
Abstract
Background:
Although several studies have reported a correlation between Behçet’s disease (BD) and Parkinson’s disease, this association has not yet been clarified.
Objective:
To determine the risk of Parkinson’s disease in patients with BD.
Methods:
BD patients (n = 17,179; mean age, 51.12±8.09 years; male, 34.95%) without known previous diagnosis of Parkinson’s disease were selected from the Korean National Health Insurance Database between 2010 and 2013. An age- and gender-matched control population of individuals without BD was randomly sampled at a ratio of 3:1 (n = 34,575). Both cohorts were followed for development of Parkinson’s disease until 2015.
Results:
Among a total of 11,525 BD patients, 50 (0.43%) developed Parkinson’s disease, whereas only 51 among the 34,575 individuals in the non-BD group developed Parkinson’s (0.15%, P < 0.0001). The incidence of Parkinson’s disease was significantly higher in BD patients than in controls. In addition, during the follow-up period, patients with BD were more likely to be diagnosed with Parkinson’s disease than those in the non-BD group.
Conclusions:
BD patients had a higher risk of Parkinson’s disease compared to non-BD controls. Physicians should carefully monitor patients with BD for potential development of Parkinson’s disease.
Keywords
INTRODUCTION
Behçet’s disease (BD) is a systemic inflammatory disease with a high incidence in the Middle East and Eastern Mediterranean [1, 2]. A large, population-based study was conducted in 2017 to investigate the prevalence and mortality of BD in South Korea from 2006 and 2015; the incidence was 26 patients per 100,000 individuals, which was much higher than in other countries [3]. The aetiology of this disease is unknown; however, HLA-B27 has been strongly suggested as one of the genetic factors that contributes to the pathogenesis of BD [1].
BD can affect every organ of the body, including the central nervous system (CNS), and symptoms are caused by vasculitis [2]. To date, there have been many studies on the incidence of metabolic diseases, such as diabetes mellitus (DM), hypertension (HTN), and dyslipidaemia, in patients with BD, and the reported incidences have been significantly higher than those found in the general population [3]. The association between BD and cancer has also been reported [1]. However, the comorbidities seen in BD patients have not been fully evaluated.
Neurological involvement has been reported in 1.3∼59% (the mean 9.4%) of BD patients and the frequency is very variable depending on study design [4]. Common manifestations are meningoencephalitis and brain stem syndrome, which are associated with disease-related mortality. Parkinson’s disease as a neurological symptom of BD has rarely been reported, and there is little research on the association between BD and Parkinson’s disease. In fact, there has been only a single case report of Parkinson’s disease in a patient with BD [2].
Here, we aimed to investigate the association between prevalence of Parkinson’s disease in BD patients using the Korea National Institutes of Health database, which has a high prevalence of BD. We determined the risk of Parkinson’s disease in patients with BD and compared it with the risk of Parkinson’s disease in patients without BD using a nationwide insurance database in the Republic of Korea.
MATERIALS AND METHODS
Data collection
This study used data collected from the Korean National Health Insurance Service (NHIS) Claims Database (in which diagnoses are recorded using the International Classification of Diseases, Tenth Revision [ICD-10] code), which contains all claims data for the Korean NHI program, the Korean Medical Aid program, and long-term care insurance from each year. Because all citizens in the Republic of Korea are mandatorily enrolled in the National Health Insurance Service (NHIS), the Korean NHIS is a universal healthcare system that provides almost 100% coverage for the entire Korean population. Therefore, the Korean NHIS database is popularly considered to represent the entire South Korean population, and has been used previously in population-based studies. This study was approved by the Institutional Review Board of the Korean National Institute for Bioethics Policy (NHIS-2018-1-328) and the Ethics Committee of Uijeongbu St. Mary’s Hospital, Catholic University of Korea (UC18ZESI0061), and was conducted according to the principles of the Declaration of Helsinki.
Study population
To evaluate the relationship between BD and Parkinson’s disease, all BD patients registered between 2010 and 2013 (n = 17,179) were extracted from the NHIS database. The year in which patients first underwent the health examination was considered the index year. We excluded patients under 40 years (n = 5,521), and patients who had been diagnosed with Parkinson’s disease before the index year (n = 133). For the control cohort, an age- and gender-matched population without BD was randomly extracted at a control-to-case ratio of 3:1. Finally, a total of 11,525 patients with BD and 34,575 age- and gender-matched controls were enrolled as the study population (Fig. 1). These cohorts were followed for Parkinson’s disease until 2015.

Flow chart of this study.
Definition of BD and Parkinson’s disease
This study used a subset of data on rare, incurable diseases from the Korean NHIS database. Parkinson’s disease and BD are categorized as rare, incurable diseases designated by the Korean government for expanded NHIS benefit coverage. If patients with Parkinson’s disease (ICD-10 code. G20) or BD (ICD-10 code. M35.2) apply for a rare incurable disease certificate (codes for rare incurable diseases: V124 for Parkinson’s disease and V139 for BD), the Korean NHIS reduces the cost by 10%. The study enrolled all patients with BD within the rare incurable disease data subset (ICD-10 code, M35.2 and V139) and the development of Parkinson’s disease was assessed using the diagnostic codes (ICD-10 code, G20 and V124).
Covariates
We evaluated age, gender, habitat (urban vs. rural), and income status (quartiles) of each individual. Other health conditions, such as DM, HTN, dyslipidaemia, congestive heart failure (CHF), ischemic heart disease (IHD), stroke, and depression, were assessed. Covariates were defined using ICD-10 codes: DM (E11-14), HTN (I10-13 and I15), dyslipidaemia (E78), CHF (I50), IHD (I24 and I25), stroke (G46), and depression (F32 and F33).
Statistics
The patients’ baseline characteristics are presented as means plus or minus standard deviations (SDs) or numbers and percentages. Continuous variables are presented as means plus or minus SDs, and categorical variables are presented as numbers and percentages. To compare characteristics between groups, Student’s t-test was used for continuous variables, and chi-square test was used for binary and category variables. The incidence rates (IR) of Parkinson’s disease were calculated by dividing the number of incident cases by the total follow-up period duration and are expressed per 1000 person-years. The cumulative incidence of Parkinson’s disease was calculated using the Kaplan-Meier method. The relative risk of developing Parkinson’s disease was expressed as the hazard ratio (HR) and 95% confidence interval (CI) using a Cox proportional-hazards regression analysis. The HR and 95% CI for each group relative to the reference were also calculated. Model 1 is crude, while model 2 was adjusted for income status, habitat, DM, HTN, dyslipidaemia, CHF, IHD, stroke, and depression. Statistical significance was defined as a two-sided P-value less than 0.05. Data were analysed using SAS version 9.4 software (SAS Institute; Cary, NC, USA).
RESULTS
Each group was age- and gender-matched; 34.95% of patients were male, and the mean age was 51.1±8.1 years. Prevalence of HTN (19.71% vs. 21.64%, P < 0.0001), dyslipidaemia (12.36% vs. 17.06%, P < 0.0001), CHF (0.74% vs. 1.61%, P < .0001), IHD (4.81% vs.8.62%, P < 0.0001), stroke (1.82% vs.3.62%, P < 0.0001), and depression (4.92% vs.13.08%, P < 0.0001) was significantly higher in patients with BD than in the control group (Table 1).
Baseline characteristics of the Behçet’s disease and control groups
Incidence of Parkinson’s disease in BD and control groups
Among 11,525 BD patients, 50 (0.43%) developed Parkinson’s disease, whereas only 51 among 34,575 non-BD patients developed Parkinson’s (0.15%, P < 0.0001). The incidence of Parkinson’s disease was significantly higher in BD patients than in controls. During the follow-up period, which ranged up to six years for some individuals, patients with BD were more likely to be diagnosed with Parkinson’s disease than those in the non-BD group (all P < 0.0001 by log-rank test). Figure 2 shows the cumulative incidence of Parkinson’s disease.
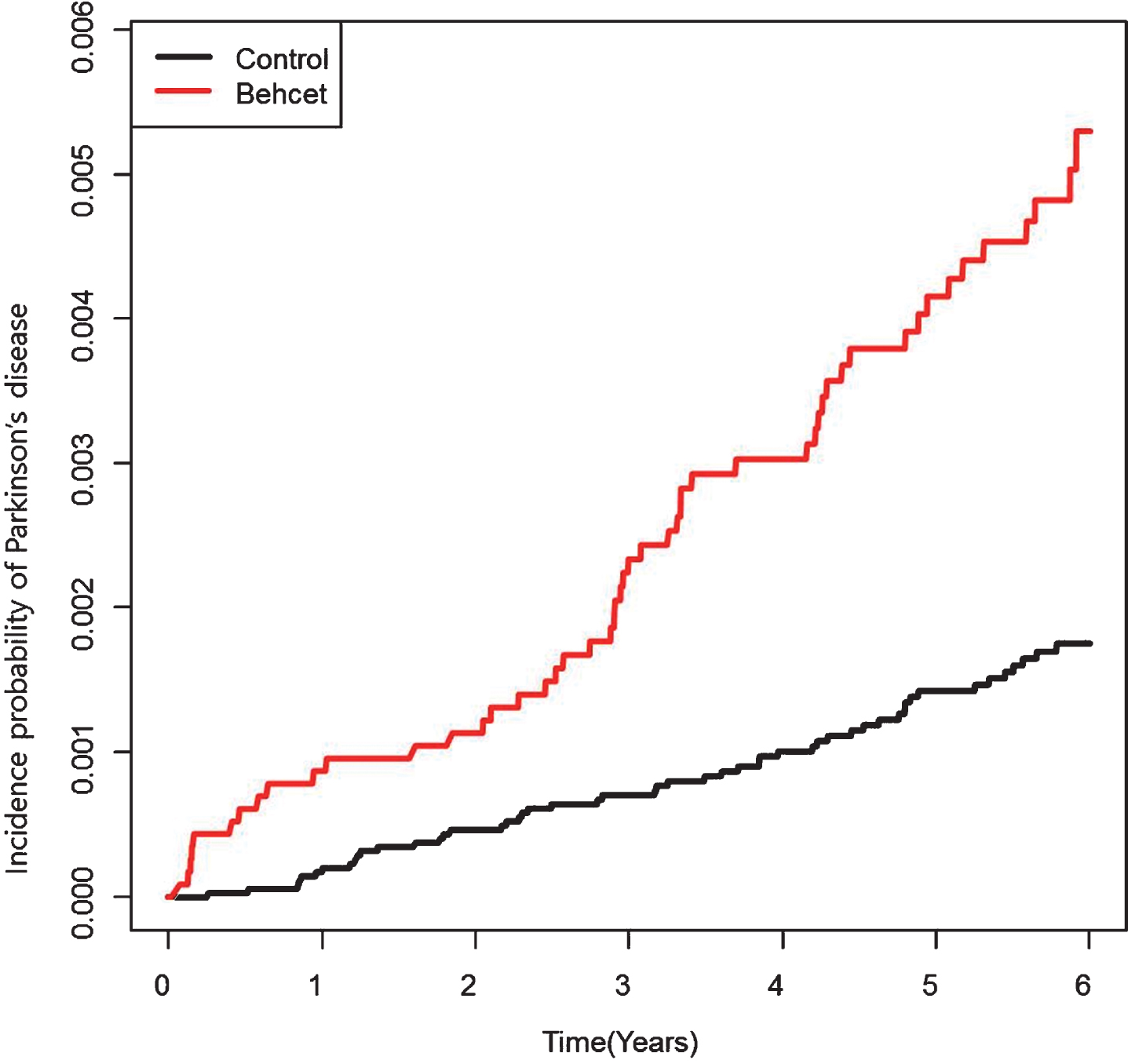
The cumulative incidence of Parkinson’s disease in both Behçet’s disease patients and controls (log-rank P-value <0.0001).
Relative risk of Parkinson’s disease in BD and control groups
The crude IRs of Parkinson’s disease in the BD and control groups were 0.85 and 0.29 per 1000 individuals, respectively. The HR of Parkinson’s disease in the BD group was 2.96 (95% CI, 2.004–4.372) compared with the control group. After adjustment for age, gender, income status, habitat, DM, HTN, dyslipidaemia, CHF, IHD, stroke, and depression, the HR was 2.466 (95% CI, 1.654–3.677) (Table 2). The increased risk of Parkinson’s disease in BD patients was similar in the subgroup analysis of age, gender, income status, habitat, DM, HTN, dyslipidaemia, CHF, IHD, stroke, and depression, with no variable being significantly associated with this increased risk (Fig. 3).

Relative risk of Parkinson’s disease according to subgroup.
Parkinson’s disease incidence rates and related events in the Behçet’s disease and control groups (P-value < 0.0001)
Model 1: No adjustment; Model 2: Adjustment for income status, habitat, DM, HTN, dyslipidaemia, CHF, IHD, stroke, and depression.
DISCUSSION
This is a large, population-based cohort study to investigate the risk of Parkinson’s disease in patients with BD using data from the Korean NHIS database. This study revealed that the IR and HR of Parkinson’s disease in the BD group were both higher than those of the control group.
BD is a systematic inflammatory disease, and involvement of the central nervous system appears in 10∼20% of BD patients [5]. Brain parenchymal involvement is more common in BD patients than peripheral nervous system involvement [6]. Neurological involvement in BD was first reported in 1957, and three types of clinical syndromes were described—brain stem disturbance, meningomyelitis, and confusional syndrome (since renamed delirium)—which result in chronic, progressive conditions, such as dementia and Parkinson’s disease [7]. However, until now, the association between Parkinson’s disease and BD had not been clarified. Only a few studies on the connection between BD and Parkinson’s disease have been reported, such as case reports of paroxysmal focal dystonia, Parkinson’s disease syndrome, and chorea in BD patients with neurological manifestations [4, 8]. The neurological involvement seen in Behçet’s disease is known to be caused by vasculitis of small vessels. A cerebrospinal fluid study in neuro-BD patients showed high concentration of IL-6, which is considered to play a main role in inflammatory neurodegeneration [4, 10]. Brain magnetic resonance imaging (MRI) can be diagnostic for neuro-BD, and the lesions seen on MRI are typically localized to the diencephalon, basal ganglia, and, less frequently, at the level of the periventricular area and subcortical white matter [5]. The substantia nigra pars compacta, which is one of the functional components of the basal ganglia, plays an important role as the source of the striatal input of dopamine. Therefore, basal ganglia involvement in BD patients can cause Parkinson’s disease [2, 11].
Parkinson’s disease is a common neurodegenerative disease. Degeneration of dopamine-producing neurons in the substantia nigra pars compacta can cause the clinical manifestations of Parkinson’s disease, such as tremors, rigidity, slow movement, and postural instability [12]. Although many studies have investigated the pathophysiology of Parkinson’s disease, its aetiology has not yet been fully elucidated [13–15]. Neuroinflammation is one of the pathophysiological components of Parkinson’s disease and according to one theory, activated microglia produce inflammatory mediators, such as cytokines and prostaglandins, that play important roles in the causation and progression of neurodegenerative diseases [12]. Therefore, anti-inflammatory agents have neuroprotective qualities and may be used as potential disease-modifying treatments for Parkinson’s disease [16]. Although there has been no definitive study on the association between BD and PD, we hypothesized that the development of Parkinson’s disease in BD patients may be caused by vasculitis or neuroinflammation in the basal ganglia due to systemic inflammation.
Associations between BD and metabolic diseases has been shown in several studies [3, 17]. In this study, our results also showed high incidences of metabolic diseases (DM, HTN, dyslipidaemia), cardiovascular disease (CHD, IHD), and stroke in patients with BD. The incidence of depression in the BD population is known to be high [18, 19]. In agreement with these data, this study showed a higher incidence of depression in the BD group compared to the control group. The development of Parkinson’s disease has been associated with several chronic comorbidities, including metabolic diseases [20, 21], ischemic heart diseases [22], stroke [23], and psychiatric diseases [24]. Therefore, we adjusted for these comorbidities when examining Parkinson’s disease in BD patients. After adjustment for these chronic comorbidities, the increased HR for Parkinson’s disease in BD patients persisted (Table 2).
The relative risk of Parkinson’s disease was predominantly observed in male BD patients (Fig. 3). The incidence of BD is higher in females than males; however, male BD patients are known to have a more severe disease course and a worse prognosis. This is because the risk of vital organ involvement is higher in male BD patients. In South Korea, neurological involvement and complications have also been reported to be higher in male BD patients [25].
There are several limitations to this study. First, data regarding potential risk factors for Parkinson’s disease, such as family history, toxin exposure, or medications were not obtained. Second, subjects in this study were relatively young (mean age of 51.8±8.1 at enrollment) after excluding the subjects who had previously diagnosed PD. More than 90% of individuals in this study were between the ages of 40 and 64. During the follow-up period, there may be concern about an ascertainment bias that BD patients were more likely to see their doctors and therefore be diagnosed with PD earlier. A long-term follow-up study is needed to come to conclusions on this issue.
Although numerous factors are responsible for the development of Parkinson’s disease, this study demonstrates that BD, which is a systemic inflammation disease, can be one of the risk factors for Parkinson’s disease. Further studies on the relationship between BD and Parkinson’s disease will be needed.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
Footnotes
ACKNOWLEDGMENTS
This study was supported by a grant from the National Research Foundation of Korea (No. 2016R1C1B1008288), funded by the Korean Ministry of Education (MOE) and the Korean Ministry of Science, ICT, and Future Planning (MSIP).