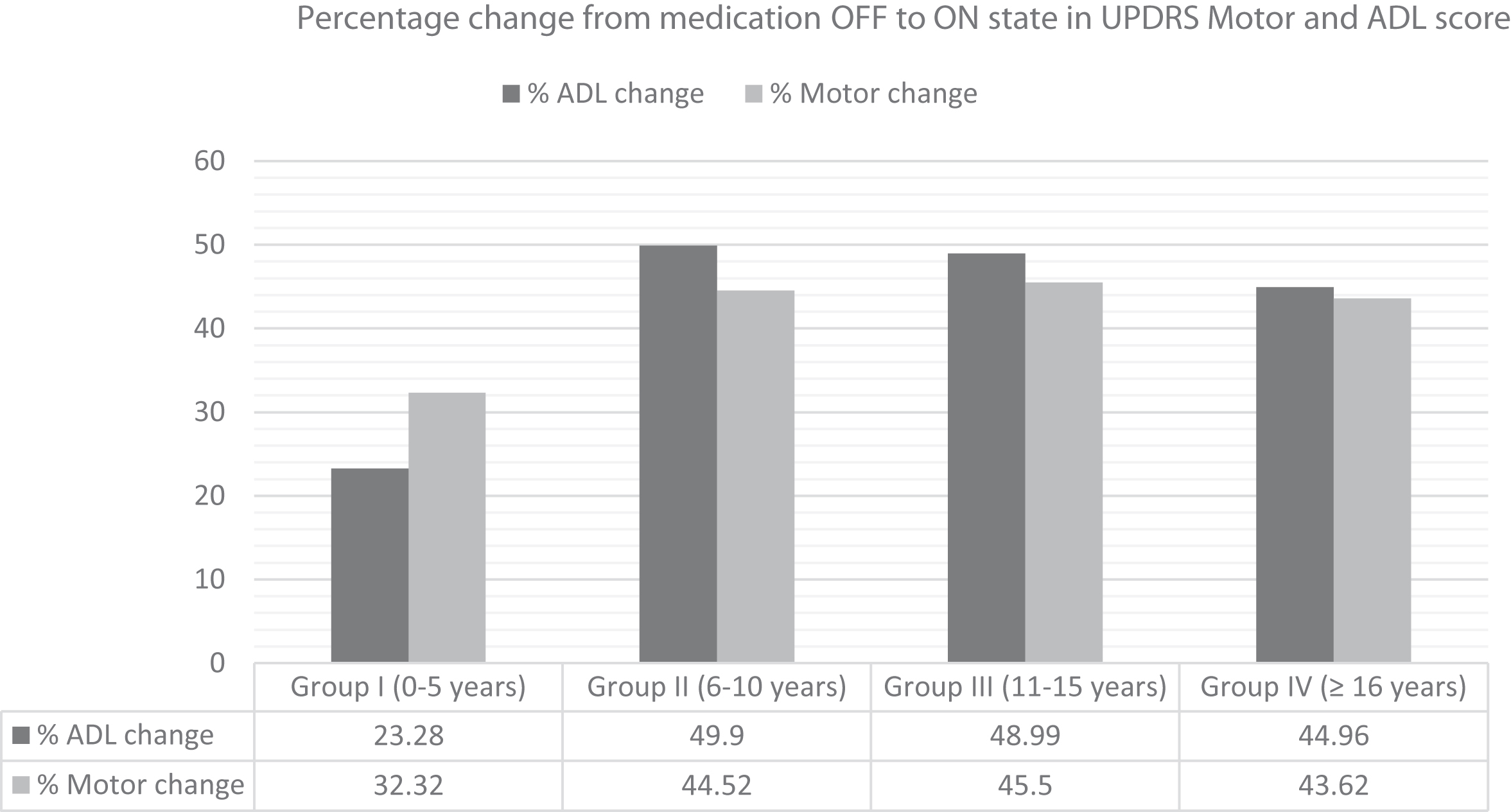
Percentage change in motor and ADL score following OFF and ON testing. This shows an improvement in UPDRS Motor and ADL scores in all the four groups following OFF and ON testing.
Percentage change from medication OFF to ON state
The patients with the longest disease duration were older and had greater UPDRS ADL and motor scores in the OFF state compared to those with disease duration < 10 years. The duration of dyskinesia and duration of OFF time were significantly less in those with disease duration < 5 years when compared to the other three groups which were not different from each other. PDQ-39 quality of life scores improved equally for all four groups, and there were no differences between groups in the PDQ-39 subscales of ADLs, emotional wellbeing, stigma, social support, cognition, communication, and bodily discomfort. However, PDQ-39 mobility subscores revealed less disability in the shortest disease duration group compared to the other groups which were not different from each other. The mean MMSE scores in all four groups were around 28, LEDD was increased with disease duration, but was not statistically different among the four groups.
This study confirms that levodopa use leads to an improvement in both motor and ADL scores on the UPDRS even in patients with long disease duration [5, 6]. Furthermore, there was no significant degradation of benefit over time as shown in Fig. 2. The likely explanation for a lesser degree of benefit in patients with a disease duration of less than 5 years is the presence of medication-refractory tremor [7]. Occasionally, levodopa and dopamine agonists are not very effective in controlling PD tremor, and this subtype of patients are considered for DBS surgery. It is possible that due to disease progression, there is less improvement in PIGD with levodopa which explains a greater improvement in group III as compared to group IV [8].
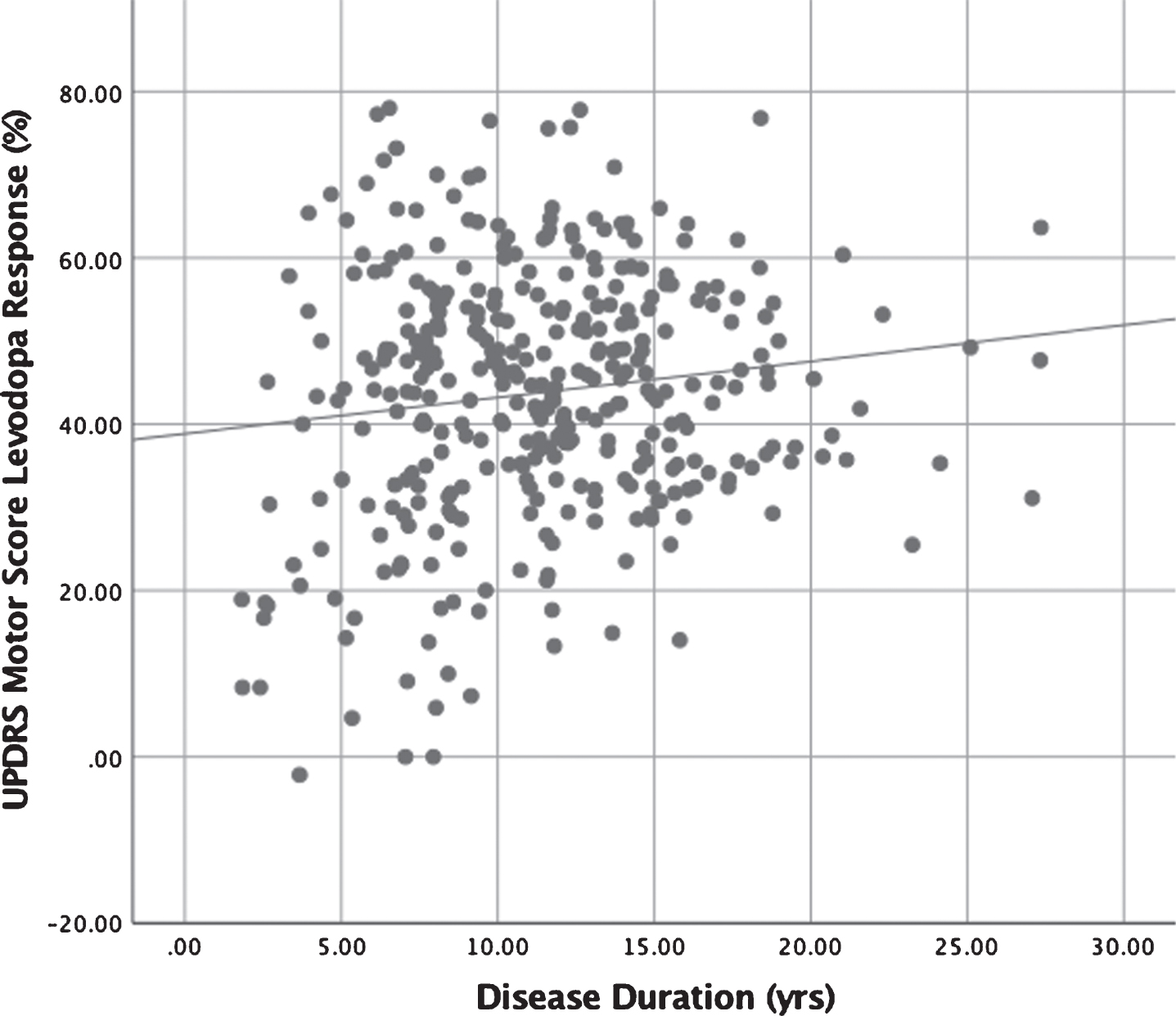
Scatter plot demonstrating the relationship between disease duration (in years) and change in UPDRS motor score (%) with levodopa. This demonstrates an improvement in UPDRS motor score (%) regardless of the disease duration. Some patients with a shorter disease duration have less benefit which is seen with tremor dominant disease.
These findings may be helpful for physicians treating PD. With disease progression, the duration of benefit with levodopa has been controversial, and it has been reported to decrease over time [2]. This may lead to a false belief among physicians, patients, and caregivers that initiating early levodopa is leading to disease progression or may reduce the long-term effect of levodopa. Earlier studies have also revealed that levodopa does not lead to dopaminergic neuronal loss [9]. As seen in the PD-MED trial, earlier initiation of levodopa leads to a better functional outcome and the use of dopamine sparing agents often leads to non-motor side effects such as impulse control disorders and excessive daytime sleepiness [10]. Another reason for delayed initiation of levodopa stems from the fear of dyskinesia and motor fluctuations. Disease duration, young age of onset, and the daily dose of levodopa have been found to be factors behind the development of motor fluctuations and dyskinesia [11, 12]. However, in our cohort, those with less than 5 years disease duration had less OFF time and dyskinesia compared to those with longer disease duration, but there were no differences between the groups after 5 years.
Our study also showed that there was no decrement in levodopa response even in the group with a disease duration of more than 16 years. This is an important finding as different delivery methods of levodopa are being developed to avoid motor fluctuations, and dyskinesia [13]. In individuals with a long disease duration experiencing motor fluctuations and dyskinesia with oral medications, other delivery methods of levodopa can be considered as well as DBS surgery. There was no significant difference in the duration of dyskinesia, OFF duration, or LEDD in those with greater than 5 years of disease. This may be related to the study population, as all were being evaluated for DBS, for which medication resistant motor fluctuations and dyskinesia are common reasons for surgical referral. The disease course of PD is also influenced by the subtype which is based on the initial presenting symptoms and signs [14]. Patients with medication-resistant tremor-dominant PD are also often referred for DBS. The current findings suggest that this may have contributed to the reduced levodopa response shown in the shortest disease duration group, as they had significantly less improvement in tremor with levodopa compared to the other groups. Consequently, a limitation of this study is the inclusion of patients who were being considered for DBS surgery only. Our study, therefore, did not include subjects with significant cognitive impairment, uncontrolled behavioral issues, or were otherwise not eligible for DBS [15, 16]. Therefore, these results cannot necessarily be generalized to all PD patients.
In conclusion, in this report, PD patients continued to receive significant benefit from levodopa even after 16 years of disease duration. Therefore, levodopa use should not be delayed in PD patients due to the fear of ineffectiveness with a longer duration of levodopa exposure. Further studies are required to see if this benefit is seen in the general PD population as well.
CONFLICT OF INTEREST
H.V. Gupta reports no disclosures. Kelly E. Lyons has received consulting fees from ACADIA and the Parkinson’s Foundation. Nathaniel Wachter reports no disclosures. Rajesh Pahwa, MD has received consulting fees from Abbvie, Abide, ACADIA, Acorda, Adamas, Cynapsus, Global Kinetics, Ionis, Lundbeck, Neurocrine Biosciences, Prilenia, St. Jude Medical, Sunovion, Teva Neuroscience, UCB and US WorldMeds. Received research grants from Abbott, AbbVie, Acorda, Adamas, Biogen, BMS, Boston Scientific, Cala Health, Cavion, Cynapsus, Intec, Jazz, Kyowa, Lilly, National Parkinson Foundation, NIH/NINDS, Parkinson Study Group, Pfizer, Prexton, Roche, Sunovion and US WorldMeds.
Footnotes
ACKNOWLEDGMENTS
This study was funded by the Helen Gold Research Fund.
Statistical analysis was performed by Kelly E. Lyons.