
Abstract
The aim of this study was to investigate the characteristics of headache in patients with Behçet's disease (BD) seeking neurological consultation. Consecutive patients with BD seen within 1 year at the neuro-Behçet's out-patient clinic were studied using an electronic database according to the classification criteria of the International Headache Society. During a 12-month period 118 BD patients were admitted, and 98 had headaches. Migraine was the most common type of primary headache diagnosed in 45 patients (46.4%) in the whole headache group, followed by tension-type headache (TTH) in 26 cases (26.8%). Thirty-seven patients had secondary headaches mainly due to cerebral venous thrombosis or parenchymal neurological involvement of BD. Of these patients, 15 had both primary and secondary headaches. The primary headaches of 13 patients were exacerbated with systemic BD flare-ups, and four patients had migraine attacks triggered only by systemic BD activation which showed a good response to the treatment of systemic inflammation. The majority of the headaches of patients with BD do not indicate any neurological involvement; they are usually due to migraine or TTH. In a minority of patients, migraine associated with systemic inflammation of BD is notable.
Introduction
Behçet's disease (BD) was first described by Professor Dr Hulusi Behçet (1889–1948) of the Dermatology Department of Istanbul Faculty of Medicine, in patients with recurrent orogenital ulcerations and eye inflammation (1). The aetiology of this chronic relapsing, multisystemic, inflammatory disease is unknown, and its prevalence is high in the East Mediterranean countries and Far East (2). Established diagnostic criteria include recurrent oral aphthae plus any two of the following: genital ulcers or scars; uveitis or retinal vasculitis; skin lesions such as folliculitis, acneiform lesions, or erythema nodosa; and a positive skin pathergy test (hyperreactivity of skin to pinprick) (3). Other than mucocutaneous and eye involvement, central nervous system (CNS), gastrointestinal tract, joints, blood vessels (mainly the venous side), and lungs may be involved (2). Males are affected more commonly, and when there is any serious CNS involvement this gender predilection is further pronounced; in our series with neurological involvement, the male to female ratio was 3.4 : 1 (4).
Neurological involvement is seen in about 5% of the patients with BD in large series, and shows two main distinct patterns (4). In the majority of these patients, parenchymal CNS involvement, a meningoencephalitic process involving mainly brainstem and diencephalon, is seen (5); whereas in a smaller group, occlusion of the cerebral veins and sinuses may lead to intracranial hypertension without any parenchymal signs (6).
Headache is a frequently reported symptom in BD patients with or without neurological involvement (4, 7–15). In a prospective short-term follow-up study from our department, special emphasis was given to the significance of the presence of headache, and it was concluded that migraine or tension-type headache (TTH) neither imply any CNS involvement, nor indicate any short-term risk for subsequent neurological involvement in BD patients unless accompanied by other neurological findings (7). Seven-year follow-up of the same cohort disclosed that only two of 27 patients of the primary headache group developed clear-cut neurological involvement (8). Because of the importance of neurological involvement as one of the most devastating manifestations of BD, and because of the need to treat it as early as possible, physicians should be aware of the critical points of headaches in this relatively uncommon disease. However, the classification and clues of headache syndromes according to the new criteria of the International Headache Society (IHS) (16) have not been investigated in BD.
In this study, our aim was to define the types of headache associated with BD and neuro-Behçet's disease in consecutive BD patients seeking neurological consultation.
Patients and methods
All consecutive patients with BD admitted to our clinic during a 12-month period were included in this study. A careful history of headache was taken by the authors and was recorded in an electronic database with the patients’ consent. This database included all questions required by the criteria of the IHS (16).
Additional inclusion criteria were as follows: the patients should meet the criteria for BD, established by the International Study Group for BD (ISGBD) (3), they should have at least one follow-up visit (telephone visits were also acceptable if an initial out-patient visit in cases with sufficient information about headache and BD features was present), and they should have completed all the essential neurological investigations such as magnetic resonance imaging (MRI) and lumbar puncture, when indicated to clarify the neurological status.
The following parameters were evaluated: gender, current age and ages at onset of BD, of neuro-Behçet's disease, and of headache, characteristics of all present and past headache disorders such as duration, frequency, associated symptoms, quality, localization, relationship with other symptoms of BD (at the time of headache episodes concurrent presence of any out of: oral aphtae, genital ulceration, uveitis, erythema nodosum, folliculitis or other skin lesions), headache diagnoses, past history and family history for headache and BD, types of neurological involvement established by laboratory data [such as MRI and cerebrospinal fluid (CSF) findings]. Recent use of colchicine, corticosteroids, non-steroidal anti-inflammatory drugs (NSAIDs) and immunosuppressive medications and their effects on the headache were carefully asked for and recorded. Physical examination and routine blood chemistry of the patients were evaluated to disclose relevant organ involvement or any concurrent diseases.
The findings of these patients were compared with those of other patients with headache admitted to our headache out-patient clinic in the past 2 years which were evaluated by the same team.
At the end of the recruitment period, all clinical and laboratory data of BD patients as well as of control patients were evaluated in joint sessions by the authors to classify their headaches according to the new IHS criteria (16). Secondary headache diagnoses were applied when a patient developed a new type of headache, in close temporal relation to the clinical onset or a new attack of neuro-Behçet's disease, or with an accompanying abnormal laboratory finding such as MRI, MR-venography, conventional angiography, or CSF findings, compatible with a neurological picture known to cause headache.
Statistical analysis
The findings of BD patients and the patients of the headache out-patient clinic were compared, as well as the subgroups of BD patients with and without neurological involvement and those with primary vs. secondary headache disorders. Student's t-test was used for parametric comparisons, and χ2 or Fisher's exact test were used for non-parametric comparisons.
Results
A total of 118 BD patients, meeting the ISGBD criteria (3), were seen within 12 months, and 98 (83%) complained of headache. We excluded one patient whose history was equivocal and could not be contacted later. The remaining 97 patients (54 F, 43 M, mean age 37.4 ± 11.2 years) were evaluated for headache characteristics. Brain MRI was performed in 69 patients and CSF examination was done in 43 patients. The control group included 479 patients who were admitted to our general headache out-patient clinic during the last 2 years (345 F, 134 M, mean age 35 ± 11.8 years). Of these, 388 patients with a definite diagnosis of migraine and/or TTH comprised the control group for primary headaches.
Based on the new IHS classification (16), 37 patients (24 M, 13 F) (38.1%) had secondary headache disorders (Tables 1 and 2). In this group, 32 patients had headaches associated with the neurological involvement of BD. Fifteen of these (8 M, 7 F, mean age 24.5 ± 8.1 years) had dural sinus thrombosis evidenced by neuroimaging, leading to subacute, diffuse, severe, progressive headache (median duration 60 days). In nine out of 15 patients, headache showed worsening at night or upon awakening and partially resolved during the day. The headache resolved within 1 month after appropriate treatments in 1/3 of them, and within 3 months in all patients. Nevertheless, we grouped these 15 patients under IHS-6.6 ‘Headache attributed to cerebral venous thrombosis’ (16). In two other patients, intracranial hypertension was documented, but we could not demonstrate cerebral venous thrombosis. On the other hand, in 15 other patients (11 M, 4 F, mean age 30.5 ± 9.9 years) parenchymal CNS involvement of BD was the cause of headache (classified under IHS 7.3.3). In these cases, there was a progressive, moderate to severe headache of subacute onset accompanying a florid neurological picture with hemiparesis, behavioural change, ataxia or brainstem signs. The duration of the headache varied between 1 and 15 days (median 3 days, mean 5 days). These patients had either cranial MRI showing extensive involvement of the brainstem, diencephalon or basal ganglia region (n = 11), and/or abnormal CSF revealing pleocytosis (n = 10) at the time of headache. Finally, five patients had secondary headaches due to rare coincidental causes such as infectious meningitis, subarachnoidal haemorrhage and sinusitis. Besides the secondary headache disorders, 15 patients of this group also had primary headache disorders (Table 1).
Demographical characteristics and classification of headaches in patients with BD

BD, Behçet's disease; F, female; ICH, intracranial hypertension; M, male; PSH, primary stabbing headache; SAH, subarachnoid haemorrhage; TTH, tension type headache.
Characteristics of the headache symptoms in primary vs. secondary headaches in BD

BD, Behçet's disease; DST, dural sinus thrombosis; TTH, tension-type headache.
This table excludes those patients with both primary and secondary headaches for convenience.
Statistically significant differences between total primary and total secondary groups as calculated by Fisher's exact test; P-values in order: 0.01; 0.001; <0.001; 0.002; <0.001; 0.004.
Seventy-five patients (26 M, 49 F) had primary headache disorders (77.3%). Migraine (IHS 1) was the most common type of primary headache with a rate of 46.4% in the whole headache group, followed by TTH (IHS 2) with a rate of 26.8%. Only three of the 45 patients with migraine had migraine with aura (IHS 1.2, 7%), which is less than in the control group (51/326; 15%), without reaching statistical significance, however. One of these patients had migraine with typical aura (IHS 1.2.1), another one had familial hemiplegic migraine (IHS 1.2.4) and the last patient had typical aura with non-migraine headache (IHS 1.2.2) and some attacks of typical aura without headache (IHS 1.2.3). Chronic migraine (IHS 1.5.1) without medication overuse was diagnosed in three patients in the migraine group. Medication overuse headache (IHS 8.2.3) was found in only one case due to simple analgesics. Two cases had primary stabbing headache (IHS 4.1) (Table 1).
Comparisons of headache characteristics of the groups with secondary and primary headache disorders are summarized in Table 2. Aggravation of headaches in the morning was significantly more frequent in the group with secondary headaches compared with the group with primary headaches (P < 0.004). Female patients predominated significantly in the group with primary headaches, whereas males predominated among cases with secondary headcaches (P = 0.0043). There were no differences in the family history of primary headaches in BD and control groups. The headache had begun after the onset of BD in 42 of 60 patients in this group. The characteristics of their headaches were not different from those of the control group when compared regarding age at onset or headache characteristics.
Thirteen patients of the group with primary headache disorders described an exacerbation of their migraine or TTH during the presence of any systemic BD finding (Table 3). Four patients of this group (4% of the whole group) had migraine attacks triggered only by oral or genital ulcers, or uveitis, which showed a good response to treatment of systemic inflammation (Table 3). Their MRIs and CSF examinations were normal at the time of the headache attacks.
The relationship between systemic BD flare-ups and primary headaches
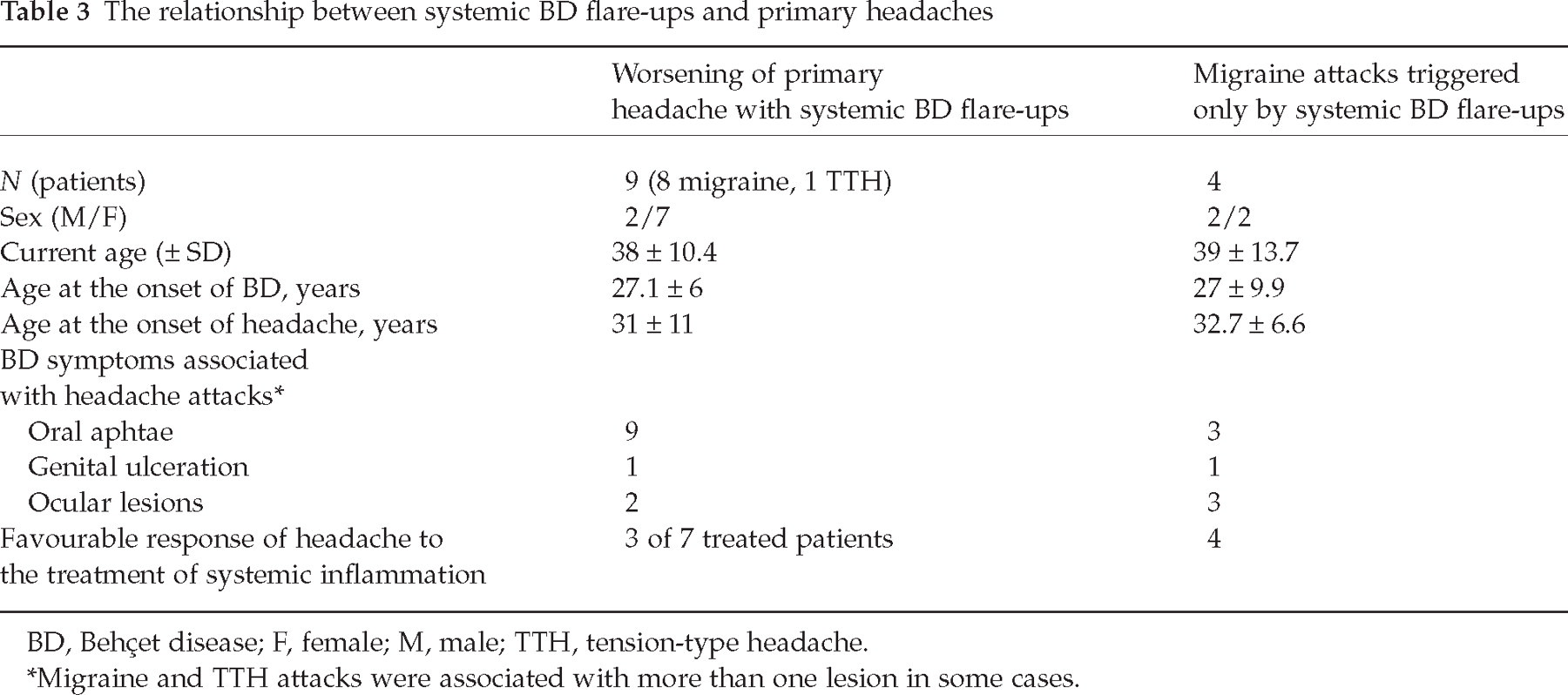
BD, Behçet disease; F, female; M, male; TTH, tension-type headache.
Migraine and TTH attacks were associated with more than one lesion in some cases.
The distribution of various symptoms of BD, such as oral aphtae, genital ulceration, erythema nodosum, folliculitis or organ involvement, did not differ between the groups with primary and secondary headache disorders. Vascular involvement and uveitis were seen significantly more often in patients with secondary headaches (P = 0.001, and P = 0.01, respectively), whereas a history of arthralgia/arthritis was reported more often by patients in the primary headache group (P = 0.02).
The relationship between headaches and treatment for BD revealed that only seven out of 34 patients treated with steroids reported a positive effect on the primary headache. There were no differences in BD treatment protocols between the group without headache and those with secondary headaches, but most of the primary headache patients were not treated with steroids and immunosupressive agents. NSAIDs were used in a substantial number of the patients for other causes, without inducing medication overuse headaches. In one of the migraine patients, cyclosporin had induced a clear increase in headache frequency (development of daily headaches from baseline of one to two attacks per month) and shortening of headache duration (attacks of 10 h replaced by attacks lasting <1 h) with the same migrainous characteristics. The presence of a psychiatric diagnosis did not differ among the groups.
Discussion
Given the diversity of causes that produce headache in a multisystemic disorder such as BD, a systematic approach to the diagnosis is essential both for management and research purposes. We therefore used the IHS criteria, second edition, in our study, which classifies headache disorders as primary and secondary (16). The diagnosis of primary headache requires the exclusion of any other disorder that might be the cause of the headache. Diagnosing a secondary headache in a patient with a preexisting primary headache is also somewhat challenging. In case of BD, a relatively uncommon disease with a set of clinical diagnostic criteria without any specific laboratory finding, this difficulty increases further.
We found that headache is a frequent symptom, as it was seen in 98 BD patients out of 118 patients who were admitted to a neurology clinic. This rate is higher than the headache prevalence reported for the general Turkish population (64.7%) (17), but similar to or lower than some reports dealing with headache in BD (11, 12). Monastero et al., in a small group of 27 patients, reported a prevalence of 88.9% (12) and Kidd found an even higher prevalence (92%) in a large cohort studied with questionnaires (11). However, most of these, like ours, were neurology-based cohorts, which might have a selection bias. Saip et al. reported recently a headache prevalence of 66.2% in a study population from a multidisciplinary out-patient clinic for BD (15), which might better reflect the prevalence of headaches in a BD population.
Intracranial hypertension due to dural sinus thrombosis is one of the important reasons for subacute progressive headache in BD and its prognosis is generally favourable (4, 6, 14, 18). We noted a difference in our BD group with regard to section 6.6 of the IHS classification (16), since this type of headache usually resolves after 2 or 3 months, but not after 1 month as indicated in the IHS classification. The secondary headache group also includes patients with parenchymal involvement of BD. We consider that these patients could in all probability be classified under IHS 7.3.3 ‘Headache attributed to other noninfectious inflammatory disease’ (16). In these cases, neuroimaging data and CSF findings should be used for accurate diagnosis (9).
As mentioned in previous studies (7, 14), we found that most of the patients (77.3%) describe primary type headaches such as migraine and TTH. It is interesting to note that there was a significant female predominance of patients with primary headaches, although BD is well known for its marked male predilection, in general and as well as in cases with neurological involvement (Table 1). Although migraine or TTH may begin after the onset of BD in some patients, the characteristics of these headaches did not show any difference from the headache out-patient clinic population. It should be noted that both BD and primary headache disorders have their onset in young adulthood, therefore the ages of onset of primary headaches and of BD could show any such intersection.
Migraine with aura was less frequent in the BD group compared with the control group, although not statistically significantly so in our large cohort. Such an observation was also reported by the small series from Italy (12). On the other hand, migraine with aura was found more frequently in another large cohort from the UK (10, 11). In the latter study, a headache questionnaire was sent to the patients. This investigation technique can sometimes be unreliable in headache diagnosis. Other than a methodological issue, there may also be some ethnic differences between the two large cohorts investigated.
Systemic lupus erythematosis (SLE) is another multisystemic inflammatory disease that may show some similarities to BD. The problem of headaches in SLE also poses a dilemma. A meta-analysis of headaches in SLE reports that the prevalence of either migraine or TTH was not different from controls and no particular pathogenic mechanism of headache in SLE patients was identified (19). Their conclusion regarding headache in SLE was in parallel with our conclusion in BD and indicated that the occurrence of headache in SLE patients does not require further investigation per se, and that headache in those patients could be classified according to IHS criteria if there is no other associated symptom of neurological involvement (19).
Evaluation of headache is difficult and a correct diagnosis is crucial, since secondary causes of headache in BD, especially parenchymal neuro-Behçet's disease, may be devastating. Our study shows that primary and secondary headaches in BD may be difficult to distinguish in terms of character or duration, although clear clues exist regarding the evolution of headache and accompanying neurological symptoms in headaches associated with neurological involvement. These may require careful diagnostic work-up (MRI, CSF analysis), or removal of medications to exclude those causes not directly related to neuro-Behçet's disease. The presence of headache should not precipitate aggressive corticosteroid or immunosuppressive therapy unless other more reliable markers of neurological involvement are present (9). Thus, lumbar puncture should be considered early if the headache is atypical or persistent.
We demonstrated that 13 patients with migraine and TTH showed worsening of their headaches when there was any systemic BD flare-up, such as an oral or genital ulcer, skin lesion, or uveitis. We also emphasize that four patients noted that recurrent migraine attacks are triggered only by such activation. These headaches were rare (4% of the whole group) and responded to treatment of the systemic inflammation (Table 3). We investigated this confusing group extensively, including cranial MRIs and CSF examinations; however, no other signs of neurological involvement could be demonstrated at the time of the headache attacks. Whether this interesting group represents an extraordinary primary headache disorder as classified in the current study, or a rare and new type of secondary headache disorder due to systemic inflammatory changes in BD, remains to be clarified. The known predilection of BD to brainstem involvement, a localization with a proven role for migraine as well as the established silent neurological involvement (4), make this discussion more challenging.
We did not systematically study the treatment of primary headache attacks in the group, but our experience suggests that established prophylactic agents like tricyclic antidepressants or valproate are effective for prophylaxis and simple analgesic drugs combined with metoclopramide are effective for acute attacks of primary headaches in BD. Since patients with BD have a tendency to major thrombotic events, the clinician should be reluctant to prescribe triptans or, at least, reserve them for the unresponsive patients. Further prospective studies are needed for the treatment of headache in BD patients.
We conclude that patients with BD and headache should be systematically assessed for accurate diagnosis, but the majority of the cases are not related to neurological involvement. In a minority of BD patients, migraine-like headache associated only with systemic inflammation of BD is notable. Since this study included only those cases that sought neurological consultation, our methodology does not allow further conclusions concerning the prevalence of headaches or primary headache disorders among BD patients, or concerning any relationship it may have to the pathophysiology of the disease. We believe that it is worthwhile to assess such issues in further prospective studies.
Footnotes
Acknowledgements
We thank Dr Piraye Serdaroglu, the founder of the neuro-Behçet out-patient clinic in our department, and to Dr Edip Aktin for their inspiration. We also thank Drs Ahmet Gul, Hasan Yazicí, Murat Inanc, Ilknur Tugal-Tutkun, Gulsevim Azizlerli and Afet Akdag-Kose for referring their BD patients to our department for neurological evaluation. This work was presented at the 11th International Congress on Behçet's Disease (2004, Antalya, Turkey).