
Abstract
Background:
Parkinson’s disease (PD) and frailty are two conditions that are increasingly common with advancing age, yet little is known about their relationship.
Objective:
The aim of this study was to examine the co-occurrence of frailty in people with PD; to describe the measures used to assess frailty in PD, and assess the prevalence of frailty in subjects with PD.
Methods:
We conducted a systematic review of Pubmed and Embase in April 2018. Studies that assessed frailty in subjects with PD were included in the review and data was extracted on the prevalence of frailty in subjects with PD. Due to heterogeneity of studies a meta-analysis was not performed.
Results:
Eight studies were included in the review, of which 7 were cross-sectional and 1 a prospective cohort study. Mean age of participants with PD in the studies ranged from 66 to 85 years. The majority (6/8) used the 5-item, Fried criteria to measure frailty, with the remainder using index-based measures. 5 studies provided data on the prevalence of frailty in PD, which ranged from 29% to 67%.
Conclusions:
Few studies have quantified the prevalence of frailty in PD, but those that have suggest a high concurrence of these two conditions.
INTRODUCTION
Parkinson’s disease (PD) and frailty are both highly prevalent in older people. Despite the frequency with which both conditions are encountered in clinical practice, the coexistence, overlap and potential interaction between the two states has not been fully explored. The topic of frailty remains complex, not least as the term ‘frailty’ is ambiguous and has eluded a consensus definition [1].
Frailty is recognised as a state of increased vulnerability and loss of resilience to stressors [2], which, in turn, confers an increased risk of disability and death. A combination of inflammatory, hormonal, and nutritional changes are associated with frailty, and have been suggested as key factors in its pathogenesis, although more research is needed to confirm a causal link [3]. The manifestation of frailty is such that a critical tipping point exists whereby reserve has been diminished to such an extent that an individual cannot adapt to physiological change and homeostatic balance is disrupted. Physical frailty is also known to be related to cognitive impairment, leading to the recently defined condition of “cognitive frailty” [4].
The operationalisation of the frailty concept varies, but two principal approaches have been adopted for use in clinical studies. Firstly, a clinical phenotypic model, first proposed by Fried [5] suggested that an individual is frail in the presence of three or more of five criteria; weakness, weight loss, slow walking speed, fatigue, and low physical activity. Conversely, an alternative index-based approach was first described by Rockwood and Mitniski [6], whereby the accumulation of multiple deficits of symptoms, disability and disease, contribute to an overall burden of frailty.
Advancing age coupled with PD are not inevitable antecedents of frailty. Albeit less commonly, frailty can be encountered in the absence of overt comorbidities. However, the impact of both non-motor and motor symptoms in PD may well ‘fuel’ a frailty syndrome, whereby the combination of factors confers an accelerated and augmented risk of negative outcomes. Factors such as fatigue, gait and balance impairment, cognitive changes, polypharmacy and adverse drug reactions all contribute to functional impairment when carrying out activities of daily living, and these feature almost invariably in older frail adults.
The objective of this study was to systematically review the literature to a) describe studies that have examined frailty in people with PD, b) describe the current measures used to assess frailty in PD and c) determine the prevalence of frailty in PD.
METHODS
Search strategy and selection criteria
This systematic review was designed and reported within the PRISMA framework – the study protocol was not published, but is available on request. A systematic search of Medline (Pubmed) and Embase was performed from the start of the database to 4th April 2018, and was conducted in line with the Meta-analysis of Observational Studies in Epidemiology (MOOSE) criteria. The search strategy included MeSH Terms and keyword variations (see the Supplementary Material for full search strategies), to identify all studies investigating frailty in patients with PD. The following strategy was used in the Pubmed database: (“parkinson disease”[MeSH] OR “parkinsonian disorders”[MeSH] OR parkinson*[tw]) AND frail*[tw]. The search was limited to English-language publications.
Studies were included if they satisfied the following criteria: a) population: enrolled subjects with a diagnosis of PD. Populations with patients with parkinsonian symptoms, but without formal PD diagnoses were excluded. b) outcome: measured frailty, assessed using a formal operationalised measure, such as the Fried criteria or Rockwood frailty index. Studies that defined frailty according to a measure of functional impairment (e.g., the ability to perform activities of daily living) or in a non-objective, non-standardised manner, were excluded.
Reviews, editorials, case studies and conference abstracts were excluded. Two reviewers (N.S., L.B.) evaluated each abstract for inclusion according to these criteria, and of selected abstracts, full publications were then obtained and reviewed in detail by the same two independent reviewers.
Data extraction and quality assessment
After inclusion, the following information was extracted from each study to a data extraction form: study date, sample size, demographic characteristics of subjects, number of people in the sample with PD, the frailty measure used and findings regarding frailty (principle measure being frailty prevalence). Study authors were contacted when required to provide further information.
The methodological quality of included studies was judged based on an adapted version of the Newcastle – Ottawa Scale [7] (NOS). This rating scale was developed to assess the quality of non-randomised studies in meta-analyses, and scores studies based on 3 domains: on the selection of the study sample; the comparability of groups and control of confounding factors; and outcome measurement. We assigned studies up to a maximum of 8 points based on this scoring system. The original NOS was developed for use with case-control and cohort studies, we adapted it to also apply it to cross-sectional studies, in line with previous research [8, 9].
In the case of multiple studies drawing on the same cohort, data was drawn from the study that included the largest number of participants, and had the best NOS score. Two authors (N.S., L.B.) independently extracted the data, and scored the studies quality. Any differences were resolved by discussion, and referred to a third researcher (E.H.) when required.
Data synthesis
Due to heterogeneity of the studies – including differences in population, frailty measure used and study design – a meta-analysis was not performed on the outcome of frailty prevalence in PD. Results of our data extraction were instead synthesised in tabular, graphical and narrative form.
RESULTS
The search yielded 116 articles in PubMed, and 241 in EMBASE. Reference lists of included studies were hand-searched for any further studies, which yielded 1 additional article. The initial literature search therefore yielded 358 results and after removing duplicates, 256 remained. Of these, 230 were excluded at the initial screening of abstracts, and 17 more were discarded after detailed review, for failing to meet the inclusion criteria (see Fig. 1 for PRISMA flowchart). One further paper was excluded at a later stage after authors were unable to provide data for PD subjects [18]. 8 papers remained for data extraction (see Table 1) [10–17].
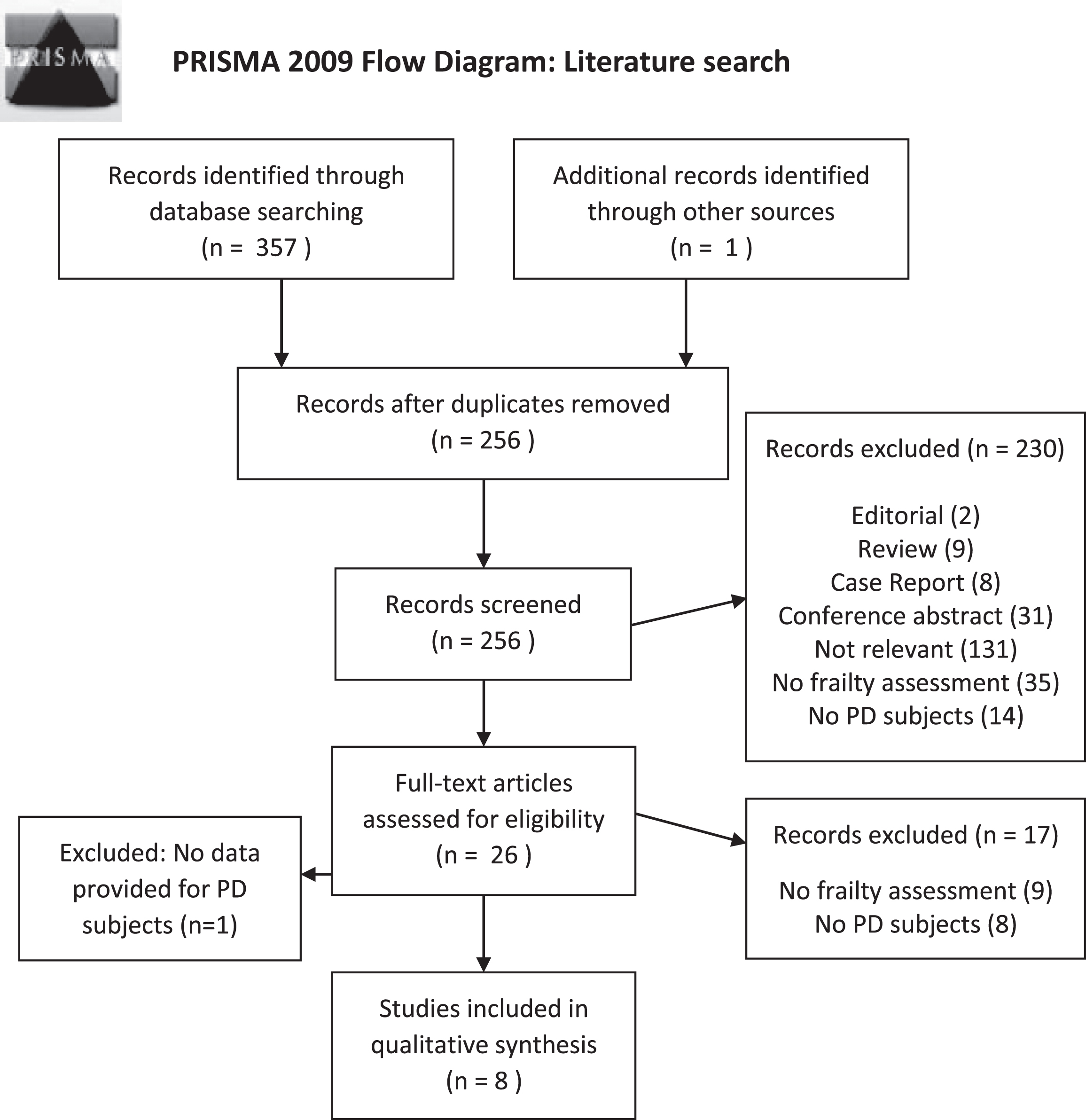
PRISMA flowchart of included studies.
Characteristics of studies included in review
PD, Parkinson’s disease; SD, standard deviation; Quality Score, Newcastle Ottawa Scale score; P, population; C, clinical; Fried, California Health Study Frailty Index, (Fried criteria); *adjusted version of Fried criteria; FGE, Functional Geriatric Evaluation questionnaire; TFI, Tilburg Frailty Indicator; H&Y, Hoehn & Yahr Scale; cogn intact, cognitively intact; **PD-specific age and gender information not provided, so age/gender figures used for overall sample.
Of the 8 papers analysed, 7 were cross-sectional studies [10–16], and 1 a prospective cohort study [17].
Correspondence with authors revealed that the same cohort of PD participants was used for four of the cross-sectional studies [10–13]. These studies were assessed separately and all included in the descriptive review, but data for frailty estimates was only extracted from one [13].
The authors of one large prospective cohort study [17] provided further unpublished data. In view of the different study design we utilised the last available frailty status of the participants to calculate the cumulative risk of frailty over time. We are aware that these risks therefore does not constitute a “true” prevalence figure, and therefore chose to present them separately to the data from the cross-sectional papers.
Methodological quality
The detail of the methodology in the extracted papers varied, and was often limited. Seven of the 8 studies scored moderately on the NOS, with only one paper scoring less than 4 (see Table 1). The studies were weakest in their sample selection, with 6 of the 8 papers scoring only 1 or 2 points in this domain (out of a possible 4). This was generally due to studies having small samples that were often not representative of the average PD patient, with samples ranging from 13 up to 74 subjects. Few studies justified their sample size, and many omitted information on response rate or non-responders. The studies performed better on comparability and outcome – only 2 studies did not control for key factors when analysing outcomes, and 7 out of 8 papers scored full marks on the assessment of frailty. Of the 5 studies from which frailty data was extracted, overall NOS scores ranged from 4 to 8, with an average score of 5.8 (see Supplementary Table 1 for full breakdown of scores).
Population
The majority (7/8) of the studies sampled patients from the general population, as opposed to a clinical cohort from, e.g., a secondary care population. Three cross-sectional studies exclusively recruited patients with PD [10, 14] and two recruited PD patients as well as matched controls [11, 13]. The prospective cohort study included up to 74 people with PD, from having sampled a large cohorts of older people [17]. PD participants were sampled throughout the course of their disease, from those living independently in the community [10–16], to those with more advanced disease and comorbidity, including some residing in institutions [17].
Classification of frailty
Most of the studies used the Fried frailty criteria [10–14] or a variation thereof [17] as a measure of frailty. The five criteria included were weight loss of > 10 lbs in the past year, maximal hand-grip strength, time to walk 15 feet at usual pace, self-reported inactivity, and self-reported exhaustion [10–14]. 1 point is scored for each positive feature. Consequently, patients were stratified as non-frail (score 0), pre-frail (score 1-2), or frail (score≥3). Most of the papers [11, 14] operationalised self-reported exhaustion by using two questions from the Center for Epidemiologic Studies Depression Scale (CES-D). Self-reported activity was quantified in kcals using the Minnesota Leisure Time Activities Questionnaire (MLTA), as per the original criteria [13] or this was modified and an exercise log was completed [14]. One paper [17] used a modified version of the Fried criteria summarising the four components of grip strength, 8 feet timed walk, BMI and fatigue (CES-D) in a composite measure.
Two studies [15, 16] utilised index-based approaches to measure frailty according to the accumulation of deficits. Both used questionnaires to gather responses on physical, mental and social domains – one using the Functional Geriatric Evaluation questionnaire (FGE) [15], and the other part of the Tilburg Frailty Indicator (TFI) [16]. These assessments were used to calculate overall scores, from which frailty categories were derived.
Prevalence of frailty in PD
Five studies provided data for the number of frail people in a group of PD subjects [13–17]. There was some evidence for heterogeneity of the prevalence estimates (I2 = 63%, p = 0.04) and these ranged from 29% to 67%, shown as a Forest Plot in Fig. 2. The wide range of these estimates is likely partly due to the different frailty measures employed. The three studies that used the Fried criteria described a frailty prevalence of 29–33% in PD subjects, whereas the estimate was higher in the studies utilising index-based measures (50% to 67%).
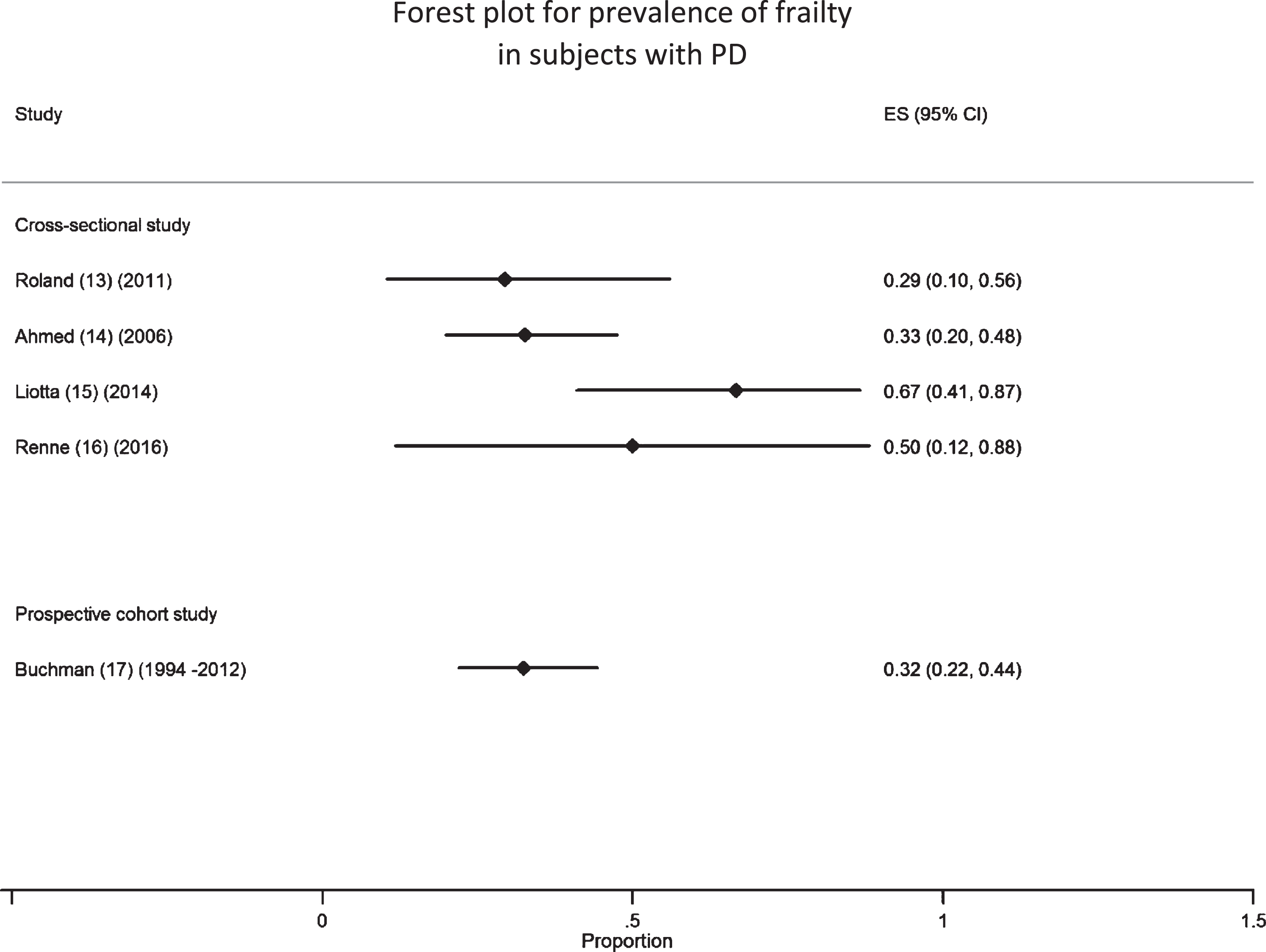
Forest Plot for prevalence of frailty in subjects with PD. Studies displayed by mean participant age in ascending order.
Predictors of frailty status
Four studies examined individual components of the 5 Fried frailty criteria, to assess which factors were best able to differentiate between frail and non-frail PD subjects. Studies were contradictory in respect to whether or not activity levels were associated with frailty status. Two of the studies papers [10, 11] found that neither self-reported activity nor objectively measured physical activity were related to overall frailty in the PD participants, in contrast to findings from non-PD cohorts. However, Roland et al. identified self-reported exhaustion as a strong predictor of frailty in PD subjects in one small study (R2 = 0.44) [12].
In contrast, Ahmed et al. [14] examined the five Fried criteria and found activity (measured as weekly calorific expenditure) to be the best discriminator between frail and non-frail PD subjects (OR 22; p < 0.001). Of the remaining Fried criteria, grip strength, walk time and exhaustion were all also significantly associated with frailty status, with only weight loss forming an exception. Ahmed et al. also examined the factors as continuous variables, noting that grip strength no longer differed between frail and non-frail, whereas walking time was significantly lower in the frail group (p < 0.001).
Frailty and PD severity
Five studies reported that higher frailty scores (using the Fried model) were associated with markers of disease severity in PD subjects. Three studies by Roland et al. described that those that were frail took higher doses of dopaminergic drugs [10], with two [11, 13] reporting that levodopa dose was significantly associated with frailty status (r = 0.61; p = 0.01). However, we cannot be certain if dopaminergic dosage and frailty are directly associated, or if the observed relationship can likely be explained by disease severity affecting both frailty and drug dose. Two studies similarly noted that frail subjects had more advanced disease, quantified using the Hoehn and Yahr scale [12] or the Unified Parkinson’s Disease Rating Scale (UPDRS) [14].
Associations between frailty, PD, and outcomes
One study examined other outcomes in a PD population, finding an association between worse quality of life scores and higher frailty (R2 = 0.12; p = 0.02) as well as higher odds for frailty in females (OR 9.8; CI 1.0–93.5) [12]. Frail subjects were also noted in one paper [10] to have lower scores on the Berg Balance Scale compared to non-frail individuals (20 vs 25.3; p = 0.04).
DISCUSSION
To the best of our knowledge, this is the first systematic review of frailty in PD. Notably, whilst frailty and PD are both highly prevalent in older people, we only identified 8 papers that had systematically and concurrently quantified these two conditions.
Our main findings show that frailty is highly prevalent in individuals with PD, with the estimates of frailty prevalence we found lying above the average frailty expected in a non-PD population of similar age [19].
The majority of studies operationalised frailty using the original or a modified version of the criteria proposed by Fried in the Cardiovascular Health Study, demonstrating that the criteria can be operationalised in people with PD. These criteria can be criticised from a reductionist perspective as simple outcomes that fail to recognise the complex psychosocial aspects of the frailty syndrome. Moreover, in the Cardiovascular Health Study, people with PD were excluded [5]. Two of the Fried criteria form some of the recognised non-motor symptoms of PD, namely fatigue and weight loss [20]. Since one of the other five Fried criteria, slow walking speed, is also a key feature of PD, the Fried measure may actually risk over diagnosing frailty in a PD population, by attributing their slow walking to frailty rather than their PD. Analysing these criteria as continuous variables rather than dichotomising them, as Ahmed et al. did in part [14], avoids loss of data.
Alternatively, these Fried outcomes could be viewed as common endpoints arising from complex and varied underlying pathology. The more comprehensive approach advocated with an index-based approach, as used in two papers [15, 16], may better capture deficits in multiple domains and reflect the complexity of a frailty state. Whilst the full index based approach may be difficult to operationalise in day-to-day clinical practice, the introduction of the visual Clinical Frailty Scale derived from the frailty index is validated for use in clinical settings [21] and offers scope to apply this to future cohorts. Critically, neither measure has been validated in a PD population with respect to predicting outcomes.
Limitations of this review include the small number of papers included, which reflects the scarcity of research on this subject. Of note, one study also met our inclusion criteria but we were unable to extract data for our subsequent analysis, as it was not possible to gain information specific for PD subjects from the paper, and we were unsuccessful in obtaining the required information from the authors [18]. Small sample sizes may have resulted in a Type 2 error whereby significant associations were incorrectly rejected, and we may have been underpowered to detect significant results. By including a spectrum of studies, from large population-based cohorts to smaller cross-sectional studies, we captured patients with different durations of PD. However, the heterogeneity of participant characteristics between different studies mean that the findings from studies of ambulant, independent PD subjects may not necessarily apply to those with more advanced disease. As well as significant variation in PD disease duration, differences in age and gender are likely to impact the frailty prevalence seen. We chose not to perform a meta-analysis of these studies, due to our acknowledgement that the heterogeneity of these papers and their limited number would impede an appropriate meta-regression analysis.
PD and frailty are both conditions of older people. Given the established association between frailty and vulnerability to negative clinical outcomes, recognition of these concurrent conditions may help target modifiable factors that improve overall prognosis. It remains to be delineated whether the two conditions share a pathophysiological basis and if so to what extent this shared aetiology can be targeted with intervention. Future studies will need to delineate the strength of the association between disease factors, the presence of frailty and age on physical and psychosocial outcomes, and mortality. However in current day-to-day clinical practice, recognition of frailty in those with PD should enhance targeting of treatment and, perhaps more importantly, discussion around future prognosis and care planning. We propose that PD is an archetypal frailty syndrome and future research will improve recognition of the syndrome in this vulnerable population to better inform treatment decisions as well as prognosis.
Key Points
•This systematic review found 8 studies that had measured frailty in subjects with PD
•Estimates of frailty prevalence lay between 29–67% depending on frailty measure used
•This emerging area warrants careful measurement in order to appropriately target interventions in this vulnerable population
CONFLICTS OF INTEREST
The authors have no conflict of interest to report.